
Abstract
Athletes who aim to qualify for the Olympic Games need to stay healthy. Research demonstrates, however, that many elite athletes take health risks to achieve sporting success. Drawing on social ecological thinking, the purpose of this study is to understand change in athlete health behaviour during the Olympic Games qualification phase. We draw on data from a six-month-long case study on four athletes who aimed to qualify for the 2016 Olympic Games in Rio. We used semi-structured interviews and weekly-online surveys to collect data. Olympic hopefuls engaged in both risky health behaviour, such as ‘competing while injured’, and in self-caring health behaviour, such as ‘balanced dietary management’. Risk-taking was encouraged by a habit of taking pain medication, insufficient medical support, and time pressure to qualify. Awareness for self-care, a trusting coach-athlete relationship, and a well-rounded athlete support programme were factors that promoted self-care. Conceptually, we found that athlete health behaviour is dynamic and ecological, that is, it is relational to personal, contextual, and temporal factors. Based on the findings, we advise Olympic hopefuls to surround themselves with people who support caring health behaviour, and that sport organisations and stakeholders adopt long-term planning and implement policies of care.
Keywords
Athletes who aim to qualify for the Olympic Games (OG) need to stay healthy. Research has demonstrated, however, that many elite athletes have a narrow, functional understanding of health and that they are ready to take various health risks to reach sporting success. Taking painkillers, competing with pain and injuries, excessive weight loss, doping and reducing recovery have been found common practices (e.g. Berg et al., 2014; Joy et al., 2016; Lentillon-Kaestner et al., 2012; Overbye, 2020). During the qualification phase for the OG, staying healthy is additionally complicated. Athletes are under pressure to achieve both international and national qualification standards, knowing that seats for their country's travelling teams are restricted and that the games only take place every fourth year (Gould and Maynard, 2009; Hanton et al., 2005; Schubring et al., 2019a). Further, participating in the OGs constitutes for many athletes a long-term dream and the pinnacle of a possible athletic career (Barker-Ruchti et al., 2019; Jensen et al., 2014).
Sociologists describe a range of causes for athletes’ readiness to take health risks. These include socialization into elite sport culture (Nixon, 1992; Schubring and Thiel, 2014; Theberge, 2008), performance-focused support systems (Howe, 2001; Malcolm and Safai, 2012), career transitions (Barker-Ruchti and Schubring, 2015), selection criteria for teams, training centres, and competitions (Cavallerio et al., 2016; Lentillon-Kaestner et al., 2012), precarious work-conditions and structural dependencies (Mayer and Thiel, 2016; Roderick, 2006). While research on elite sport risk behaviour 1 and its sociocultural underpinnings is substantial, little attention has been given to caring health behaviour 2 in athletes and the reasons why athletes may decide against taking health risks (for exceptions see Barker-Ruchti et al., 2017; Safai, 2003; Schubring and Thiel, 2016). Consequently, there is limited knowledge on how athletes navigate between risk-taking and self-care. Further, scholars have rarely considered change in athlete health behaviour in the OG qualification phase. In this study, we address this gap in knowledge with the purpose of understanding change in athlete health behaviour during the OG qualification phase. Our specific aims are to identify ecological factors, which include both individual and contextual aspects, that influence athlete health behaviour, and to conceptualise the ecology 3 of athlete health behaviour during the OG qualification phase.
To achieve these aims, we first establish McLeroy et al.'s (1988) ecological theory of health behaviour as the analytical framework for the study. Next, we describe our methodology and present four storied cases on Olympic hopefuls’ risky and caring health behaviour. We close the article with an empirically grounded conception of the ecology of athlete health behaviour before discussing implications for research and practice.
Ecological theory and athlete health behaviour
Ecological theories are increasingly used to study health behaviour and to identify barriers and facilitators of positive health 4 outcomes in different groups and contexts (Golden and Earp, 2012; Sallis and Owen, 2015). Health behaviour is herein understood as lifestyle choices and practices, which impact on individuals’ bodily, social, and/or mental health (Antonovsky, 1996; McLeroy et al., 1988). Following the ecological turn, scholars in the social sciences of sport have also drawn on ecological thinking to understand athlete health and wellbeing. However, most of the existing empirical studies focus on problematic behaviour, such as alcohol and drug consumption (Fetherman and Bachman, 2016; Smith et al., 2010; Williams et al., 2006), as well as the causes of negative health outcomes in athletes, such as injury, emotional abuse, and mental ill-health (Jacobs et al., 2017; Kuettel and Larsen, 2020; Stirling and Kerr, 2014).
From an ecological systems theory point of view, health behaviour is understood as ecological in nature, which means ‘a joint function of person and environment’ (Bronfenbrenner, 1989: 25). Change or stability in health behaviour is theorised as the result of ongoing interaction between a person's individual characteristics and the social and physical environments in which one lives. Drawing on Bronfenbrenner's work (1979), McLeroy and colleagues (1988) argue that health behaviour is multifaceted and influenced by barriers and facilitators operating and intersecting between individual and environment. To systematise influences on individual health behaviour, the authors suggest grouping influences on five hierarchically ordered levels (see Figure 1). 5 The first, intrapersonal level, includes an individual's knowledge, attitudes, behaviour, self-concept, and skills, but also ‘the developmental history of a person’ (McLeroy et al., 1988: 355). In the context of elite sport, for instance, a strong athletic identity has been found to increase athletes’ readiness to take health risks (Mayer and Thiel, 2016; Roderick, 2006), while career longevity can support self-care in athletes (Barker-Ruchti et al., 2017). The second, less proximal interpersonal level, encompasses other significant relationships, such as with family members, friends, work colleagues, and social networks. Coaches, teammates, or medical support staff have been found to both positively and negatively influence athlete health behaviour (Madrigal et al., 2015; Malcolm, 2020; Safai, 2003; Schubring and Thiel, 2016). The third, organisational level, encompasses formal and informal rules, organisational culture, economic and social resources, but also work hazards that ‘can have substantial influence on the health and health related behaviour of individuals’ (McLeroy et al., 1988: 359). In elite sport, the culture in a training group can lead athletes to normalise pain and injuries or to refrain from using drugs (Cavallerio et al., 2016; Lentillon-Kaestner et al., 2012; Overbye, 2020). The next distal, fourth level, termed community level, comprises the interrelations between different groups to which an individual belongs, including personal friendship networks, as well as the ‘relationship among organizations’ and the ‘power structures’ within a political or geographic area (McLeroy et al., 1988: 365–366). If, for example, coaches’ employment conditions depend on athletes’ performance and the number of elite athletes they train, or if coordination between local and national governing bodies of sport is weak, these relationships and power structures can influence athlete health behaviour (Dohlsten et al., 2021; Jacobsson et al., 2018). The fifth, most distal level, constitutes the public policy level, which refers to local, regional, and national policies and laws. Supporting factors for athlete health on this level can be the development of regulatory mechanisms to reduce hazards such as concussion or abuse or policies to encourage dual career development (European Commission, 2012; Lang, 2020).
