
Abstract
This study presents empirical evidence on self-medication with analgesics among elite German handball players. The aim is to elucidate the intentions behind therapeutic and preventive analgesic use and identify high-risk profiles for this complex health-risk behavior based on psychosocial factors. Data were collected from 459 handball players (233 female, 226 male athletes) across the highest German divisions (1st – 3rd and German Youth Handball Bundesliga) through a quantitative online survey conducted between October 2021 and April 2022. The survey requested demographic information and details on analgesic use patterns, intentions behind analgesic use, and psychosocial variables. The study shows that athletes use self-medication with painkillers as a coping strategy to manage distractions from acute injuries and pain as well as to prevent expected distractions. Engaging in self-medication allows athletes to navigate the pressures of elite sport. Classification tree analysis revealed distinct risk profiles for therapeutic and preventive analgesic use. Key factors of self-medication include age, athletic identity, willingness to compete hurt, and perceived performance state. The high-risk group for therapeutic self-medication with analgesics consists of senior athletes. The high-risk group for using analgesics preventively, in contrast, is composed of athletes over the age of 17 with strong negative affectivity, a heightened willingness to take risks, and good perceived performance. Our findings highlight the necessity for specific interventions to address the multifaceted motivations behind self-medication and promote safer practices in elite sports. Future research should concentrate on longitudinal studies and diverse athlete populations and use qualitative studies to gain a deeper understanding of the determinants of analgesic use and to develop effective intervention strategies.
Elite sport poses physical, emotional, and social challenges for athletes. The intensity of competitions, the pressure to perform, and the high expectations placed on elite athletes often create a highly demanding environment. Together with the precarious nature of contracts and the constant chance of failure, the working environment of athletes is characterized by high degrees of uncertainty (Roderick, 2006b). Athletes are thus challenged to balance their individual desire to play, the social pressure to perform, and their goal of staying “healthy” (or fit to play) (Malcolm and Sheard, 2002). Oftentimes, elite athletes are expected to push their bodies to the limit in training and competition, constantly managing and risking their health in the process (Theberge, 2008). According to Hughes and Coakley (1991), a central shared belief among athletes and coaches characterizing what it means to be an athlete “involves accepting risks and playing through pain” (p. 309). Playing through pain is even recognized as “positive deviance” (Hughes and Coakley, 1991: 307), as it represents over conformity to the norms and values of elite sport shared by various stakeholders within the sports network such as medical specialists, coaches and managers (cf. Nixon, 1992). By engaging in health-related risk behaviors such as performing hurt (i.e. playing despite being injured, ill or in pain), athletes further avoid being “inconvenienced” by the club staff or stigmatized by other players as “poofters” (Roderick et al., 2000). Building on this idea, the use of analgesics has been discussed as a strategy to enable performing hurt and thereby meet sport-specific expectations (Mayer et al., 2018). Throughout their careers, athletes are thus socialized into a veritable “culture of risk” (Nixon, 1992), in which they learn that sacrificing their bodies for the game and taking health risks is necessary for success (Atkinson, 2019).
With its high level of physical contact (Luig et al., 2020) and high incidences of injuries (Engebretsen et al., 2013; Raya-González et al., 2020), handball is considered a particularly tough and risky sport and thus offers an ideal platform for research on health-related risk behaviors such as the use of analgesics1. The prevalence of analgesic use is generally high in elite sports (e.g. Harle et al., 2018; Pedersen et al., 2022; Trinks et al., 2021) and especially high in handball (John et al., 2023; Sari et al., 2021), with many athletes relying on analgesics regularly. In a recent sociological mixed-method study with Danish elite athletes, Overbye (2021) found that analgesic use was widespread and significantly influenced by interactions within the sport network. The identified reasons for taking analgesics were extensive, but primarily aimed at participating in competitions and training without distraction, both with and without injury. These findings echo previous research that distinguished between two common strategies for analgesic use in sports. Firstly, analgesics may be legitimately prescribed by physicians and used under medical supervision to treat a diagnosed medical short- and long-term condition or an acute sport injury (Mottram and Mottram, 2010). Despite the ambivalent role of sport clinicians and physicians which are “sometimes supporting the culture of risk, sometimes contributing to a culture of precaution” (Malcolm, 2006: 377), they are still trained to consider the medical side effects of analgesic use and influence the shared decision-making process with athletes and their coaches on this basis (Hainline et al., 2017a; Shrier, 2015). Safai's (2003) work illustrates that while sports medicine professionals partially treat and advise coaches and athletes on the basis of a culture of risk, “the core process remains centred on the desire to heal” (p. 143).
Secondly, existing studies suggest that athletes commonly engage in self-medication with analgesics either to perform hurt or to prevent declines in performance due to potential pain and related distractions (André et al., 2020; Fernando et al., 2017; Warden, 2009). Whereas the first strategy (i.e. using analgesics to be able to perform hurt) is indicative of therapeutic self-medication, the second strategy (i.e. using analgesics to prevent declines in performance due to potential pain) can 1 be described as preventive self-medication. In this study, we define therapeutic self-medication as the use of analgesics without medical recommendation or guidance in the presence of pain or symptoms of illness (cf. Ruiz, 2010) Therapeutic self-medication carries the potential for misuse when analgesics are used in an inappropriate manner (e.g. higher doses than medically recommended or longer time frames of application than medically recommended; Smith et al., 2013). Conversely, we define preventive self-medication as the proactive use of analgesics prior to practice or a game when no pain is present. Due to the nontherapeutic nature of preventive self-medication, it could even be considered abuse, which is defined as “the intentional, nontherapeutic use of a drug or substance, even once, to obtain a desired psychological or physiological effect” (Smith et al., 2013: 2292).
We thus conceptualize self-medication as a health-risk behavior that is part of the culture of risk enabling athletes to play through pain and injury, thereby managing pressures and fulfilling both individual and social expectations. The unsupervised use of analgesics in the context of sport is associated with several risks. Firstly, analgesic use in sport increases the risk of acute and chronic injuries by numbing relevant pain signals and diminishing their informative value regarding overuse of the athlete's body (Berrsche and Schmitt, 2022; Mayer and Thiel, 2018). Secondly, analgesics have well-known side effects, ranging from gastrointestinal toxicity reported as the most common adverse drug reaction (Rich and Scheiman (2000) to renal, cardiovascular and cerebrovascular side effects (for an overview see: Harirforoosh et al., 2013), aspirin-induced asthma (Jenkins et al., 2004) and neurological side effects (Auriel et al., 2014). Self-medication can further heighten the risk of severe negative side effects through overdosing (amount or time period), drug interactions, or a lack of accompanying medication and precautions (Khan et al., 2018; Pedersen et al., 2022). In addition to the adverse side effects of analgesics, Ziltener et al. (2010) suggest that while analgesics might be helpful for some sport-related issues, their use is not beneficial or even contraindicated for some typical sports injuries (e.g. overuse tendinopathy, acute muscle tears, bone fractures and stress fractures).
Given the high prevalence rates, well-known side effects of analgesics and other potential risks associated with self-medication, this study critically examines self-medication with analgesics in elite handball. This empirical investigation focuses on two central aspects of this practice among elite German handball players: 1) the intentions behind therapeutic and preventive self-medication and 2) risk profiles for therapeutic and preventive self-medication.
