
Abstract
Background
Compared to total knee arthroplasty (TKA), patellofemoral arthroplasty (PFA) is a far less commonly performed operation. However, in carefully selected cohorts, PFA continues to be an appropriate treatment option for end-stage isolated patellofemoral joint osteoarthritis. In the later situation whereby a PFA is considered for conversion to a TKA – often due to disease progression – uncertainty remains regarding optimal management of the in situ patellar button. This review of the contemporary literature aimed to provide a summary of the current evidence to support surgeon decision-making, by evaluating the compatibility, efficacy, and survivorship of retained versus revised patellar buttons in PFA-to-TKA conversion. Specific focus was paid to implant design and technical considerations during revision, plus post-operative patient-reported outcomes and modes of secondary patellar component failure.
Methods
A review of the Embase, Cochrane and PubMed databases was performed following PRISMA search principles.
Results
This investigation highlights that the fate of patellar buttons in PFA-to-TKA conversion has previously been poorly studied, with scant publication data available. Most reports have been of singular cases or small cohort series. Larger formal RCTs and level 1 evidence are lacking.
Conclusion
The findings herein suggest that surgeons can confidently retain well-fixed, undamaged, dome-shaped all-polyethylene patellar buttons in the conversion of a PFA to TKA with the expectation of acceptable mid-term performance and survivorship, as long as congruent tracking with the new tibiofemoral components is achieved. This result is likely translatable to the majority of contemporary, all-polyethylene, dome-shaped patellar buttons, even with manufacturer mismatch.
Introduction
Patellofemoral arthroplasty (PFA) can be a successful treatment for debilitating isolated patellofemoral joint osteoarthritis (OA) in a selective patient population who have failed optimised non-operative or less invasive surgical measures. A recent systematic review found that the overall prevalence of isolated patellofemoral arthritis is 7% in community-based populations and 19% in symptomatic cohorts. 1 A selective PFA remains a viable surgical option that may otherwise preserve healthy or unaffected tibiofemoral compartments. It has been suggested that unicompartmental knee replacements (including PFAs) may more closely resemble native knee kinematics in comparison to TKA. 2 However, disease progression in the remaining native compartments, incorrect patient selection, 3 focal pain and implant failure or wear can result in patients subsequently seeking conversion of their PFA to a TKA.
The use of PFA remains relatively low as illustrated by international joint registries, constituting only 1.2% of primary TKAs in the United Kingdom, 4 0.1% in the United States 5 and less than 0.5% in Australia. 6 Given infrequent use, there exists a paucity of credible information to support surgeon decision-making with regard to both the technical aspects of PFA-to-TKA conversion and the longer term results. A few heterogenous smaller studies have previously suggested a relatively straightforward procedure technically, with clinical outcomes comparable with primary TKAs.7–9 However, others have suggested less favourable outcomes (i.e. more comparable to TKA revision results).10,11 As a critical intrinsic omission, these studies often provide limited information with regard to the compatibility and ultimate survivorship expectancy of the original patellar button when converting to a TKA.
This structured review aimed to provide a concise insight into, and summary of, the contemporary understanding of patellar button designs used in primary PFA, key considerations in determining component retention versus revision and technical factors relevant to the revision process, in order to support surgeon decision-making in PFA-to-TKA conversions. We also explore the available data regarding the performance and survivorship of the patellar component after revision to a TKA.
Search strategy and selection criteria
To ensure a relevant, accurate and representative synopsis of the current state of understanding of the role of patellar button retention versus revision in the conversion of PFAs to TKAs, a structured and systematic search and retrieval of publications was performed according to the accepted Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Search criteria: The search results are depicted in Figure 1. Three databases, (i) Cochrane, (ii) EMBASE and (iii) Medline were searched from inception until 20 September 2021. Search results were limited in the first instance to articles available in the English language with available abstracts. PRISMA search summary. * Mon Sept 20 10:22:10 2021 Search: [(patellofemoral arthroplasty OR patellofemoral replacement) OR (PFA OR PFR)] OR [(total knee arthroplasty OR total knee replacement) OR (TKA OR TKR)] AND (patellar component OR patellar button) AND (conversion OR revision OR retention) AND (English\[Language]).
