
Abstract
Several studies have examined the provision of medical care in a variety of competitive sport settings. These are important contributions, but the majority of this work has focused on elite sports that tend to have a group of medical health professionals as part of the team, with little attention given to sports that lack access to such services. This lack of dedicated medical support may result in athletes being more likely to engage in ‘team-doctoring’ – a term used to describe athletes seeking medical advice from teammates and coaches. This concept is yet to be theorised and empirically described. In this paper, we begin to define, explore and contextualise the process of team-doctoring in relation to sociocultural interactions, beliefs embedded within the combat sport subculture and the critical role it plays in shaping fighters’ perceptions of health and injury. In so doing, we demonstrate that team-doctoring is the process whereby apparent medical knowledge is (mis)understood, recommended, transferred, interpreted and developed within a somewhat coherent team.
Introduction
A number of sociologists have convincingly argued that sport often occurs in a cultural context that can serve to normalise and glorify risk, pain and injury (Frey, 1991; Hughes and Coakley, 1991; Malcolm, 2006, 2009; Matthews and Channon, 2016; Matthews, 2020; Nixon, 1992, 1993; Theberge, 2006: 127). Nixon (1992) described this as a ‘culture of risk’ that is effectively mediated to athletes via social networks called ‘sportsnets’ that reinforce ‘cultural and interpersonal messages exhorting and encouraging them to play with pain or injuries’. In this regard, several scholars have explored elements of the medicalisation of sport and the athletic body to understand sociocultural factors that shape athletes’ perceptions and experiences of risk, pain and injury (Malcolm, 2006, 2009; Malcolm and Sheard, 2002; Roderick et al., 2000; Safai, 2003; Walk, 1997, 2004). These studies provide valuable insights into the relationships between athletes and medical care providers, which appear to play a central role in medics’ ability to negotiate different options for treatment. However, with the exception of Pike (2005), Liston et al. (2006) and Matthews (2020), little attention has been given to competitive sports that have limited access to medical professionals.
This is particularly the case in combat sport settings, where ‘fight medics’ are often outsourced and usually only present during fight nights (Channon, Matthews and Hillier, 2019, 2020a, 2020b). This is interesting, especially given that public debates around the safety of combat sport have a long history (British Medical Association (BMA), 2007; Murphy and Sheard, 2006; Rudd et al., 2016; Sheard, 1997). Yet the majority of studies in this area are largely based on systematic reviews that examine the incidence of injuries (Gartland et al., 2001; Jensen et al., 2017; Strotmeyer et al., 2016), rather than medical provision within combat sports. While Channon, Matthews and Hillier (2019, 2020a, 2020b) provide some interesting accounts from the perspective of medical staff, there is still no work which considers these issues from the perspective of fighters.
Safai (2003) argued that a lack of access to medical professionals may result in athletes being more likely to engage in ‘team-doctoring’ – a term she uses to describe athletes seeking medical advice from teammates and coaches. Such interactions might lead to usually well-intentioned ‘medical’ advice being either wrong, misinformed or lacking in important ways. This is similar to Freidson’s (1960: 377) ‘lay referral system’ which describes an informal network of lay people that may influence an individual’s attitude towards illness and formal healthcare. ‘Team-doctoring’ has yet to be thoroughly theorised or empirically described. Considering this, and the apparent transient nature of medical relationships in combat sports, it seems fitting to study this form of lay sports medicine within such settings. To develop some useful ideas to frame this work, we discuss the construction of medical knowledge and its possible sociocultural implications within sporting contexts.
Lay knowledge and thought collectives
In his pioneering work Genesis and Development of a Scientific Fact, Ludwick Fleck ([1935] 1979: 38) argued that medical knowledge is the outcome of a collective process and communication amongst members of a ‘thought collective’; defined as ‘a community of persons mutually exchanging ideas or maintaining intellectual interaction’. Within a thought collective is a small core of ‘special experts’, surrounded by a larger circumference of ‘laymen’, ‘educated amateurs’ and/or ‘general experts’ (Fleck, [1935] 1979). According to Löwy (1988), in a medical context this knowledge is constructed through the exchange and circulation of ideas and practical experience amongst specialists, general practitioners and patients.
Members within a collective are connected via a shared ‘thought style’ which serves as a ‘special carrier for the historical development of any field of thought, as well as for the given stock of knowledge and level of culture’ (Fleck, [1935] 1979: 38). Fleck ([1935] 1979: 92, our addition in brackets) also argued that ‘the adoption of one thought style (likely) excludes the simultaneous take up of a different one’, suggesting that no communication or exchange of ideas can arise between different collectives. His work also structures the passing of knowledge as flowing from the top down – that is, from experts to the public. Both these ideas have been explicitly and implicitly reconsidered in more recent developments of this work (Cobley and Sanders, 2007; Freidson, 1960; Löwy, 1988; Mößner, 2011; Peine, 2011).