Self-medication as a coping strategy
On the one hand, we consider self-medication in elite sport as a form of risk-taking behavior in the culture of risk through which athletes attempt to ensure continued participation in sport despite potential health risks and side effects of misuse (cf. Overbye, 2021). Indeed, previous research in elite sports has shown that the culture of risk significantly influences athletes’ willingness to participate despite pain or injuries by using analgesics (Diehl et al., 2019; Mayer et al., 2018; Overbye, 2021).
On the other hand, in accordance with research on doping in sports (cf. Bette and Schimank, 1995, 2006) and on the use of prohibited and permitted substances in sport (Didymus and Backhouse, 2020), we regard self-medication as an individual coping strategy to deal with the challenges of the elite sport setting. As part of an elite sports career, athletes experience physical impairments (e.g. pain or injuries) that create emotional (Reussner et al., 2023), social, and organizational challenges and distractions (Roderick et al., 2000). The constant pressure to perform even when in pain is accompanied by the athletes’ personal and social expectations (cf. Hammond et al., 2014; Roderick, 2006a). Meeting these expectations (e.g. by performing hurt) allows athletes to avoid conflicts or stigmatization. With their easy applicability and strong causal coupling with freedom from pain, the use of analgesics can constitute a particularly practical strategy for athletes in individually treating pain symptoms in temporal connection to their sport. Thus, self-medication with analgesics could represent a ‘useful’ strategy for coping with the elite sport system from the athletes’ perspective. However, by relying on self-medication to maintain participation and performance, elite athletes jeopardize their health in two ways: directly, by using analgesics without supervision and risking misuse and overdosing, and indirectly, by exposing their (potentially weakened) numbed bodies to physical risks.
Coping with injuries and pain through therapeutic self-medication
Being regularly confronted with high levels of physical stress in elite sport, athletes inherently rely on their athletic performance to increase the chance of a successful career. Thus, injuries not only lead to physical pain but can also represent “a disruptive experience curtailing the mode of athletic expression within a milieu of uncertainty about return to play” (Roy et al., 2015: 1). Consequently, pain and injuries can become critical life events (cf. John et al., 2019; Reussner et al., 2023) with the potential to question the athlete's life trajectory, personal identity, and social functioning. For elite athletes, health events can further trigger biographical risks such as losing their spot on the team and their self-image as athletes (Roderick et al., 2000).
In this context, therapeutic self-medication can serve as a coping strategy. Striving to “make the ‘team sheet’” (Roderick and Schumacker, 2016: 166), athletes often opt to play hurt. In this regard, the use of analgesics could allow athletes to continue participation and maintain focus on performance despite pain and injury. Further, through the use of analgesics, athletes regain a sense of control by alleviating immediate pain and hiding accompanying distractions (Overbye, 2021). Consequently, therapeutic self-medication with analgesics even serves a dual coping purpose. First, it enables the immediate continuation of sports participation, preserving the athlete's short-term engagement (Overbye, 2021). Secondly, athletes maintain their sport-related social functioning within the team (Thiel et al., 2015), discreetly managing health-related issues without any disclosure to their sports network.
Coping with potential pain and related distractions through preventive self-medication
In correspondence with our conceptualization of therapeutic use, we consider preventive self-medication with analgesics to be aimed at coping with potential distractions triggered by anticipated pain or physical contact. With pain, injuries, and physical contact being inherent to handball participation (Giroto et al., 2017; Langevoort et al., 2007), athletes expect their occurrence. By using analgesics before competition or training, athletes increase the likelihood of maintaining participation regardless of external influences (Overbye, 2021) and, as a result, stabilize or potentially enhance their performance (André et al., 2020; Fernando et al., 2017; Warden, 2009). Thereby, similar to doping behavior, preventive self-medication with painkillers can be regarded as a control mechanism in elite sports careers.
However, the attempt to ensure performance through the use of certain substances represents a paradoxical strategy, wherein certain risks are reduced by increasing other risks (cf. Bette and Schimank, 2006). While self-medication with analgesics might manage current biographical risks associated with an athletic career (e.g. getting substituted or experiencing declines in performance), their use generates additional physical risks and postpones biographical risks to the future.
The role of psychosocial factors in therapeutic and preventive self-medication
Based on theoretical considerations regarding health-risk behaviors (e.g. Mayer et al., 2020), we hypothesize that certain combinations of psychosocial factors increase the likelihood of athletes engaging in self-medication. As empirical studies on the psychosocial determinants of self-medication with analgesics in elite sports remain scarce, we also draw on existing scholarship regarding health-related risk-taking more broadly. We assume that self-medication is impacted by similar structural, social, and personal determinants as other health-related risk behaviors. Demographic factors such as age and gender are discussed in the context of risk-taking in sports (Charlesworth and Young, 2006) and analgesics use in elite sports (John et al., 2023). Further, an athlete's performance level has also been linked to playing hurt (Hammond et al., 2014; Mayer and Thiel, 2018) and analgesic use (Leyk et al., 2023). Moreover, we assume that how athletes perceive their own health status may play a relevant role in self-medication as it has been found to influence the general use of analgesics in elite sports (Overbye, 2021). Similarly, risk behaviors could also be linked to the athlete's evaluation of his or her own performance. Since performance is crucial to future team selection, athletes may attempt to compensate for poor performance by taking health risks but may also validate positive performances through risk-taking behavior in order “to maintain membership in the athletic fraternity” (Hughes and Coakley, 1991: 322). Finally, athletic identity and perfectionism have also been shown to contribute to health-related risk behaviors (e.g. Coker-Cranney et al., 2020; Mayer et al., 2018; Schnell et al., 2014).
Purpose of the study
Previous studies have examined the prevalence of therapeutic self-medication among amateur and competitive athletes (e.g. André et al., 2020; Fernando et al., 2017; Locquet et al., 2016), discussed preventive analgesic use in sports from a theoretical perspective (Warden, 2009, 2010) and investigated the potential performance-enhancing effects of analgesics (Holgado et al., 2018; Semark et al., 1999). Whereas most studies have been conducted from a sport medical perspective, a recent study analyzed analgesic use from a sociological perspective investigating the situations and routines in which Danish youth and senior elite athletes use analgesics (Overbye, 2021). However, there is a lack of studies focusing on and empirically investigating therapeutic and preventive self-medication, particularly with regard to exploring psychosocial determinants that characterize risk profiles for therapeutic and preventive self-medication among elite athletes.
In this study, we therefore aimed to answer the following two research questions: 1) Why do elite German handball players engage in therapeutic and preventive self-medication with analgesics? 2) What are the risk profiles for therapeutic and preventive self-medication among elite German handball players?
To answer these questions, we analyzed the intentions behind therapeutic and preventive self-medication with analgesics among German handball players, drawing on Overbye's (2021) research on the reasons for sports-related painkiller use among athletes. Additionally, we used classification tree analysis (CTA), a statistical method based on machine learning, to identify psychosocial risk profiles of handball players who are at high and low risk of engaging in therapeutic and preventive self-medication. Even though this is a quantitative methodological approach, it has the potential to explore the complexity of athletes’ experiences and characteristics to a greater extent. By capturing not only the influence of isolated constructs on a dependent variable (i.e. therapeutic and preventive self-medication), but also examining the interaction of different psychosocial factors on a group level, this method provides further insights into the phenomenon of therapeutic and preventive self-medication from a sociological perspective and can therewith inform interventions and future research.