Inclusion criteria: The following MESH terms were used: ‘[patellofemoral arthroplasty OR patellofemoral replacement] OR [PFA OR PFR]’, ‘conversion OR revision OR retention’, ‘[total knee arthroplasty or total knee replacement] OR [TKA OR TKR]’ and ‘patellar component OR patellar button’. Titles and abstracts of identified records were screened to exclude obviously irrelevant studies. Articles that described the concept of patellofemoral arthroplasty, and/or specifically the conversion of PFA to TKA were reviewed to extract data when available on PFA implant design, reasons for and rates of revision or retention of the patellar component in situ, and patellar component and patient-reported outcome measures (PROMs) at follow-up after revision to TKA. No limitations were placed on age, gender, date, study design or length of follow-up. The bibliographies of relevant papers were manually reviewed to identify further studies, with additional data sourced from international joint registries.
Exclusion criteria: Articles were excluded if they did not specifically analyse PFA-to-TKA conversion or patellar button survivorship, or if no full-text in English language was available. Individual case reports or cohort series containing outcome data for less than five patients were also omitted from the principal analysis.
Quality of studies: The quality of principal studies identified was determined using the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) method. 12 Using this approach, studies were evaluated for study design, severity of limitations, consistency, directness and other modifying factors. Depending on the scores using the GRADE criteria, the overall quality of studies was determined to be high, moderate, low or very low. In addition, the level of evidence of studies was determined using the adjusted Oxford Centre for Evidence-Based Medicine 2011 Levels of Evidence. 13
PFA revision to TKA
Principal studies included for review.
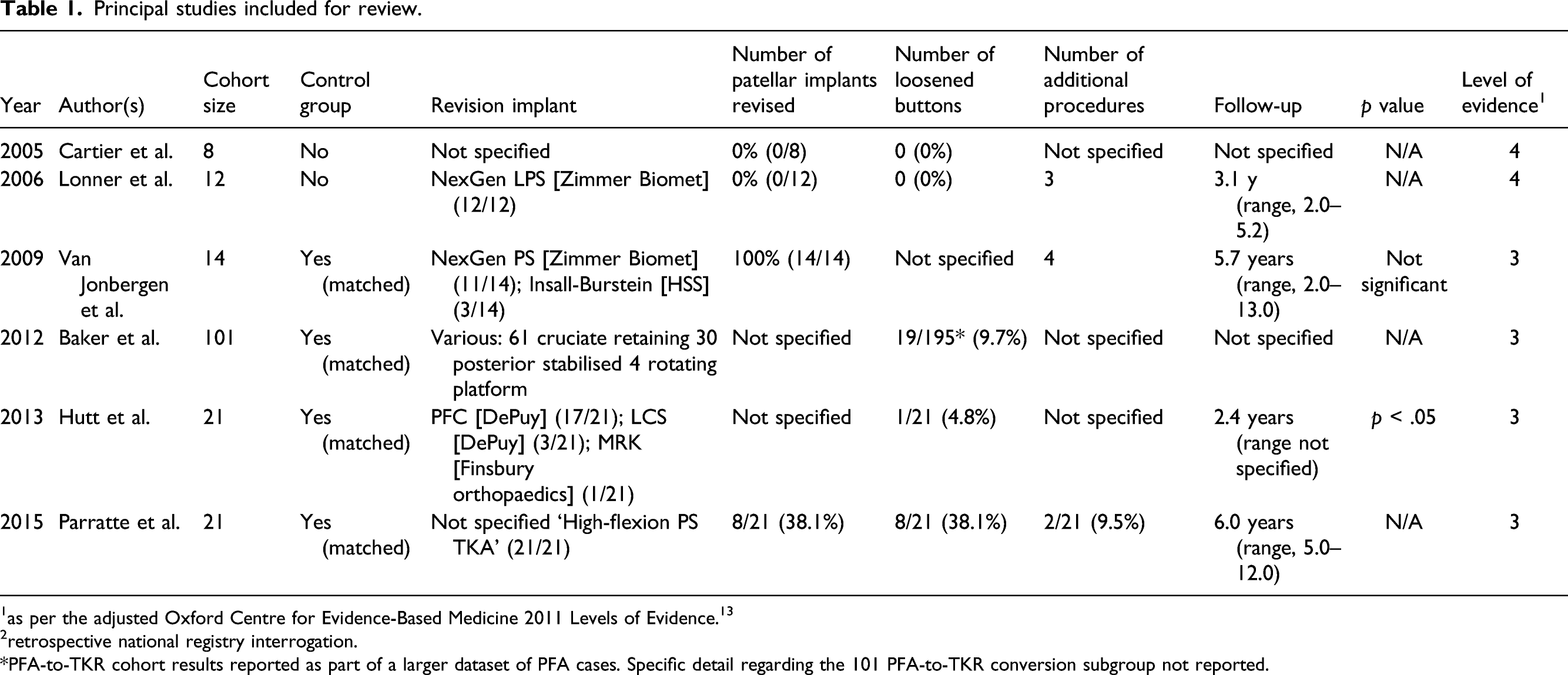
1as per the adjusted Oxford Centre for Evidence-Based Medicine 2011 Levels of Evidence. 13
2retrospective national registry interrogation.