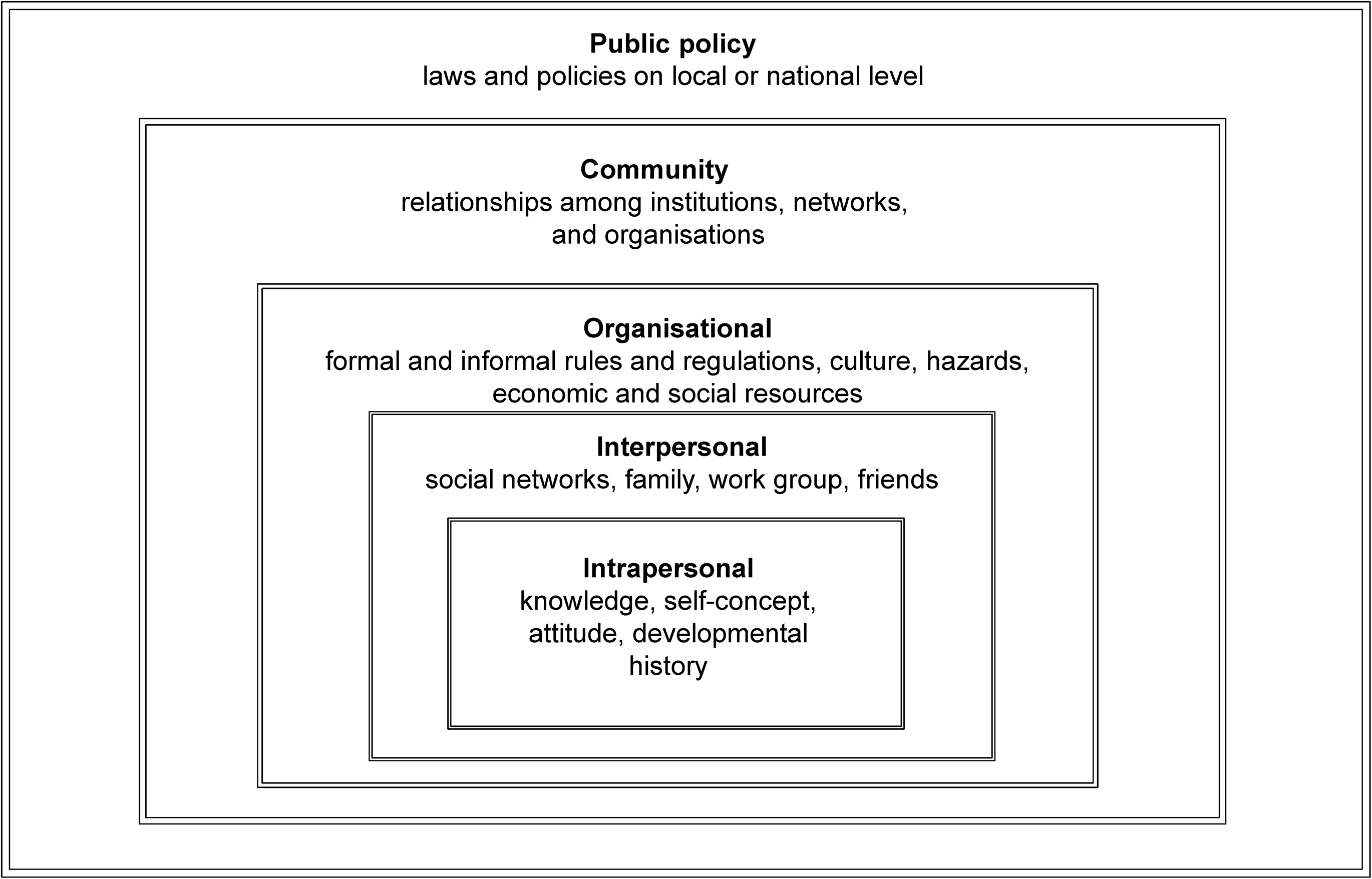
Ecology of factors that influence health behaviour.
In the following, we use the ecological framework presented in Figure 1 to study Olympic hopefuls’ health behaviour during the qualification phase. In so doing, we advance the application of the general health ecology framework to the context of elite sport in three ways: First, the multilevel factors of influence, such as family or culture, are general. Information on their quality and presence/absence is needed to understand whether they promote, maintain, or discourage health-risky or caring behaviour in athletes. Second, depending on the elite sport context, factors of influence need further specification and additional factors may be identified. Finally, given that individuals are nested within a dynamic and complex system of relationships (Bronfenbrenner, 1989: 25), influencing factors do not operate on their own but interact and cut across different layers of the environment. Thus, identification of context-specific factors of influence needs to be coupled with a deeper understanding of the rhizomatic ways they co-exist and interact to influence athlete health behaviour. To address these shortcomings and develop an empirically grounded conception of the ecology of athlete health behaviour, we discuss the general health ecology framework in dialogue with Olympic hopefuls’ lived health behaviour. First, however, we outline the methodology that allowed us to generate the article's data.
Methodology
To examine athlete health behaviour during qualification for the OG, we adopted a longitudinal, qualitative case study design that allowed us to collect in-depth context-specific data and to capture change over time (Neale, 2020; Yin, 2014). The data included in this research constitutes a sub-study of the Paths-to-Rio project through which we accompanied ten athletes from fall 2015 to fall 2016 who aimed to qualify for the 2016 OG (see Schubring et al., 2019a: for study description). The project has obtained clearance from the Regional Ethical Vetting in Gothenburg (Dnr. 954–13).
Sampling of participants
For this article, we used ‘maximum variation (heterogeneity) sampling’ (Patton, 2015: 283) to purposefully select four information-rich cases from the data collected for the Paths-to-Rio project. Purposefully selecting ‘a small sample of great diversity’ has two strengths: it yields ‘high-quality, detailed descriptions of each case, which are useful for documenting uniqueness and diversity’, and allows identifying ‘important shared patterns that cut across cases and derive their significance from having emerged out of heterogeneity’ (Patton, 2015: 283). Drawing on these principles, we assured variation regarding: (a) type of sport, and (b) OG qualification. The sampling resulted in the inclusion of athletes from two individual and two team sports, two of whom qualified for the OG (see Table 1). 6 The four athletes were all aged in their twenties and attempted to qualify for the OG for the first time. The exclusiveness of the sample does not allow us to identify the athletes’ sport, exact age, and the country where they live and compete.
Description of participating athletes (using pseudonyms).

Data collection
Upon recruitment and information on ethical safeguarding, the four participants first answered a background questionnaire on their sporting career and health situation (see Schubring et al., 2019b). Second, we used a weekly web survey that included 12 closed questions on athletes’ health and training state, as well as risky and caring health behaviour (see Schubring et al., 2019a). During the qualification phase, on average, the four athletes completed 21 of the 26 weekly surveys (min. 18; max. 26) sent to them. Third, each athlete participated in two semi-structured interviews, one in fall 2015 and the second in spring 2016. The first interview served to explore athletes’ sporting backgrounds, their health experiences and preparation for the OG. To support interviewees to express their own attitudes and experiences, we used short stories (vignettes) depicting three different examples of athlete health behaviour (see Schubring et al., 2019c). Interviewees were invited to reflect and comment on each vignette in relation to their own sport and behaviour. In the second interview, we asked participants to share their qualification phase experiences and expectations about qualifying for and participating in the OG. To explore athletes’ negotiation of risky/caring health behaviour, we created line charts based on athletes’ weekly survey responses and brought a printout to interview 2. These line charts visualised changes athletes had reported regarding their performance, physical health and well-being between interviews 1 and 2, and facilitated reflection and probing on factors contributing to the changes (see Schubring et al., 2019c). All interviews were recorded and transcribed verbatim.