Methods
Study design and participants
Data for this study was collected through an online survey platform between October 2021 and April 2022. Prior to data collection, ethical approval was obtained from the Faculty of Economic and Social Sciences ethics committee at the University of Tübingen (AZ.: A2.5.4-176_ns). All participants provided their informed consent online before proceeding with the survey. On average, participants spent 30 min completing the survey.
The survey was directly disseminated to athletes and clubs via various channels facilitated by the German Handball Federation using anonymous web links. The final sample consists of 459 handball players (233 female, 226 male athletes) with a mean age of 22.8 years (SD = 4.8 years). A total of 9.6% (n = 44, n female = 32; n male = 12) of the athletes competed in the first division, 6.5% (n = 30, n female = 25; n male = 5) in the second division, 28.5% (n = 131, n female = 86; n male = 45) in the third division, and 55.3% (n = 254, n female = 90; n male = 164) in the German Youth Handball Bundesliga (for more information about the sample, see also: John et al., 2023). Thus, the sample of our study can be considered elite on a national level (cf. Swann et al., 2015). On average, the athletes engaged in physical participation in their sport for 13.51 hours per week (SD = 5.57 h).
Instruments
The online survey comprised several components, including a demographic questionnaire, an extensive questionnaire on analgesic use including therapeutic and preventive self-medication, questions on intentions behind using analgesics in self-medication, and questions exploring the participants’ understanding of pain and injuries. Additionally, we collected data on various psychosocial variables to gain a comprehensive understanding of the factors associated with self-medication in this population.
Dependent variables: Therapeutic and preventive self-medication
First, we inquired whether the participants had used painkillers in connection with handball in the previous season. If this was the case, we asked them about the specific situations of painkiller use. These situations included therapeutic self-medication and preventive self-medication with analgesics before practice and competition. If the participants indicated that they had used painkillers in these sport-related situations, we further asked them about the intentions behind their use.
Questionnaire items regarding the intentions behind self-medication
To identify the intentions behind therapeutic analgesic use, we used a self-designed questionnaire that listed potential intentions and asked participants to indicate how much they agreed with each reason for therapeutic use on a five-point Likert scale. Possible intentions behind therapeutic use were derived from previous research (André et al., 2020; Overbye, 2021) and included items assessing the intentions and health-related issues behind self-medication among athletes such as “I took painkillers last season without a doctor's recommendation due to practice-related pain” (Table 1). Similarly, we recorded the intentions behind preventive self-medication before practice or competition based on quantitative and qualitative studies (Hammond et al., 2014; Mayer et al., 2018; Theberge, 2008) and included items such as “Last season, I took painkillers before a game/practice so that I wouldn’t feel any pain that might occur” (Table 2).
Intentions behind therapeutic self-medication.
Intentions behind preventive self-medication.
Independent variables: Psychosocial factors for classification tree analysis
In order to examine risk profiles for therapeutic and preventive self-medication, we assessed several psychosocial variables that had been shown to be associated with analgesic use and health-related risk-taking (see above). The included demographic factors were age and gender. We assumed that the athlete's age could characterize risk profiles as age impacts the access to pain medication, pressure to perform and experiences with injuries and pain management. Similarly, gender was included as a demographic variable, as gender differences in analgesic use patterns have been described in previous studies (e.g. John et al., 2023; Overbye, 2021). We also collected sport-specific variables such as the role within the team (differentiated between first-team players and rotation players), the amount of time the athletes participated in handball per week, the league in which they competed, and their perceived health status and performance state. Furthermore, we assessed the athletes’ personal characteristics. To capture the athletes’ athletic identity, we utilized the Athletic Identity Measurement Scale (AIMS; Brewer and Cornelius, 2001). This instrument assesses three dimensions of athletic identity, namely social identity, exclusivity, and negative affectivity dimensions. We further assessed the athletes’ willingness to take risks using a scale that was designed to assess the athletes’ risk perception and willingness to accept negative physical or psychosocial consequences of athletic activity (Schnell et al., 2014). Further, the various dimensions of perfectionism (self-oriented, other-oriented, socially prescribed) were assessed using the Multidimensional Perfectionism Scale (Hewitt and Flett, 2004). Lastly, the ‘willingness to compete hurt’ scale was used to assess the athletes’ perception of legitimate reasons for not competing hurt (Mayer et al., 2018). Here, the athletes had to indicate their agreement with statements that were related to refraining from competition for various reasons such as not feeling physically resilient, having a cold with fever, or experiencing joint pain at rest (e.g. “I refrain from competitions if I feel joint pain at rest”). Thus, high scores on this scale indicated a low willingness to compete hurt.
Statistical analyses
We conducted two statistical analyses. First, we descriptively analyzed the intentions of elite handball players for therapeutic and preventive self-medication with analgesics. This descriptive data is presented with the mean and standard deviation for each intention. We also indicate the percentage of athletes who “fully” or “rather” agreed with the listed intentions for therapeutic and preventive use.
Second, we identified risk profiles of athletes with a higher (or lower) likelihood of engaging in preventive and therapeutic self-medication. To achieve this, we employed a CTA (Camp and Slattery, 2002). CTA constitutes an exploratory group-level approach that has been successfully used in previous elite sports research to investigate risk profiles of elite athletes with regard to burnout (Granz et al., 2019), willingness to compete hurt (Mayer et al., 2018) and risk acceptance (Schnell et al., 2014). The exploratory character of CTA makes it particularly useful for examining complex phenomena within large samples since it is a “highly flexible (approach that) does not require the stringent theoretical and distributional assumptions of more traditional methods” (Mayer et al., 2018: 145), thereby allowing to include various variable types (nominal, ordinal, or metric) in the exploratory analysis. The classification tree model was preferred over regression analysis to mitigate the risk of overfitting and produce an informative visual output, in which the high and low risk groups can be easily identified (Andrews et al., 2002).
Using principles of machine learning, we employed CTA to detect sub-groups of handball players that exhibited high (and low) probabilities of engaging in preventive or therapeutic self-medication based on the assessed psychosocial predictor variables. Therewith, CTA allows us to capture the complex interplay between psychosocial variables and self-medication. To achieve this, the exhaustive CHAID algorithm (Chi-squared Automatic Interaction Detector) within IBM SPSS 24 systematically detects relationships between the psychosocial factors (independent variables) and therapeutic or preventive self-medication (dependent variable) based on chi-square tests (Camp and Slattery, 2002). At each step of the analysis, the CHAID algorithm identifies the psychosocial predictor that exerts the most influence on the dependent variable, splitting the sample into various subgroups (i.e. when CTA identifies the athlete's role in the team as the first splitting variable, it means that the athlete's role in the team is the psychosocial predictor that exerted the most influence on self-medication. The same principle applies to all further splitting variables). When no further statistically significant splits can be made based on the available psychosocial predictor variables, CTA reaches its “final node” and thus, the high- or low-risk profile of athletes who are characterized by a specific combination of psychosocial factors.
To ensure the validity and reliability of our analyses, we set certain rule specifications for the calculations in line with previous research aimed at identifying risk profiles (cf. McCarty and Hastak, 2007). The significance level for node division and category merging was set at .05. Adjusted to the sample size in this study, the depth of the tree was set to three, and the minimum number of cases in superior or inferior nodes was established as 40 and 20, respectively.