*PFA-to-TKR cohort results reported as part of a larger dataset of PFA cases. Specific detail regarding the 101 PFA-to-TKR conversion subgroup not reported.
A 2006 study by Lonner et al. 7 analysed the revision of 12 failed PFAs to TKAs at a mean of 4 years from primary operation, with 10 initially being for primary patellofemoral arthritis and two for post-traumatic arthritis. At the time of revision, the average age was 50.1 years. The reasons for revision included patellofemoral maltracking or catching (3), progression of tibiofemoral arthritis (6) or a combination of both (3). The original trochlear components included the Lubinus (7), the Autocentric (3), the Avon (1) and the LCS (1), with all being converted to a posterior stabilised NexGen Legacy TKA. The 12 patellar components were an all-polyethylene central dome prosthesis, cemented in situ, and intra-operatively, it was determined that none (0) of the patellar components required revision on account of all being deemed well-positioned without substantial wear, loosening, fragmentation or macroscopic oxidation. They also tracked acceptably with the revised femoral prosthesis. After an average follow-up of 3.1 years, there was no evidence of loosening of implants, and all patellar components remained intact without evidence of excessive tilt, clunking or subluxation, in addition to an improvement in PROMs and function. Although a small study, this work suggests that appropriately scrutinised in situ patellar buttons can be retained with good results in the short- to mid-term.
These results supported the earlier small case series by Cartier et al. (2005) 14 who retrospectively reviewed long-term results of 59 Richards II and III implants over an average of 10 years. Of these, a total of 8 knees (13.6%) required conversion to TKA for progressive tibiofemoral arthritis. They retained the original all-polyethylene patellar button in all cases, including cases with decreased thickness of the implant but without evidence of overt component loosening. The authors deemed the revision surgery to be ‘simple’ with results comparable to those of a primary TKA, although outcomes of this sub-set of results and the period of follow-up post revision surgery were not stated.
A retrospective matched case–control study by van Jonbergen et al. (2009) 8 analysed the conversion of 13 patients (14 knees) with Richards II patellofemoral prostheses to Insall-Burstein TKA (3 knees), and NexGen posterior stabilised TKA (11 knees), at an average of 11 years after the index operation. In all cases, the patellar component was removed and replaced with the ‘standard’ domed patellar button, without encountering any technical problems during conversion. This was performed uniformly due to concern that the Richards II all-polyethylene patellar prosthesis has a long midline central ridge that may predispose to excessive polyethylene wear or maltracking. The authors concluded that PFA did not have a negative effect on the outcome of future TKA, with no statistically significant differences in knee outcome scores compared to primary TKA at a mean of 5.7 years post‐operatively. However, a high number of patients required subsequent manipulations under anaesthesia (MUAs) in the conversion group (23.1%; 3/13), although no patella or extensor mechanism complications were described, per se.
Christ et al. (2017) 15 described an implant retrieval analysis following the conversion of 21 PFAs to posterior stabilised TKAs from 2001 to 2011. Nineteen of these were anterior cut second-generation PFA implants, and the patellar component was revised in nine of these procedures. Two patellar implants had severe wear - both in the same patient who had bilateral valgus deformity with recurrent lateral patellar subluxation - and one had a failed LCS modular patella. They again deemed that conversion was technically straightforward with similar operative times and implants used as in primary TKA. However, post-operatively, the complication rate was noted to be closer to that seen in revision TKA, with a high number of additional procedures performed, including four patients requiring MUA and three prosthetic joint infections. Furthermore, two separate patients with DePuy PFAs who had their patellar component revised ‐ one for patellar clunk and the other for pain - suffered recurrent patellar dislocations and later progressed to patellectomies. Despite the large number of further procedures, range-of-movement and pain scores were reported to be similar to primary TKA cohorts, with 16 of 18 patients (88.9%) having no functional knee limitation at an average of 2.25 years from revision surgery.