Data analysis
Procedures to analyse longitudinal qualitative research data are limited and seldom directly applicable to other studies (Thomson and McLeod, 2015). Against this background, our analytical procedure is the result of a methodological journey directed by the aim to understand change in athlete health behaviour during a qualification phase. Two main analytical steps can in hindsight be distinguished:
Case-wise chronological analysis to identify critical situations
In this step, the first and second authors created chronological portfolios for each athlete to integrate their survey responses and interview data, and to contextualise and temporalize athletes’ health behaviour. In a first section, we summarized information from interview 1 and the background questionnaire along four themes: athletic background, previous health problems, expectations for the upcoming qualifying phase, and support situation. The second section contained a chronological report on the qualification phase. We used months as headings under which we summarized the athletes’ weekly survey responses, alongside eventual competition participation, and interview quotes describing athletes’ experiences of critical situations. This analytical step resulted in data consisting of 15–21 A4-pages per athlete and a total of 72 A4-pages for the four athletes. The portfolios enabled us to identify situations in which athletes needed to navigate between risky and caring health behaviour and to select one particularly critical and data-rich situation per athlete for deeper analysis. These situations included suffering an injury close to a qualification event (Nick); intense training leading to pain (Debbie); lack of adequate medical support at a training camp (Bianca), and necessity to meet weight requirements (Cara).
In-depth analysis of critical situations for ecological influences
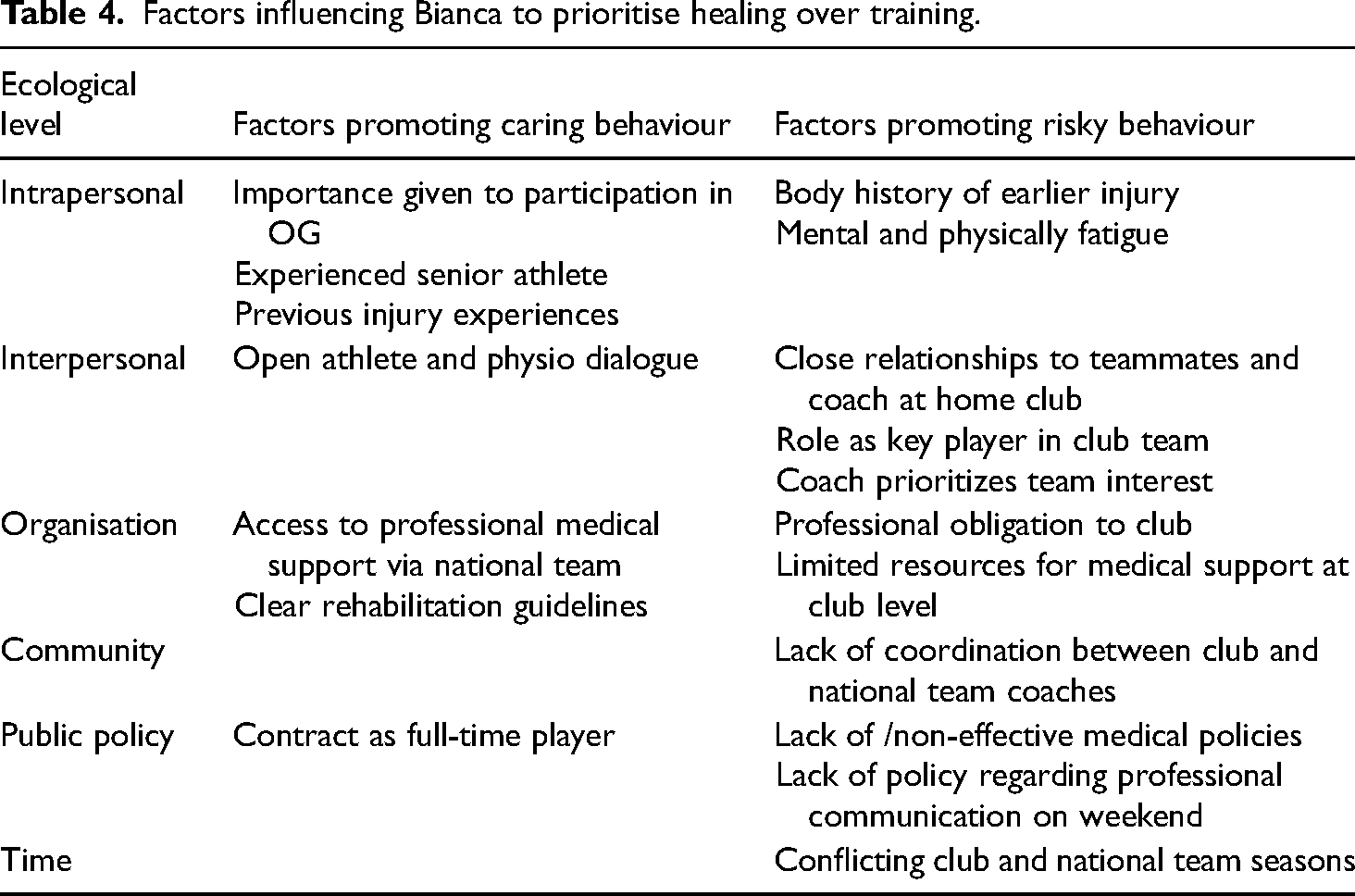
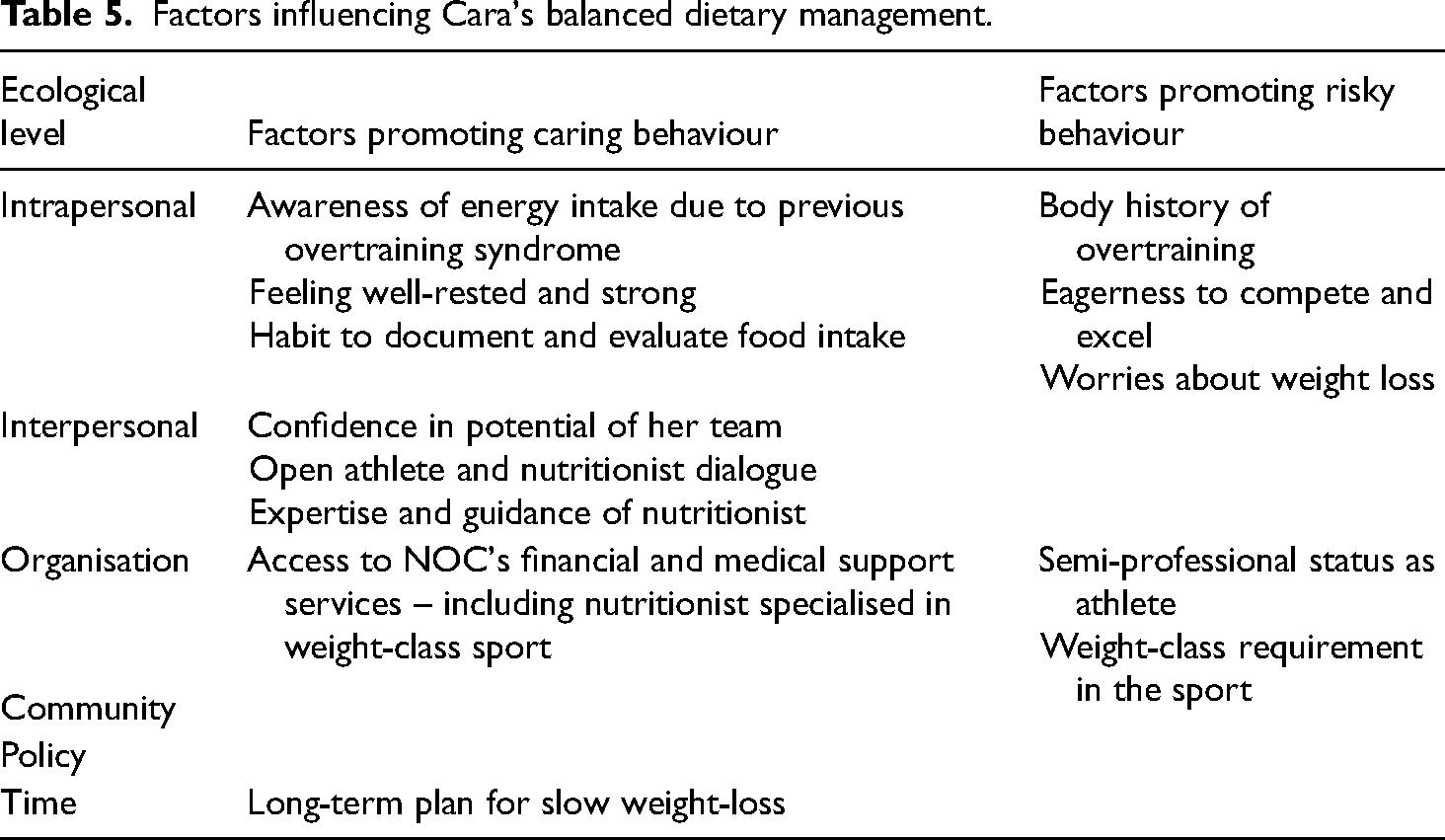
The second step involved an in-depth analysis of the identified critical situations. Using ecological theory, we analysed the interplay of factors that influenced athletes’ health behaviour and then used the ecological levels to group them thematically (see Tables 2–5). During the analysis, two adaptions were necessary. First, we distinguished factors promoting risky or caring behaviour. Second, we found the timing of events important in influencing athlete health behaviour and therefore included time as an additional layer. Finally, we went over the case-specific factors of influence on each level to reduce unnecessary duplicates and formulate overarching labels where needed. This analytic step resulted in the creation of a revised, ecological model of athlete health behaviour, which served to situate the empirically identified influences (see Figure 2).