Results
Intentions behind therapeutic self-medication
We asked the athletes who reported therapeutic self-medication with painkillers in the temporal context of handball participation (n = 240; 52.3%) about their intentions behind this use (Figure 1). The analysis revealed that the items “to treat practice-related pain” with 59.6% (M = 3.3, SD = 1.5) and “to treat competition-related pain” with 59.1% (M = 3.3, SD = 1.5) received the strongest agreement (“rather agree” or “fully agree”) from the handball players. Additionally, 43% of the athletes agreed that they used painkillers to alleviate headaches (M = 2.7, SD = 1.66) and 33.3% to treat menstrual pain (Mfemale = 3.14, SDfemale = 1.66).
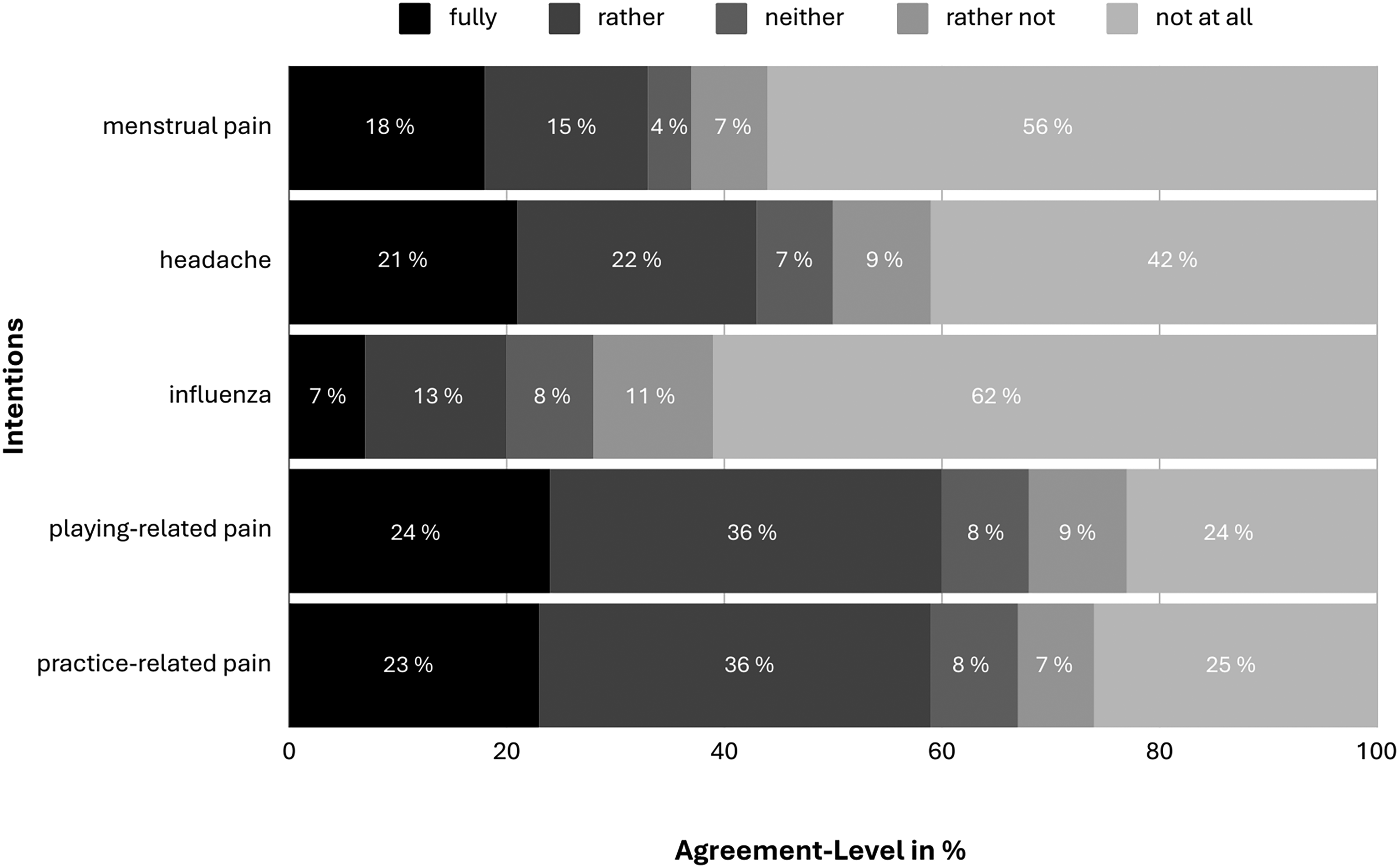
Agreement with intentions behind therapeutic self-medication numbers for menstrual pain is only reported for female athletes (nfemale = 139).
Intentions behind preventive self-medication
Preventive use of analgesics before competition was reported by 84 athletes (18.3%). Among these athletes, we observed strong agreement regarding two specific intentions behind their preventive analgesic use (Figure 2): First, 89.3% of athletes agreed to the intention “in order not to feel any pain that may occur” (M = 4.2, SD = 1.0), and second, 75% agreed to the intention “not to be distracted by any pain that may occur” (M = 3.8, SD = 1.3). The item “to increase performance in competition” (M = 2.36, SD = 1.4) received agreement from 26.2% of the athletes, while only 42% of these 84 athletes stated that they had never taken painkillers preventively with the intention of improving performance in competition. It is further noticeable that preventive self-medication with painkillers was hardly done routinely before competition, with only 2.4% of athletes agreeing to this intention.
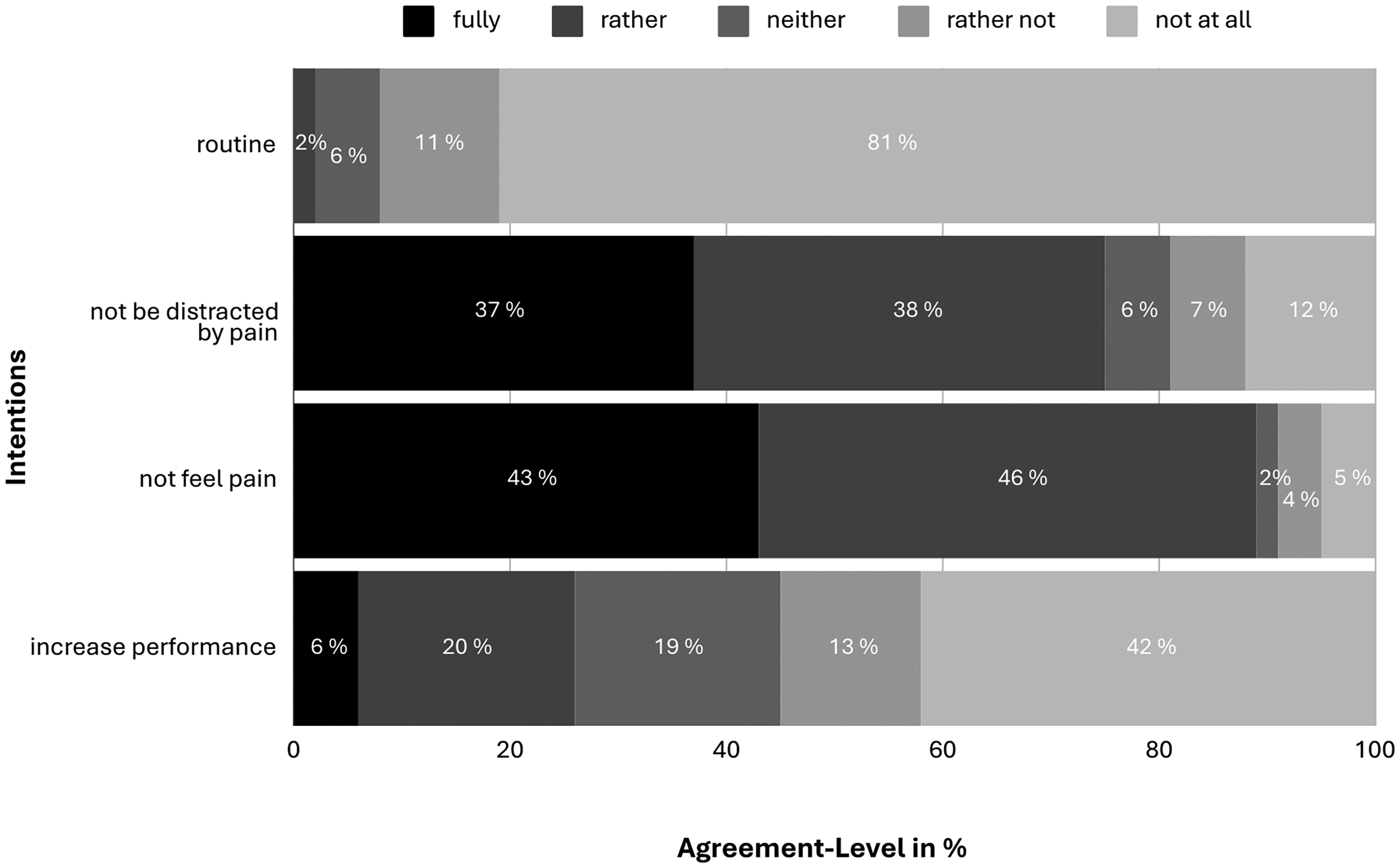
Agreement with intentions behind preventive analgesic use before competition.