The number of patellar component revisions were similar in the study by Paratte et al. (2015) 9 in which 21 PFAs were revised to TKAs, of which eight patellar prostheses were exchanged – all found to be loose, malpositioned, worn or with evidence of maltracking. All patellar buttons removed had a small central peg with minimal bone loss. Paratte and colleagues 9 also found that operative times and clinical outcomes were comparable between revision of PFA to TKA and primary TKA, with the majority of procedures safely performed using standard ‘primary’ implants. A higher complication rate in the revision PFA group compared to the primary TKA group was again noted, with two patients requiring unscheduled returns to theatre for acute open haematoma irrigation and debridement without evidence of infection. Overall, although there was a trend for a higher complication rate for revision PFA in comparison to primary TKA, in each of the studies where the original patellar button was left in situ, no complications related to the extensor mechanism at follow-up after conversion were described.7,9,15
Looking at Australian Orthopaedic Association Joint Replacement Registry (ANJRR) data reviewing the risk of repeat revision when PFA was revised to a TKA over a 17-year period, Lewis et al. (2019) 16 found that the main reasons for revision were progression of OA (56%), component loosening (17%) and refractory pain (12%). Of all PFA revisions, 42% had the index patellar component revised - however, there was no subsequent difference in rates of secondary revision when considering initial retention versus revision. Additionally, there were no secondary revisions in the primary PFA to revision TKA group that were deemed to be specifically patella-related. While a near-complete registry such as the ANJRR permits confident appraisal of ‘goodness’ whereby component revision is the defined endpoint, it – as with many large registries – is a blunt measure and lacks the sensitivity to ascribe implant ‘performance’ or long-term patient satisfaction.
Separate studies have tried to better understand clinical performance and patient-defined satisfaction following PFA-to-TKA conversion, reinforcing a sentiment that while such undertakings are usually technically straightforward, knee outcomes post-operatively are often less satisfactory when compared with primary TKAs when considering function and other PROMs.11,17 Whilst these papers do suggest improvements in objective PROMs from baseline after conversion surgery, they make scant comment on patellar component ‘issues’ at time of revision, provide no data regarding the actual rates of the patellar implant revision or detailed technical factors related to this at the time of surgery, nor report with consistency on radiographic outcomes or important patella-related clinical outcomes such as patellar tracking or anterior knee pain at follow-up.
Finally, in the largest non-registry ‘patellar button-centric’ report to date, Lonner et al. (2003) 18 presented the outcomes of an unrevised all-polyethylene patellar component in a series of 202 revision TKAs (not specifically PFAs). At an average of 7 years post revision, it was found that 10% had anterior knee pain (i.e. 21 patellae). Eleven of these showed evidence of loosening and/or excessive wear, and in all 11 (100%), implant failure occurred in patients in which the index patellar component had been sterilised with gamma irradiation in air. The remaining 10 knees were found to have patellofemoral impingement or other soft-tissue abnormalities, a rate deemed comparable to the reported rate of anterior knee pain found after primary TKA. 19 Despite 68% of the revision tibiofemoral components being from a different manufacturer than the index patellar prosthesis (i.e. mismatched), Lonner and colleagues 18 concluded that retaining an all-polyethylene patellar button can be successful if it is well positioned and fixed with minimal wear and no visually appreciable oxidation - a sentiment which was later supported in multiple other studies.20,21 Additionally, a mismatch between product lines may also be considered acceptable if the patellar component articulates appropriately with the femoral prosthesis, with no statistical association between failure rate and the number or geometry of lugs/pegs securing the prosthesis. Thus, in the absence of mechanical wear or evidence of overt loosening, patellofemoral complications may be minimised with concerted retention in a well-fixed, dome-shaped, all-polyethylene patellar prosthesis – regardless of component manufacturer compatibility. 18
Implant design - trochlear component
There are two basic types of patellofemoral prostheses which are based on the method of trochlear preparation. These include first-generation resurfacing implants utilising an ‘inlay’ technique, and second-generation anterior cut implants using an ‘onlay’ technique. 22
First-generation resurfacing implants replace the trochlear cartilage whilst leaving the subchondral bone intact, with the implant embedded into the bone (‘inlay’ design). 22 Given this, their positioning is dependent on the anatomy of the native trochlea with little technical scope for adjustment. Implants can have either an asymmetric trochlea such as Spherocentric (Aston Medical SAS), LCS (DePuy) and Autocentric (DePuy), or alternatively be symmetric such as the Richards (Smith and Nephew) and Lubinus (Waldemar Link) prostheses.