In this light, Arksey’s (1994) work on the role of ‘lay experts’ in the social construction of repetitive strain injury (RSI) offered a valuable assessment of Fleck’s ([1935] 1979) analysis. Arksey (1994: 455) argued that ‘lay persons introduced doctors to a different way of thinking’, which was evident in the various ways in which RSI sufferers had an influence in shaping their physicians’ medical ‘fact building’ knowledge. Some physicians acknowledged their patients’ subjective experience with the illness and integrated this ‘lay expertise’ into their understanding of the condition. This communication between RSI patients and their physicians demonstrates that knowledge exchange, in some cases, can be less hierarchical than Fleck ([1935] 1979) originally suggested.
Other studies of medical lay knowledge indicated similar findings (Busby et al., 1997; Prior, 2003; Sarangi, 2001). Notably, Prior (2003) examined the limits of lay expertise. His work showed that lay people could effectively identify aspects of change in existing symptoms, but had almost no knowledge of disease processes that lie behind them. As such, their experiential knowledge was partial and restricted to symptomatic features relevant to their lives.
Taken together, these studies highlight several issues associated with the medical ‘expertise’ of lay people. Arksey’s adoption of Fleck’s conceptualisation of ‘thought collectives’ provided a useful analysis for understanding and assessing the social and cultural influence of lay people in knowledge construction. In relation to team-doctoring, these ideas help us conceptualise how experiential knowledge is developed within a group setting with various cultural influences. As a means of further developing these ideas and aligning them with research within sporting context we discuss sportsnets in more detail.
Sportsnets as thought collectives
Nixon (1992) argued that when network relations within a sportsnet are larger, closer, denser, more centralised, higher in ‘reachability’ (to prominent members) and relatively homogenous and stable, athletes are more likely to be deeply embedded in an environment that fosters health-compromising behaviours. Membership of such sportsnets works to instil norms and values that pressure athletes to play through pain and injury. Furthermore, Liston et al. (2006: 392) also noted that even in a ‘relatively small, loose and not highly centralised’ sportsnet, athletes could still become normalised to the notion of ‘playing hurt’.
Conversely, several sociologists interested in medical care of athletes have demonstrated how greater flexibility, heterogeneity and looseness in the social formation of sportsnets can result in players aligning less completely with the risk-taking and health-disregarding norms (Killick et al., 2012; Malcolm, 2006, 2009; Safai, 2003; Walk, 1997, 2004). For example, Walk (1997, 2004) showed that some student athletic trainers (analogous to physiotherapists in the UK) formed close friendships with players, which enabled them to undermine the ‘exploitative’ tendencies of sportsnets. Similarly, Safai (2003) concluded that the ‘culture of risk’ that dominated elite collegiate sporting environments could be countered by a ‘culture of precaution’ which helped coaches and athletes resist the promotion and tolerance of injury.
A key dimension to the processes described by Walk (1997, 2004) and Safai (2003) is the socialisation of athletes. Kotarba’s (1983) study of chronic pain among professional athletes is an excellent example. His conception of athletic subcultures was based on ‘a social network utilised by professional athletes to ‘make sense’ of illness and injury problems in confidence’ (Kotarba, 1983: 151). Specifically, he found that athletes – with similar experiences and problems – played a vital role in circulating information and methods that pertain to disguising pain and returning to play as quickly as possible. This is an example of lay knowledge passing between athletes in order to assess and manage their pain and injury. There was a social structuring to this knowledge which resulted in players who submit to pain and/or injury often becoming stigmatised. In this regard, the athletic trainers in Kotarba’s (1983: 159) study categorised players as ‘gamers’ and ‘nongamers’. They preferred to deal with ‘gamers’ because they consulted them when they were ‘really in pain’. In turn, they tended to avoid ‘nongamers’, because they were perceived as malingerers.
Considering the forgoing discussion, Nixon’s (1992) notions about ‘sportsnets’ clearly resonate with key elements of Fleck’s ([1935] 1979) ideas on ‘thought collectives’. Nixon (1992: 130) identified athletes as ‘receivers rather than sources’ of information within their sportsnet, which aligns with Fleck’s unidirectional circulation of knowledge within a thought collective. Also, Nixon (1992: 133) stated that ‘contacts in dense networks with a homogenous culture tend to be mutually reinforcing’. That is to say, when athletes are deeply embedded in such sportsnets, various members of that group are likely to reaffirm similar normative ideas, which means that they are less likely to voluntarily seek information from alternative sources. This reinforcement and circulation of norms and values can be explained by a shared ‘thought style’. Within these ‘dense’ thought collectives, members are less likely to adopt more than one thought style; as such, we might expect cultural messages around accepting risk and unhealthy practices to go largely unchallenged.