Similarly, we examined the group of athletes who reported using analgesics preventively before practice sessions (n = 48, 10.5%). A comparable response structure emerged within this subsample, indicating similar intentions behind preventive analgesic use before practice and competition among the athletes (Figure 3). The two intentions – “in order not to feel any pain that may occur” (M = 4.0, SD = 1.2) and “not to be distracted by any pain that may occur” (M = 3.5, SD = 1.4) – received agreement from 78.7% and 63.9% of athletes respectively. Here, 17.1% of athletes agreed to the item “to increase performance in practice” (M = 2.0, SD = 1.3).
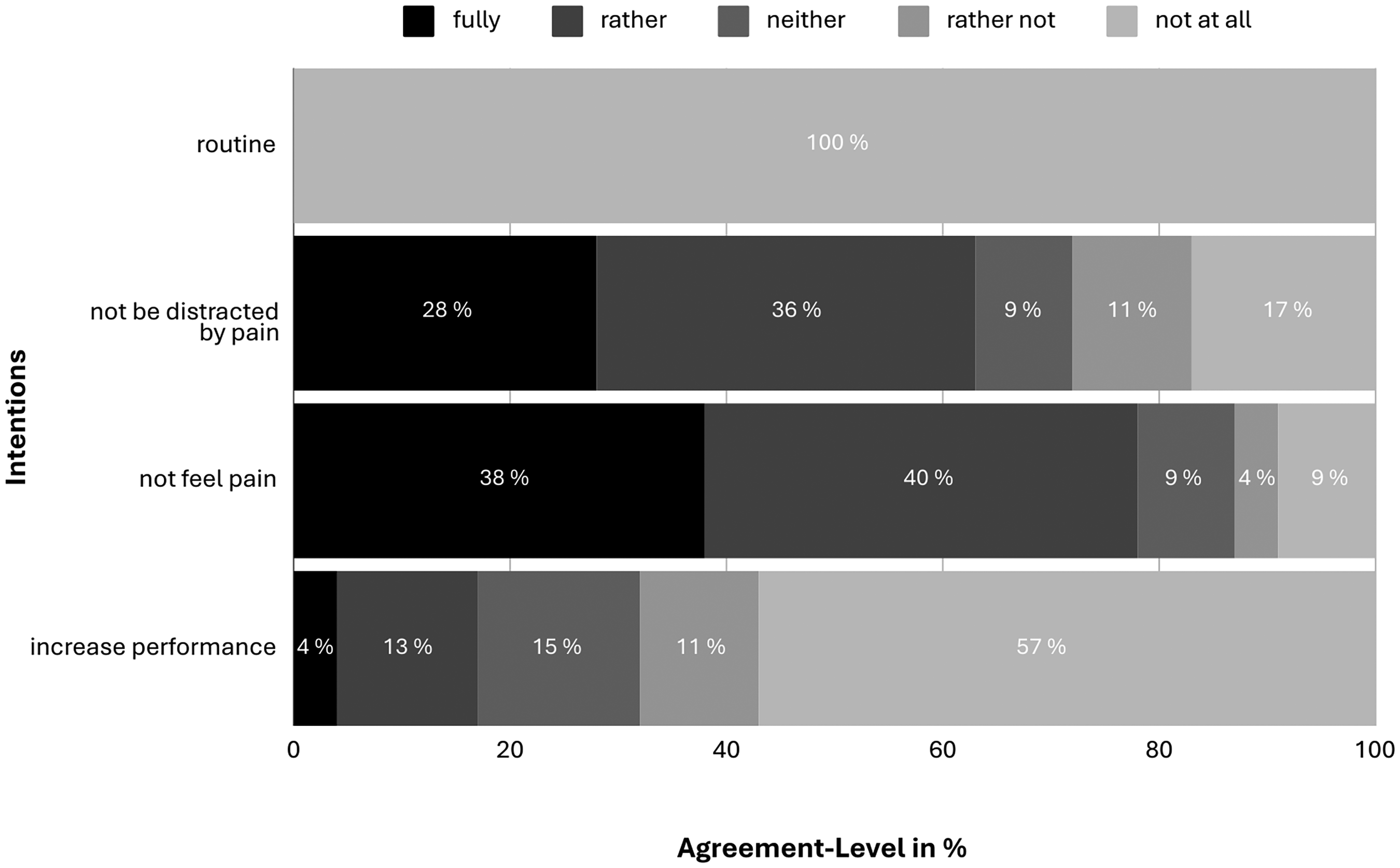
Agreement with intentions behind preventive analgesic use before practice.
Risk profiles for therapeutic self-medication
Among the 231 athletes who practiced therapeutic self-medication (Mage = 19.8, nfemale = 139; n male = 92), the CTA revealed a high-risk profile for therapeutic self-medication consisting of senior handball players (node 1 in Figure 4). The low-risk profile consists of youth handball players who reported a low willingness to compete hurt (node 4 in Figure 4). The athletes’ age level (senior vs. youth) was identified at level 1 and the youth athletes’ willingness to compete hurt was identified at level 2.