Second-generation implants utilise anterior femoral cuts as in a TKA, entirely replacing the anterior compartment of the knee (‘onlay’ design). This makes them arguably more versatile given that the positioning of the prosthesis can be made irrespective of the geometry of the native trochlea (including the presence of dysmorphology). Once again, they can be asymmetric such as the Hermes (Ceravor), Vanguard (Biomet), JourneyCompetitor (Smith and Nephew) and Gender Solutions (Zimmer) prostheses. The Avon (Stryker), FPV (Wright Medical Technology) and Natural Knee II (Zimmer) are examples of symmetric implants. Design improvements with second-generation implants have led to reduction in patellar maltracking, and have resulted in improved short- to mid-term outcomes, leaving progression of OA in the tibiofemoral compartments as the chief cause of failure.23,24
Implant design - patellar button
The patellar button itself can be dome-shaped, faceted, and be either asymmetric or symmetric. 22 Metal-backed patellar buttons decrease the available polyethylene thickness and have been shown to be more prone to fatigue failure compared to all-polyethylene implants.25–29 Their use has decreased considerably across the past 10 years. 6 Correctly positioned spherical dome designs allow self-centering on the trochlea, and if revision to TKA is needed, they usually allow congruency matching the trochlear shape of the new tibiofemoral components. This makes the all-polyethylene patellar button the most versatile choice and the most frequently used contemporary option. 25 The majority of PFA implants have a patellar button design such as this that theoretically allows retention when converting to TKA. As a special-circumstance consideration, the LCS PFA (DePuy) prosthesis has a metal-backed, mobile-bearing, patellar component deemed only compatible with the trochlear and femoral component in its same product line. 22 If a different TKA prosthesis is to be used, this patellar component should be revised. It is noted that this implant was discontinued in 2009 given unacceptably high complication rates including significant wear, polyethylene fracture or dislocation, extensive metallosis and arthrofibrosis. 22
Conclusion
Limited data exist when exploring the outcomes of PFA-to-TKA conversion to guide point-of-care decision-making, and even less so on the ultimate outcomes of patellar component retainment versus revision. On the basis of current information, it appears that a well-positioned patellar prosthesis that shows no signs of excessive wear, loosening, delamination or visible oxidation can be retained if it tracks congruently with the new tibiofemoral components at the time of revision surgery. Historical analyses would suggest that satisfactory outcomes can be confidently anticipated with no robust evidence to suggest an increased rate of patellar component failure. It is important that an all-polyethylene, dome-shaped, patellar button compatible with current TKA designs is used when performing primary PFA for ease of later revision to TKA if required. As a separate consideration, it may be worth having a lower threshold for revision of patellar implants that were originally sterilised with gamma irradiation in air, given the demonstration of higher failure rates of these component types. Lastly, although now discontinued, if an LCS (DePuy) metal-backed, mobile bearing PFA patellar component is in situ, it must be remembered that this implant is only mechanically compatible with products from its own line and therefore, should be revised if using a different manufacturer for the conversion to TKA to avoid acknowledged high complication rates.
The small number of patients in each of the studies available for review substantively limits the comparison of outcomes between retention of the patellar button compared to revision. Ideally, further randomised studies analysing the mid- to long-term fate of the unrevised all-polyethylene patellar component in revision PFA to TKA should be conducted, with particular attention paid to clinical performance surrogates such as PROMs at follow-up (including the presence of anterior knee symptoms) or patellar component failure. Given the relative infrequency of these procedures, this may present an opportunity for future initiatives drawing upon larger nationwide and/or industry-supported registry composites.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.