While conducting the analysis, the first and second author discussed and audited interpretations in the author group. The co-authors, who hold expertise in pedagogy, nutrition, and sustainability studies, acted as ‘critical friends’ (Smith and McGannon, 2018) and their reflections, as well as exploration of alternative interpretations, allowed the refinement of the findings (Cornish et al., 2013).
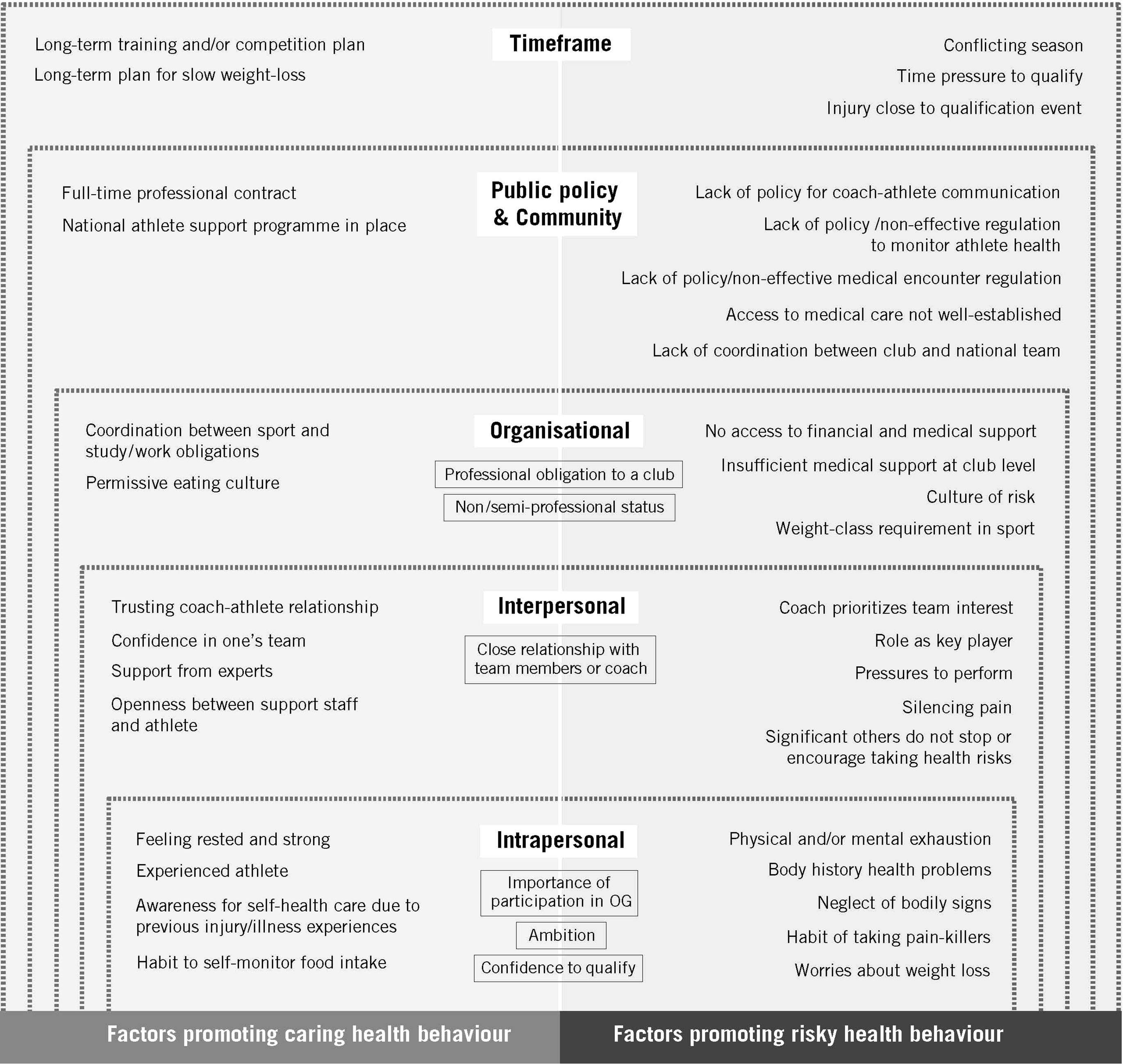
Model of the ecology of athlete health behaviour in the OG qualification phase.