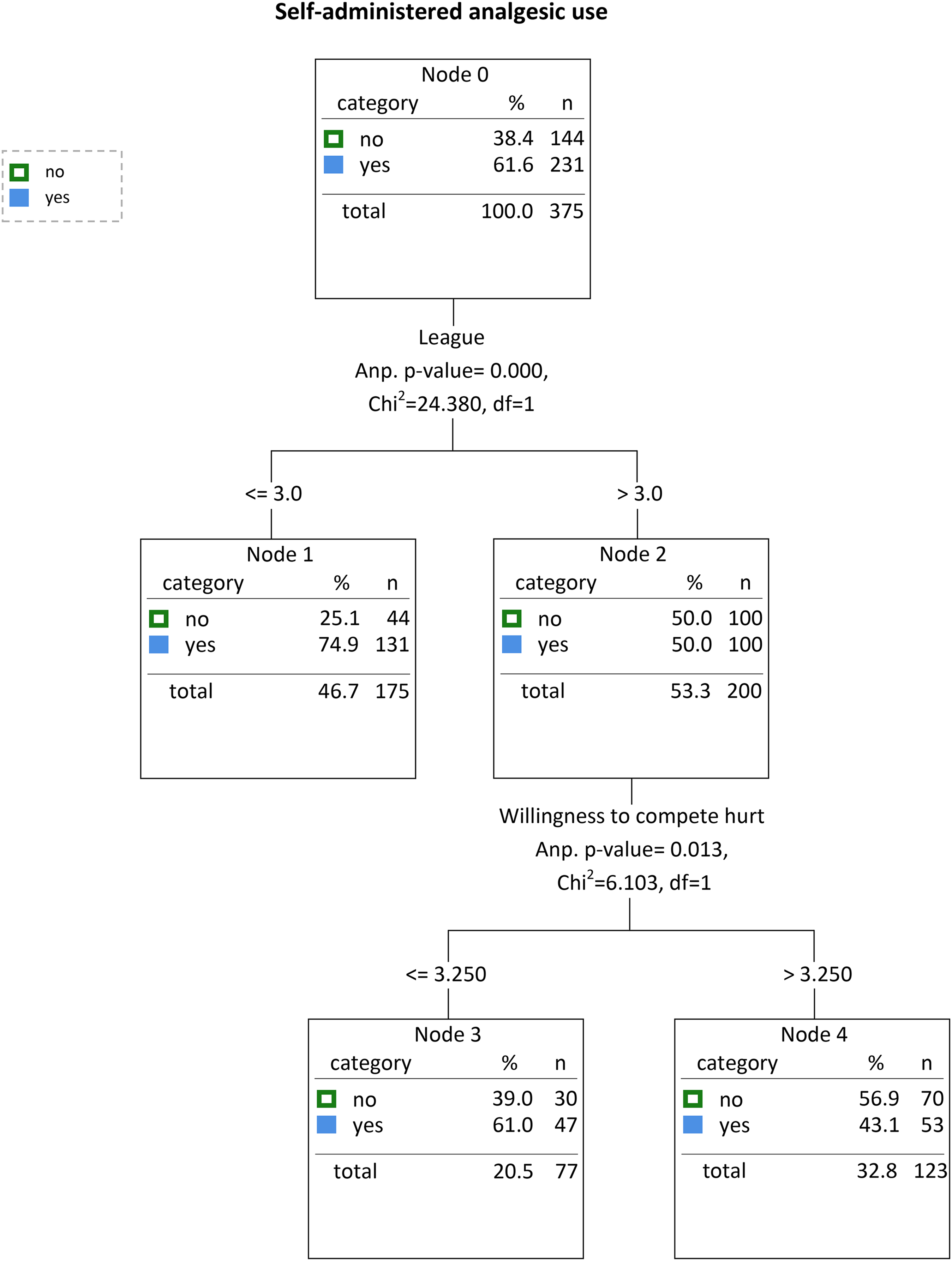
Classification tree analysis of therapeutic self-medication.
Root node – level 1: League
At level 1, the classification tree differentiated between senior and youth leagues. While 74.9% of senior league players engaged in therapeutic self-medication (node 1 in Figure 4), 50.0% of youth athletes reported such practices (node 2 in Figure 4).
Branch beneath node 2: Willingness to compete hurt
Further subdividing the youth players subgroup, the willingness to compete hurt variable was identified on level 2. Youth athletes who were less willing to compete hurt (higher score on the scale) were least likely (43.1%) to therapeutically self-medicate with analgesics (node 4 in Figure 4), while those who were more willing to compete hurt were more likely (61.0%) to self-medicate (node 3 in Figure 4).
Risk profiles for preventive self-medication
Among the 91 athletes who practiced preventive self-medication in practice or competition (Mage = 20.1, nfemale = 42; n male = 49), the CTA revealed a high-risk profile for preventive self-medication consisting of athletes above the age of 17 who scored high on the subfactor negative affect of athletic identity and perceived their performance state in the last season as excellent or good (node 11 in Figure 5). Among this group of players, the prevalence of preventive self-medication was 65.5%. The low-risk profile for preventive analgesic use is characterized by athletes aged 17 or younger who perceived themselves as starters and practiced their sport twelve hours or less per week (node 7 in Figure 5). This profile had a prevalence of 6.6% for preventive self-medication.
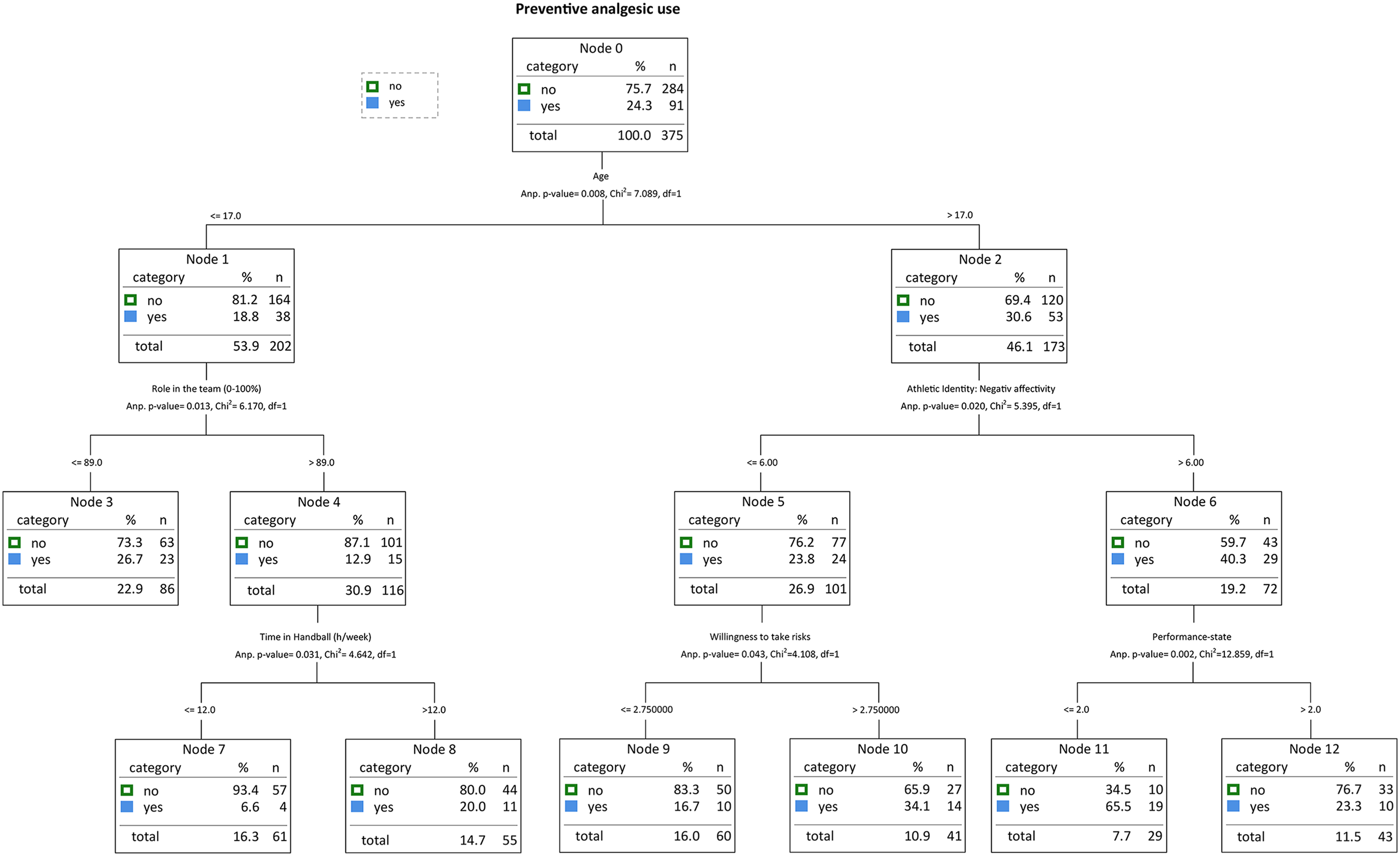
Classification tree analysis of preventive self-medication.
At Level 1, the classification tree differentiated between athletes older than 17 years of age and athletes aged 17 or younger. Role in the team and the subfactor negative affect of athletic identity differentiated groups at Level 2. Willingness to take risks, perceived performance state during the last season, and time practicing handball (h/week) were identified on Level 3.
Root node – level 1: Age
The total sample was partitioned into two subgroups by the predictor age. Athletes above the age of 17 had a significantly higher probability of using analgesics preventively (30.6%; see node 2 in Figure 5) in comparison to athletes aged 17 or younger (18.8%; see node 1 in Figure 5).
Branch beneath node 1: Role in the team and time in handball per week
The subgroup of athletes aged 17 or younger was further statistically divided by the variable of their perceived role in the team. The athletes who perceived themselves less as starters had a higher probability of using analgesics preventively (26.7%; see node 3 in Figure 5) than those who perceived themselves more as starters (12.9%; see node 4 in Figure 5).
Among the athletes 17 and younger who perceived themselves more as starters, the variable of time in handball (h/week) significantly divided the groups. Athletes who spent more than 12 h per week in their sport had a higher probability of using analgesics preventively (20.0%; see node 8 in Figure 5) than those who spent 12 h or less in their sport (6.6%; see node 7 in Figure 5).
Branch beneath node 2: Negative affect, willingness to take risks, and performance state
The athletes older than 17 were further statistically subdivided by the subfactor negative affect of athletic identity. The athletes with a high score on this subfactor had a higher probability of using analgesics preventively (40.3%; see node 6 in Figure 5) than the athletes with a lower score on this subfactor (23.8%; see node 5 in Figure 5).
The willingness to take risks divided the group of athletes with a lower score on the athletic identity subfactor. Those athletes with a higher willingness to take risks showed a higher probability of using analgesics preventively (34.1%; see node 10 in Figure 5) than those with a lower willingness to take risks (16.7%; see node 9 in Figure 5). Lastly, the subgroup of athletes older than 17 with a pronounced negative affectivity of their athletic identity was separated by the variable of their perceived performance state during the last season. Those athletes who judged their performance state as weak were less prone to using analgesics preventively (23.3%; see node 12 in Figure 5) than those who perceived themselves as performing well (65.5%; see node 11 in Figure 5).
Discussion
To our knowledge, our study represents the first study in elite sports investigating risk profiles for therapeutic and preventive self-medication with analgesics among a sample of elite German handball players and their intentions behind these health-related risk behaviours.
Intentions behind therapeutic and preventive self-medication
Therapeutic self-medication with analgesics, which is practiced by every second elite German handball player, can be interpreted as a coping strategy for managing actual physiological symptoms (e.g. pain). However, in line with theoretical assumptions regarding performing hurt (e.g. Mayer and Thiel, 2018; Roderick, 2006a; Roderick et al., 2000), self-medication can also be considered a strategy for coping with psychosocial challenges within an athletic career (e.g. experiencing stigmatization when not performing hurt). In this regard, the athletes in this sample reported treating physical irritations including playing-related or competition-related pain through self-medication (Figure 1). By numbing or suppressing sensations of pain (Warner et al., 2002), players might aim to ensure that they are able to push their physical limits, focus solely on their performance and maintain their athletic identity. Therewith, through using analgesics to manage pain without consulting a doctor, athletes might attempt to navigate personal and social conflicts independently (cf. Theberge, 2008) and consistently achieve freedom from pain during sport participation (Overbye, 2021).
Almost one-fifth of the elite German handball players in this sample also reported self-medicating with analgesics preventively. These players reported using painkillers preventively to engage in handball unfazed by potential pain and, in some cases, to improve their performance (see Figures 2 and 3). Using analgesics preventively prior to practice and competition could be interpreted as an attempt to avoid anticipated challenges. In this regard, by muting potential physiological distractions (such as injury, pain, or expected pain; e.g. Hainline et al., 2017b) with the help of painkillers, elite athletes may also aim to mitigate biographical risks (like substitution or losing their spot on the team; e.g. Hammond et al., 2014). The fact that few athletes also reported using painkillers to enhance performance further generates the idea that analgesics are occasionally used beyond their traditional role (i.e. as painkillers) to cope with performance pressures inherent to elite sports and keep up with teammates and opponents. Similar intentions are also assumed behind the use of performance-enhancing drugs (Pappa and Kennedy, 2013). It should be noted, however, that most athletes did not take analgesics preventively, and of those who did, only some athletes had the specific intention of improving performance.
The presented findings on the intentions behind therapeutic and preventive self-medication suggest that some elite athletes tend to minimize biographical risks by increasing risks in other aspects of life (cf. Bette and Schimank, 1995, 2006). Therewith, self-medication with analgesics represents a paradoxical strategy: to deal with expected distractions due to pain and potential decreases in performance, the athletes in this study took health risks by self-medicating with analgesics for preventive or therapeutic purposes.
Risk profiles for therapeutic and preventive self-medication
The classification tree models identified distinct risk profiles for therapeutic and preventive self-medication characterized through specific sets of psychosocial determinants.
High-risk profile for therapeutic self-medication
Within the CTA for therapeutic self-medication, the athlete's age emerged as a central characteristic for risk profiles, with senior athletes (1st–3rd senior leagues) showing a higher likelihood of therapeutic self-medication with analgesics compared to their counterparts in youth leagues. These findings are consistent with the concept of a risk culture in elite sport. Senior athletes have to cope with even higher pressures to perform (Diehl et al., 2019; Mayer et al., 2018) and expectations to prioritize performance over health (Nixon, 1993; Roderick et al., 2000), which may contribute to a greater tendency to self-medicate with analgesics. In addition to coping with increased performance demands, senior athletes may have accumulated more injuries during their longer careers. As a result, they may have more experience in managing their pain and injuries through the use of analgesics in self-medication, which might be further facilitated by easier access to over-the-counter pain medication.
Low-risk profile for therapeutic self-medication
The low-risk profile for therapeutic self-medication comprised youth players with a lower willingness to compete hurt despite health-related concerns. This finding is consistent with the study of Mayer and Thiel (2018), which identified two clusters among youth elite handball and track and field cohorts, namely “Athletes conditionally willing to rest” and “rest-averse and pain-trivializing athletes”. The latter group would be more likely to use therapeutic self-medication as a coping strategy to maintain their performance while injured or in pain.