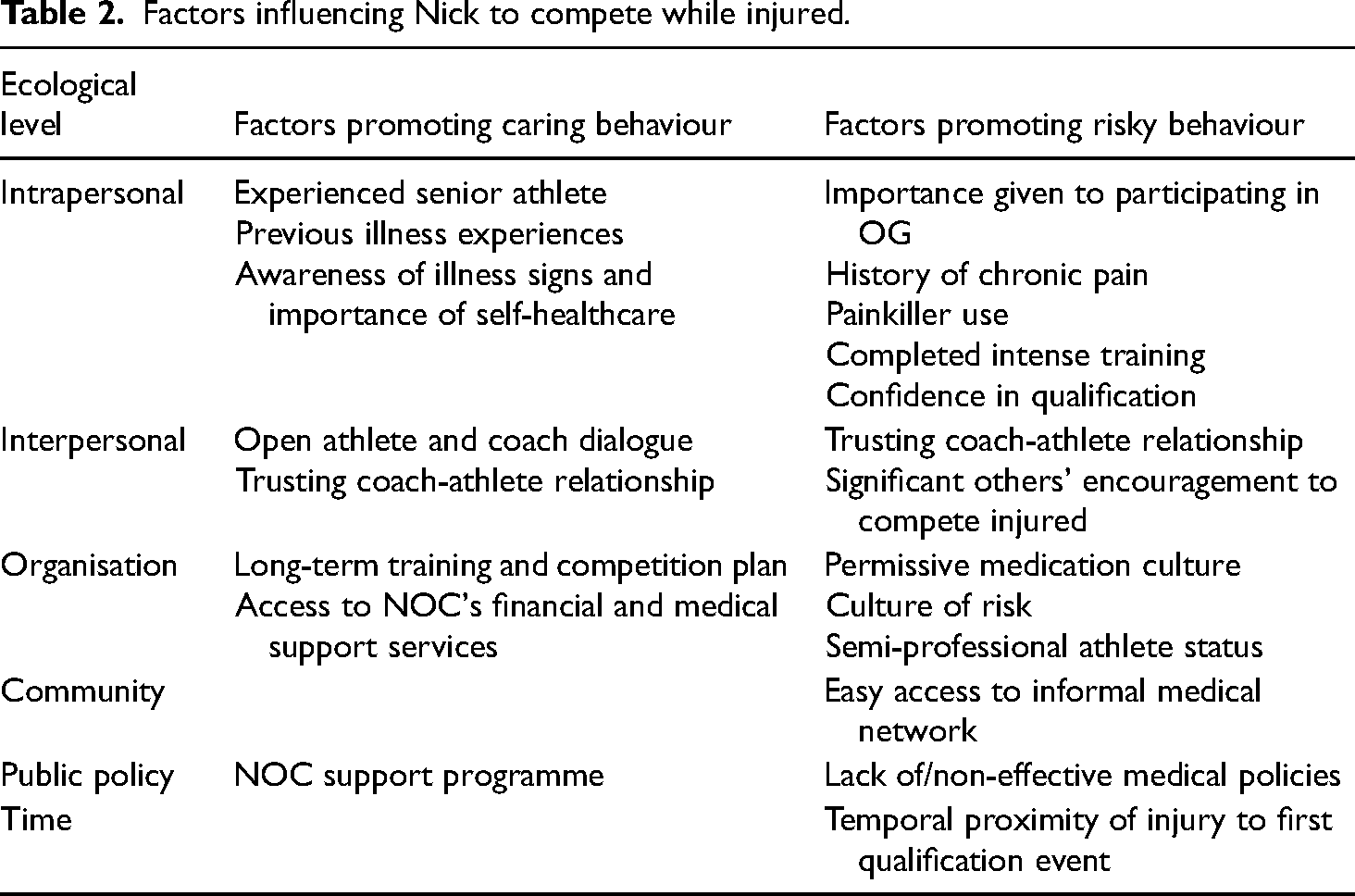
Factors influencing Nick to compete while injured.
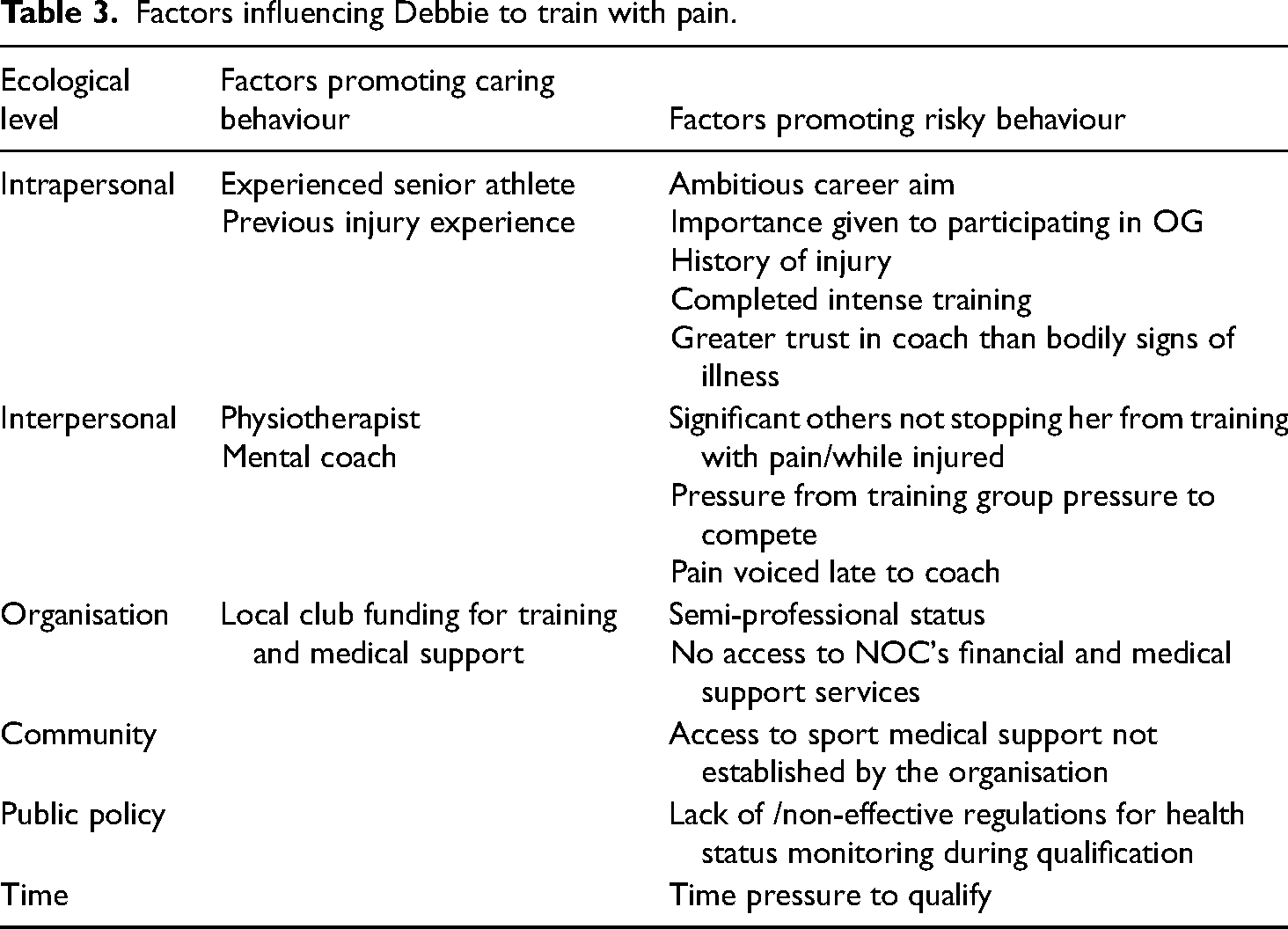
Factors influencing Debbie to train with pain.
Factors influencing Bianca to prioritise healing over training.
Factors influencing Cara's balanced dietary management.
Representation of data
To capture the interplay between Olympic hopefuls’ health behaviour, and the ecological influences, we chose to represent our findings through non-fictional short stories followed by analytical comments. From a methodological perspective, storying constitutes a powerful way to share and make sense of human experience (Smith and Sparkes, 2009). Storied representations further facilitate accessibility of findings (Cavallerio et al., 2016) and have the potential to act upon readers by teaching them what to pay attention to or by calling forth reflection (Polkinghorne, 1988). In our case, the storying of findings allowed the chronological ordering of events and the integration of the different types of data. In this way, the importance of past, present, and future time for athlete health behaviour could be acknowledged.
To create the short stories, we chose one situation from each athletes’ portfolio data, which captured the navigation between risky and caring health behaviour particularly well. When storying, we paid specific attention to the contextualisation in athletes’ past backgrounds, careers, and health situations; the temporalization by including details on time and change, and the ecology, by including information on factors of influence for athletes’ health behaviour. To preserve confidentiality, we use pseudonyms for persons and places, and disguised or withheld some details (e.g. sport, injury location, or historical time) that would make the cases easily identifiable to insiders (see Schubring et al., 2019a). We entitled the created short stories a) competing while injured, b) training with pain, c) prioritising healing, and d) balanced dietary management. Below, we give some contextual information and then present the four short stories, each followed by an analytical section that identifies and discusses ecological influence.
Findings
About a year before the games, the four Olympic hopefuls were generally critical towards taking health risks, but also described that finding the ‘right balance’ between ‘pushing the limits’ and caring for bodily needs was difficult. During the six-month long qualification phase, maintaining the advocated balanced health regime was repeatedly challenged. The short stories give insight into this process and the ecological factors influencing Nick, Debbie, Bianca, and Cara's health behaviour.