High-risk profile for preventive self-medication
The classification tree for preventive self-medication with analgesics (Figure 5) highlights the chronological age as a pivotal factor. Older athletes, particularly those over the age of 17 years, were more likely to use analgesics preventively, suggesting that this risk behavior may be influenced by the transition to a competitive environment. However, the high-risk profile for preventive analgesic use (Figure 4) was further characterized by strong negative affectivity observed in athletes older than 17. Negative affectivity refers to how strongly a person feels negative emotions when experiencing unfavorable results in sports (Brewer and Cornelius, 2001). This finding suggests that athletes who react especially negatively to sporting failure or missing practice and competition may be particularly motivated to self-medicate preventatively to prevent distractions, manage potential discomfort, and maintain their performance. This finding is consistent with the concept of entering an “identity tunnel” (Curry, 1993: 287), which suggests that athletes with a strong athletic identity may actually overconform to the values of the sport because “they see it as confirming or reconfirming their identity as athletes and as members of select sport groups” (Hughes and Coakley, 1991: 311). The identification of the perceived performance state during the last season as the final splitting variable for the high-risk group of preventive analgesic use reinforces the idea of overconforming to the sport ethic through preventive self-medication. According to the assumptions of Coker-Cranney et al. (2020), athletes who “engage in actions aligning with the sport ethic, and receive favorable feedback […] and performance outcomes […] may begin to adopt those methods with increasing frequency” (p. 250). In this regard, the results of the present study suggest that sport performance and success do not necessarily minimize the health-related risk behavior of preventive self-medication. Instead, perceived good performances could also lead to an escalatory dynamic. Athletes may have learned to use analgesics preventively to maintain good performance, achieve success, and thereby also avoid the negative emotional reactions associated with failure or missing out. However, the expected increase in performance and pain resistance through analgesics promises a pseudo-safety, as analgesic use can lead to collateral damage and potential long-term consequences in the form of side effects and acute or chronic injuries (DiFiori et al., 2014; Pedersen et al., 2022).
Low-risk profile for preventive self-medication
The low-risk profile for preventive analgesic use is characterized by age, role in the team, and the time spent playing handball per week. Specifically, young athletes (aged 17 or younger) who perceived themselves as starters and spent less than 12 hours per week playing handball showed the lowest risk of preventive self-medication. This finding suggests that not having to worry about missing out on playing time is a relevant aspect in preventive analgesic use. When athletes perceived themselves as starters who rarely miss a game, they were less likely to use analgesics preventively. This finding corresponds with research suggesting that the pressure to compete for a spot on the team and perceived uncertainty about playing time increase performing hurt behavior (Berg et al., 2014; Roderick, 2006a). In turn, as the athletes perceive their career continuity as secured and the biographical risk associated with missing playing time as low, they appear to reduce potential health risks. Finally, the amount of time spent playing handball each week also constituted a relevant aspect in reducing the risk of preventive self-medication with analgesics. Manageable practice and competition schedules with adequate time between practices and competitions may provide athletes with a “‘window of opportunity’ to recover” (Hammond et al., 2014: 173), which may reduce the perceived need for preventive analgesic use.
Implications for interventions and athletes’ well-being
Addressing self-medication with analgesics is a significant challenge due to its complex and multifaceted nature. The results of our study emphasize that self-medication is not driven by a single factor or motivation; rather, athletes who self-medicated agreed with multiple intentions behind their use of analgesics. Combined with the results of the high- and low-risk profiles, our findings call for a comprehensive, multifaceted, and target-group-specific approach to prevent, control, or combat self-medication with analgesics in elite sports.
First, athletes transitioning to senior levels should be specifically targeted and provided with information on alternative strategies for coping with the increased personal (e.g. pressure to perform) and physical challenges (e.g. pain due to increased intensity) often associated with high-performance sport. Further, athletes who exhibit high levels of negative affects, such as strong negative emotions when experiencing unfavorable results in sports, and who are going through a period of poor performance should be given special attention, as they may be at particular risk of self-medicating with analgesics preventively to regain their athletic role. Since the coaching staff (e.g. coach and athletic trainer) usually has the most contact with the athletes in handball, it stands to reason that they could, if adequately trained, serve as a conduit of knowledge about pain medication or refer athletes to relevant persons. However, research indicates that the coaching staff often perpetuates norms and values related to the culture of risk, such as performing hurt (e.g. Nixon, 1992). Therefore, we suggest that athletes should rather consult trained medical specialists (e.g. general practitioners) from outside of the athletic context (Hughes and Coakley, 1991).
In addition, given the frequent unsupervised use of analgesics, trained practitioners independent of the association and club (such as physicians or sport psychologists) should initiate informed discussions with elite athletes about health as a preventive measure. These discussions could center around the question of how to balance short-term team and individual performance with long-term athlete health and team success in a competitive environment (John et al., 2023; Schubring and Thiel, 2014).
Finally, health-related risk behaviours, such as self-medication with analgesics, should be addressed organizationally in terms of their negative impact on long-term individual and team performance. Accordingly, heightened willingness to take risks and to perform hurt should not be heroicized by the team culture and the coaching staff but should be addressed critically.
Limitations and future directions
While the study's results provide valuable insights, it is essential to acknowledge its limitations. The data collected through self-report questionnaires might be subject to biases (e.g. social desirability, recall bias), and the cross-sectional design prevents causal conclusions. Furthermore, the quantitative approach with predefined intentions behind therapeutic and preventive self-medication constrains the scope for the perceptions and attitudes of the athletes themselves, confining them to the options provided in the questionnaire. As the study focuses solely on German handball players, its generalizability to other sports and populations is limited. However, it characterizes the risk profiles of preventive and therapeutic analgesics use among elite handball players and provides valuable insights into the interplay of psychosocial factors. Future research could include longitudinal mixed-method studies to track and qualitatively assess self-medication over time and explore the effectiveness of interventions aimed at altering the culture of risk-taking and painkiller use in elite sports. Qualitative studies could also provide a very useful approach to identifying the underlying assumptions and perceptions that are particularly conducive to preventive self-medication.
Conclusion
The study provides empirical evidence that deepens the understanding of analgesic use in elite sport by providing valuable insights into two critical aspects of self-medication: first, the intentions behind therapeutic and preventive self-medication with analgesics among elite German handball players and, second, the risk profiles associated with the therapeutic and preventive use of analgesics. The results show that athletes use analgesics in self-medication – sometimes beyond their traditional role as painkillers – to manage anticipated pain and enhance performance. While therapeutic use appears to be aimed at coping with physiological challenges, preventive use is aimed at reducing anticipated distractions (such as pain), maintaining performance, and thereby conforming to the athletic role.
The high-risk profile for therapeutic self-medication with analgesics, with a prevalence of 64.9%, was observed in senior athletes, potentially due to increased performance pressures and accumulated injuries. With regard to preventive analgesic use, the high-risk group with a prevalence of 65.5% comprised athletes aged above 17 years who exhibited strong negative affectivity and had achieved good performances in the last season. Overall, these findings contribute to a better understanding of the complex intentions behind and risk factors associated with self-medication among elite handball players. The knowledge gained from this study can inform targeted interventions aimed at promoting the health and well-being of athletes.
Footnotes
Acknowledgments
We express our gratitude to all the participants for taking the time to complete the survey. We also extend our thanks to the gatekeepers who assisted in distributing the survey to the athletes. A special note of appreciation also goes to Patrick Luig, Dirk Büsch, and Axel Kromer, for their ongoing support throughout the survey preparation and data collection process.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the German Institute of Sport Science under Grant number 070301/21-24.