Competing while injured – Nick
Nick competes in an individual high intensity sport and has been part of the national team for several years. He is also a member of his country's National Olympic Committee (NOC)'s athlete support programme, which gives him access to support services (e.g. nutritionists, medical staff) and a stipend, but he also works part time to make a living. A few years ago, Nick had his sporting break-through and since then, participation in the OG has become highly important: ‘My dream goal is to be in the Olympics’. Earlier in his career, Nick suffered from overtraining and believes staying healthy and not getting injured during the qualification phase to be crucial. At our first meeting in autumn 2015, he explains: ‘My philosophy is if you are in pain, it is not going to get better if you train hard, and it's better to rest one or two days than be away for maybe a couple of months’. At that time, he also hoped that the chronic pain he felt during the previous season would subside. Nick had been taking painkillers to keep training and competing, which people in his training environment had assured him was no danger.
Nick trained intensely from autumn 2015 to January 2016. When entering the competition season in early spring 2016, he therefore felt strong and confident to be able to meet the qualification requirements set by his NOC. Nick's goal was to qualify early to have as much time as possible to prepare for the OG in August the same year. To reach this goal, Nick's coach Tom planned for Nick to start the season with smaller events to build up Nick's confidence. In a training session, a few days prior to what was planned to be Nick's first competition for the season, Nick had an accident that resulted in a bone fracture in his upper body. Worried about his participation in the competition, Tom and Nick decided to consult Jim, a physiotherapist they knew well and whom they trusted, because ‘he had been a martial arts athlete so he knew a lot about this type of fractures’. Jim examined Nick saying that ‘nothing is broken, it's no danger, it's just the pain’. Nick felt relieved thinking: ‘When someone tells me that there is no danger, and you cannot get more injured or anything, then I can handle it. Then I can handle the pain’. Based on Jim's conclusion, Nick and Tom decided Nick would continue to compete, however, in another event to reduce the impact and pain. Despite the injury, Nick delivered a top-performance, but felt not satisfied. Over the following weeks, Nick took painkillers to avoid reducing his training to heal the injured bone. After all, he thought, ‘my injury is sort of a good pain because I know it's not dangerous. I can train with it’.
Analytical summary
The account demonstrates how various ecological factors influenced Nick to compete while injured instead of resting to heal his fractured bone (see Table 2). The table evidences that Nick both disposed of experiential knowledge and was situated in an environment that could promote health-caring behaviour, such as a trusting relationship with his coach and the financial and medical support he received via his NOC. However, these factors were outweighed by other factors such as the importance Nick attached to participation in the OG, the subtle ‘culture of risk’ (Nixon, 1992) in which health consequences of competing injured/taking pain killers were silenced, as well as the organisational lack of policies in case of medical encounter. An important aspect in Nick's ecological situatedness constitutes the timing of the injury, which created time pressure and possibly also led Tom and Nick to consult Jim instead of trying to get an appointment for a full medical assessment.
Training with pain – Debbie
Debbie is a semi-professional athlete who has been competing at the senior level in an individual technical sport for several years. Her greatest success besides her national medals was her participation in a world championship. Since then, she has worked on developing her performance, but also suffered a major leg injury, which threatened to end her career. Debbie could recover and has returned to elite level training in her club. While her ‘goals for Rio are very high’, her greatest dream is ‘going for world record’. Besides her sporting career, Debbie works nearly full-time. She is a member of a sport-specific team of elite athletes supported by a local elite club but is not a member of a national support programme.
In autumn 2015, Debbie followed an intense training regime to prepare for the qualifiers in spring 2016. Jessi, her coach, has planned for Debbie to skip the indoor season to increase the volume and intensity of her training. Debbie trusts her coach and his expertise. A few months into the intensive preparation training, Debbie realised: ‘I have pushed my body a lot and need to give myself a rest to avoid injury’. While the pain in her leg stirred up worrying memories of her previous injury, Debbie struggled to tell her coach, ‘because, it feels hard to not be able … he made me a program and then I have to say, no, I can’t do it because my body feels a bit tired’. Several weeks pass, where Debbie first tried training with pain and taking some painkillers before getting help from a physiotherapist and a mental coach. When finally speaking with Jessi, he told her: ‘maybe you have to accept that you will feel like this, but you also have to learn what pain is okay, and what pain is not okay. While Debbie felt relieved that ‘my coach can tell me that’, she concluded that ‘if I want to be a good athlete, I have to push myself.’ In February 2016, her pain was not better but worse, but Debbie still thought ‘at the moment, it is possible (and necessary) for me to train with some pain’. To keep the volume of 16–23 hours per week, Debbie and Jessie adjusted her training. Debbie also thought of the upcoming training camp abroad. It felt important to participate, especially in the competitions that can serve as qualifiers – if she could just reach the required norm. While Debbi worried about her pain and the limited medical support abroad, she decided to travel with her team. At the camp, several weeks passed before she was able to compete. Seeing her teammates compete for qualification stressed Debbie. While still in pain, she competed every weekend trying hard to perform well, however, without reaching the required qualification norm. Upon return from the camp, Debbi is required to rest to recover. In May, Debbie returned to training, but suffered yet another muscle injury in the leg in which she had experienced pain since the end of 2015. She finally had a medical check, and the diagnosis was devastating. Debbi must stop training to heal the injury and it becomes impossible to qualify in time for the Olympics.
Analytical summary
Debbie's story of months-long training with pain gives insight into the procedural nature of athlete risk behaviour and ecological factors that can impede proper medical diagnosis and recovery during an OG qualification phase (see Table 3). While Debbie, like Nick, has experiences and resources (e.g. physiotherapist, local support programme) that could promote caring behaviour, her situation appears more precarious from the outset (e.g. obligation to work, lack of support, prior injury). Factors that add to this precarity are partly intrapersonal, as well as interpersonal and organisational. For example, organisational practices, policies, and structures appear absent or insufficient to provide Debbie with medical care early and to follow-up on her health status. Further, the cultural belief that pain is part of being an athlete (Overbye, 2020; Theberge, 2008) and the growing time pressure to qualify created a dynamic in favour of risk-taking that Debbie did not defy on her own.
Prioritising healing – Bianca
Bianca is a team sport athlete. She enjoys the everyday contact with her teammates and full-time employment by her club as a player makes her feel confident and secure. For a few years, Bianca has also been a member of the national team and had just recently played the World Championships (WC), which was a dream come true. Bianca experienced several injuries earlier in her career.
At the end of 2015, Bianca looked forward to her club entering the off-season. She felt worn out ‘both mentally and physically, because you are active the whole year round’. Although knowing she should prepare for the highly intense national team camp scheduled at the beginning of 2016, she decided to take a break, reasoning that ‘you have to consider what [is] best for you’.
A few days into the national team camp, Bianca suffered a muscle rupture. The national team's medical staff were certain that the injury requires rest and rehabilitation. They requested a physiotherapist to overlook Bianca's rehabilitation at home. The hope was for the injury to heal before the upcoming qualification game for the OG. During the prescribed rehabilitation, Bianca's home club had to prepare for the season with a training camp abroad. Because of her key role in the team, her club tried to convince Bianca to join the camp but informed her that they could not afford to bring along a physiotherapist. Bianca explained to her club coach that she wanted to join the camp, but also wanted to continue her rehabilitation. She felt torn between her club and the national team. The repeated requests stressed Bianca, especially when her club coach called ‘during the weekend wondering: “well, don’t you want to come?”’ Bianca felt that her coach ‘puts the whole pressure on me’. Unsure about what decision to take, she talked to her physiotherapist, who advised her to stay at home. Bianca followed this advice. She reasoned that ‘it is stupid to travel that far and not bring a physio if something happens’. Bianca felt relieved once the decision was made. Now she could focus on recovering from the injury.
Analytical summary
Bianca's story, similar to Debbie's, demonstrates how athlete health behaviour is a ‘joint function of person and environment’ (Bronfenbrenner, 1989: 25), where factors promoting caring and factors promoting risk-taking interact (see Table 4). Bianca's mental and physical tiredness at the end of the season can be included with the factors that promote risk-taking. Further, interpersonal and organisational aspects together with the conflict between club season and national team OG qualification timeline complicated prioritising her health. Factors that enabled self-care in Bianca were her wish to participate in the OG but also that she, in contrast to Debbie, expected her club to have a ‘duty of care’ – a reasoning that may be grounded in her professional work relationship with the club. Interpersonally and organisationally, her physiotherapist and the clear guidelines from the national team doctors provided crucial support for Bianca to prioritise healing over training while injured.
Balanced dietary management – Cara
Cara is a team sport athlete who combines elite sport with part-time studies. Like Nick, she is part of her country's NOC's athlete support programme, which gives her access to support services (e.g. nutritionists, medical staff) and a stipend. Cara had her international breakthrough a few years prior to the OG, when her team qualified for the final at the U23 WC. In Cara's sport, weight plays an important role, which demands her to carefully manage her food intake. She had previously worked with a nutritionist, but the recommended diet left Cara feeling deprived of energy and struggling to perform. Having developed an overtraining syndrome that required bed rest to recover, Cara left the nutritionist concluding that s/he had little insight into the specific demands of her sport. After becoming a member of the NOC support programme, she started to work with Melanie, a nutritionist specialised in weight class sports.
Entering the qualification phase in autumn 2015, Cara felt strong and confident about her team: ‘we know that we have the ability to become the best in the world’. Having had time to recover from an intensive competition season, she felt well rested and eager to train and compete again. During the first weeks, Cara struggled to match her food intake with the amount of energy she burned in training. Several times, she felt she was eating enough but the food record she kept revealed that she ate too little. Knowing from experience that ‘nine times out of ten you eat too little’, Cara developed a habit of documenting her food intake, especially when increasing her training volume. Cara found this method as helpful.
Two months before the qualifying event, Cara began deliberate weight loss to weigh into the right weight class. Melanie, her nutritionist, set up a plan to help her lose weight slowly and in stages. In the beginning, as Cara explained, the diet involved ‘no great changes really, but you have to pay more attention to what you eat, it's as simple as that’. While she felt that Melanie's instruction about what to eat were easy to follow, it bothered her that she now must weigh everything she ate. There were moments when Cara wished to compete without the weight requirement, but she knew that ‘it's just part of the sport’ and ‘everyone that I compete against has to do it’. Even though Cara made weight several times and managed to reach the required weight, she felt anxious and worried about the diet and whether it would work. As the weeks passed and she gradually lost weight and got in shape, positive feelings took over. Cara was glad she could talk to Melanie about her concerns during this time: ‘I really trust her, because I know that she is an expert in her line of work’.
Analytical summary
The storied account of Cara's dietary management, in contrast to the previous three, focused on another dimension of athlete health behaviour. Similarly, multilevel factors interact but the athlete's overall situation appears more secure from the outset. While there are intrapersonal aspects and organisational conditions that could promote ‘elite sport risk behaviour’ (Schubring et al., 2019a), they are outweighed by factors that support a balanced approach (see Table 5). Key aspects are the intrapersonal resources Cara developed following her overtraining experience and that she entered the qualification phase well-rested. On the interpersonal and organisational levels, Cara received professional, financial, and emotional support. A central figure is the specialist nutritionist who guided her through the emotionally demanding weight loss period. The long-term planning that Cara and her nutritionist did also had a health protective function.
Conceptualizing the ecology of athlete health behaviour
The combined use of non-fictional short stories to temporalize the four athletes’ health behaviour together with social ecological theory (Bronfenbrenner, 1979; McLeroy et al., 1988) as an analytical lens allowed us to identify both the multilevel factors that influenced athlete health behaviour in the OG qualification phase and to gain a deeper understanding of their interaction. Based on the findings, we came to understand athlete health behaviour as a dynamic process during which athletes navigate between risk-taking and self-caring. We further conceptualise athlete health behaviour as the result of a complex interplay between athletes and their multilevel contexts. In this ecology, we consider athletes as both agents grounded in the individual capitals they bring into play, and subject to micro- and macro-level influences which they need to navigate. To provide an empirically grounded conceptualisation of the ecology of athlete health behaviour in the OG qualification phase, we have – based on the case-based analysis of factors of influence (Tables 2–5) – developed an ecological model (Figure 2) that distinguishes between barriers (right half side) and support factors (left half side). Factors that we found can promote either caring or risky behaviour – depending on context and timepoint – are placed centrally. Further, we present the identified community and public policy factors on a joint public policy & community level for easier representation (see discussion further below), and we have added the distal level, timeframe, given its identified importance.
Discussion
The purpose of this study was to understand change in athlete health behaviour during the OG qualification phase. We found that the OG qualification period is an extremely demanding career phase, which can jeopardize athlete health and wellbeing. Besides intense training, competition schedules, and time pressure to qualify, the athletes in our study faced unpredictable events and set-backs, such as injuries or missed qualifications, while several also completed studies or a part-time job to secure a living. The multiple demands, coupled with the insecurity of qualifying, complicated the athletes’ initial wish to care for their health. As in Nick's and Cara's cases, competing injured and training hurt was adopted notably when feeling under time pressure to qualify while also being entangled in relationships, communities and structures that created expectations for athletes to take health risks. In the absence of integrated health management approaches and policies in favour of athlete health and well-being, athletes are left on their own in a precarious situation (Dijkstra et al., 2014; Lang, 2020; Roderick, 2006). However, we also found that athletes have agency to resist taking health risks, especially with adequate interpersonal and organisational support and policies of care (see also Schubring and Thiel, 2016; Barker-Ruchti et al., 2017; Dohlsten et al., 2021). Bianca's and Cara's cases exemplify how athletes prioritized to heal an injury and used a balanced dietary management to deal with weight-class requirements in their sport. These examples are educational for research and practice, as they demonstrate how social conditions can facilitate self-care in athletes despite a highly demanding career situation. As sociological research has often focused on problems related to athlete health and well-being (e.g. Cavallerio et al., 2016; Jacobs et al., 2017; Malcolm, 2020; Young, 2004), we call for more studies on self-care and positive health outcomes in athletes, including how athletes navigate between health-risky and caring behaviour. Embracing these dimensions will generate new research questions and understanding the social conditions of self-care in athletes can give direction to sport organisations and practitioners.
To identify ecological factors that influence athlete health behaviour, we drew on McLeroy and colleagues’ (1988) system of five levels of influence (intraindividual, interindividual, organisational, community and policy). This systematization facilitated classifying findings from each of the cases (see Table 2–5) and aggregating them across cases in a comprehensive overview of factors that promoted caring and/or risky health behaviour in athletes. The empirically grounded conceptualisation of the ecology of athlete health behaviour in the OG qualification phase (Figure 2) yields important insights:
First, it clarifies that athletes are situated in and part of a multilayered, interrelated ecology (for similar argument, e.g. Henriksen, 2010; Jacobsson et al., 2018) and as such are and should not be made solely responsible for their health behaviour as individualistic health discourses suggest (for similar arguments Golden and Earp, 2012; Malcolm, 2020; Quennerstedt, 2019). Instead, several levels of influence, such as organisational, policy and time-related aspects, as well as the relationship between them, need to be factored into the equation. While the athletes’ career goals, experiences, habits, body histories, or state of exhaustion clearly matter, influences situated more distally to the athletes, such as athlete support programs, financial security or lacking medical policies, can outbalance or even overrule athletes’ interpersonal dispositions and perceived possibilities to act (for similar findings see Dohlsten et al., 2021; Fetherman and Bachman, 2016; Jacobsson et al., 2018).
Second, the empirically grounded model (Figure 2) suggests that ecological factors are neither general nor relationships between them universal, but that they change meaning and importance depending on the sport-specific, historical, and individual context. For example, we found that significant relationships, a professional contract, and the subjective importance of the OG can, depending on the situation, motivate risky or caring health behaviour, which is why we placed them in the centre of the model (see Figure 2). While this contingency reflects the complexity of athlete ecology (Jacobsson et al., 2018; Roderick, 2006), it complicates formulating clear-cut guidelines for practice. To address this challenge, we see a need for more longitudinal case studies on athlete health behaviour in different career phases and sports. Further, we propose that it is key to reflect with athletes, coaches and their managers on the observed dynamics.
Third, the model facilitates the systematization of the factors that supported caring or risky health behaviour in athletes into different levels and domains. This systematisation allows the distribution of factors to be evaluated, demonstrating that a greater number of factors for health-risking were identified in the studied cases than for caring behaviour, notably on the policy and community levels. Further, we found more influencing factors on the proximal levels than on the distal levels. The differences in distribution may reflect that athletes and not elite sport organisations with their communities and policies were the prime subject of our research. However, the distribution can still direct researchers to gaps in current knowledge (see also Golden and Earp, 2012; LaVoi and Dutove, 2012) and serve sport organisations and stakeholders in their efforts to evaluate their practices and structures to identify needs for action.
Despite the outlined benefits, we experienced challenges in the application of McLeroy and colleagues’ (1988) socio-ecological conception. Notably, the distinction between the organisational, policy, and community levels seemed more fine-grained than the distinction between intrapersonal, interpersonal, and organizational levels. Consequently, the distinction between the distal levels was delicate to make when working with the empirical material and some of the identified factors appeared on several of these three levels. To address this challenge and to avoid duplications, we have merged the policy and community levels (see Figure 2). Further, we identified that time-dimensions play an important role for athlete health behaviour – as others have highlighted before us (Barker-Ruchti et al., 2019; Collinson, 2003; Hanton et al., 2005). We have therefore, similar to Bronfenbrenner (1979), added an extra time level and argue for timeframes to be taken into account more systematically when researching the ecology of health behaviour in and outside of sport. While these changes allowed us to refine and empirically ground the conceptualisation of the ecology of athlete health behaviour in the OG qualification phase, it does not aspire to be all encompassing or closed to further development. For example, interpersonal relationships outside of sport can play an important role in athlete health behaviour (Schubring and Thiel, 2016; Madrigal et al., 2015), even if they did not appear decisive in the critical incidences we analysed herein. The model (Figure 2) thus constitutes a heuristic for and not a picture of the ecology of athlete health behaviour.
Methodologically, the qualitative longitudinal design proved to be beneficial. It allowed us to see how athletes navigate between risky and caring health behaviour depending on the individual, interpersonal, organisational and time dimensions they experienced. Based on these insights, we argue that health behaviour needs to be conceptualized as a process and not a one-time-event – a shift of paradigm echoing theorizations of health as a dynamic practice, and not a state (Antonovsky, 1996; Quennerstedt, 2019). This re-conception of health behaviour has implications for preventive efforts and methodological consequences for how to design and represent research on athlete health behaviour. We have used storying as one method to capture and represent temporality. While the findings of the study are based on a small and diverse group of elite athletes, naturalistic generalisations can be made (Smith, 2018). Thus, we believe our findings can speak to athletes, coaches, and policy makers. A methodological challenge that comes with involving exclusive research samples in longitudinal qualitative research – such as the here presented study – is that careful choices need to be made regarding which personal and contextual information can be made public without revealing participants’ identity (Schubring et al., 2019a). While prioritizing confidentiality can limit the contextualisation of presented findings, we argue this choice is both indispensable for continued ethical research in elite sport and justifiable because social science research's prime interest is with social practices, interactions, systems and their people rather than individuals per se.
Conclusion and implications
The aim of this study was twofold: to identify ecological factors that influence athlete health behaviour, and to conceptualise the ecology of athlete health behaviour during the OG qualification phase. To reach these aims, we used a qualitative longitudinal case study design (Neale, 2020) and ecological systems theory (McLeroy et al., 1988). Through four non-fictional short stories, we showcased how Olympic hopefuls navigated through the qualification phase by practicing both health-risking (competing injured, training with pain) and caring behaviour (prioritising healing, careful weight management). Responding to aim one, on a case-to-case base, we outlined the ecological influences that jointly contributed to the identified health behaviour. Referencing our theoretical framework, we distinguished between intrapersonal, interpersonal, organisational, community and policy influences, but also identified an additional layer, namely time, as key influencers. For aim two, we aggregated the case-based factors of influence into an empirically grounded model of the ecology of athlete health behaviour, which we conceptualised as a dynamic interplay between athletes and their context, involving multi-level barriers and support factors, which influence athletes’ navigation between risk-taking and self-care in non-linear ways.
Building on these findings, we suggest that ecological theories are valuable means to gain a fuller understanding of the multiple interrelated factors and social processes that influence athlete health. As others have argued (LaVoi and Dutove, 2012; Spaaij, 2014), the benefit of ecological perspectives lies in the synthesis of micro-, meso- and macro-influences, which enables a more comprehensive explanation of social phenomena. Such fuller understanding is important for sociologists of sport and practitioners alike. Further, social ecological theories, in contrast to a range of other sociological theories (Turner, 2008), have the potential to account for both individual agentic and structural influences on human behaviour instead of either/or. They may also challenge and expand the ‘sociological imagination’ (Mills, 1959) in fruitful ways by drawing attention to the roles personal (including bodily) and temporal dimensions, and natural/non-human environments, play in the formation of identities, practices, and organisation in the field of sport.
Regarding research needs, we encourage sociologists of sport to further explore positive health behaviour and self-care in athletes. More specifically, knowledge as to how organisational, community, and policy processes can counter athlete precarity and limit dependency from funders and coaches is important. The latter can require multi-sited methodologies, and the involvement of stakeholder groups situated beyond athletes’ direct training context.
For Olympic athletes to be able to deal with qualification situations in healthy and sustainable ways, we want to highlight the following:
Sport organisations should adopt long-term planning and close follow-up of athletes’ health and wellbeing prior, during and after OG qualification phase. Such follow-up together with smooth and affordable access to medical services and policies that limit organisational conflicts of interests will help prevent health problems and increase athletes’ chances to qualify.
Coach and other support personnel should be aware of their meditating role in athletes’ ecology and be empowered to identify risky/caring health behaviour in athletes and critically reflect on the consequences with athletes. Using storied cases in coach education could be a way to work and to develop these capacities in coaches.
Athletes should be made aware of the ecology they are part of and be given possibilities to critically reflect on their own health behaviour, its causes and consequences. Surrounding themselves with people who promote caring health behaviour could help athletes to listen to their inner voice, to address problematic power relationships or raise issues that require change on an organisational level.
Footnotes
Acknowledgements
The authors thank the study participants for sharing their experience. They acknowledge Geraldine, Erik and Lisa, and thank the anonymous reviewers for their insightful comments on an earlier version of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partly suppported by the Swedish Research Council for Sport Science under grant P2017-0026.