When taken together, the preceding comments highlight: (a) the potential importance of the as yet under-theorised and under-reported notion of team-doctoring for further understanding athletes’ health and risk related practices; (b) the potential utility of aligning ideas about ‘thought collectives’ and sportsnets as a means of framing the production of lay knowledge within the process of team-doctoring; and (c) combat sport social spaces which might offer interesting organisational distinctiveness which means they provide opportunities to empirically detail ‘team-doctoring’. After a brief discussion of methodological issues, the remainder of this paper explores data that is useful for considering these interlinked points.
Methodology
Initial entry to the field was mainly established through the first author, AlHashmi’s, personal contacts and individual rapport. Her active involvement in the Muay Thai scene for over 6 years, as a spectator and participant (7 wins, 2 losses, 0 draws), made it relatively easy to identify with and access members of that particular community. As she can conform with the cultural norms within such spaces, her acceptance as a cultural ‘insider’ was simple. This provided relatively unhindered access to observations and interviews with key members of the community.
It is perhaps useful to point out that AlHashmi has been training and fighting Muay Thai for years before partaking in this project. But in order to continue her ‘personal’ involvement in the sport and balancing it with her PhD commitments, she has since joined a fight gym closer to the university where this research is being conducted. AlHashmi was able to quickly establish trusting relationships with ‘core’ members after training there regularly for around five months. This also coincided with the time she started representing the team in competitions, which demonstrates to some degree her acceptance as ‘part of the team’. As such, part of her new-found affiliation as an ‘active’ fighter for this club meant that she was often a member of their corner/backstage team at combat sport events. This type of access provided her with another sample source predominantly through informal chats with potential participants backstage. Also, since this study is part of a larger project, the majority of her observational access focused on shadowing ringside medical personnel in combat sport events, and, because she was situated at the ringside, she was able to establish relationships and build rapport with referees, coaches, fighters and judges who typically also had experience in other aspects of combat sports. Therefore, by utilising these forms of access, a snowball sampling method was used to help increase the number of participants.
AlHashmi’s identity as a fighter played a central role in leading the data collection for this study. However, as a Middle Eastern, Muslim woman, researching in a western setting that is predominantly masculine and white, we were aware that her presence might alter some established patterns of interaction. However, through her continuous and active engagement with people within such spaces, she started to develop similar speech patterns, mannerisms and cultural norms that pertained to that group. It is important to note that those behaviours were not intentionally adopted for a desire to ‘fit in’; rather, they were primarily part of a normal socialisation process that mediated, maintained and reaffirmed her membership, and that of others, to that subculture. With that, her cultural differences, although present, became less apparent.
Given AlHashmi’s embodied involvement in the sport, Elias’s (1987) ‘detour via detachment’ (also see Matthews, 2015, 2018) was used as a means of reflecting upon the data used in this project. This was mainly managed through lengthy discussions with the second author, Matthews, about how her position in the field as a fighter contributed to shaping the co-production of knowledge at various stages. This enabled her to be aware of moments when she had normalised certain health-compromising practices such as enduring physical damage (e.g. repeated blows to the head) and engaging in potentially dangerous weight-cutting methods. These conversations were designed to ensure that AlHashmi was able to critically ‘see’ such practices and their social production within the spaces she was so comfortable within; in other words, to ensure the ‘familiar’ could become ‘strange’. We had some notable successes during this process, but this does not change the fact that AlHashmi occupied an ‘insider’ or involved position and this should be considered when assessing the strengths and limitations of the data.
In certain situations (e.g. gaining access), AlHashmi status as a fighter largely preceded that of researcher. By presenting herself as a fighter and having the physical skills to back this up, we believe that participants were more comfortable to speak about certain experiences and/or ‘controversial’ issues that might be left unspoken in the presence of cultural ‘outsiders’. In this regard, AlHashmi was able to align herself with participants’ experiences of injury and health-compromising behaviours. While being a fighter is not a prerequisite for conducting such research, nor does it provide some sort of privileged insights; we argue that it did give opportunities to easily gain access to experiences which might have been more challenging to collect for someone with less experience of combat sports.
In total, the interview sample comprised of fighters from different combat sport disciplines (n=39 + 7 supplementary) including Muay Thai (13 male, 6 female), kickboxing (4 male, 1 female), mixed martial arts (MMA; 2 male, 1 female), boxing (5 male, 1 female) and Brazilian Jiu-Jitsu (BJJ; 2 male, 4 female) with some being active fighters and coaches (n=6), coaches/referees (2 males, 1 kickboxing/boxing and 1 Muay Thai) and ringside medical personnel (2 males). Interviews averaged around 30 minutes and took place in various locations such as private areas in cafes, backstage at events, university meeting rooms, quiet corners in gyms, and venue lobbies. Interviews were recorded with the consent of the interviewees and transcribed as soon as possible. Interviewees were assigned pseudonyms to ensure their anonymity. None of the fighters interviewed in this study had access to club-affiliated medical support. It is also important to note that although the larger study included interviews with referees and ringside medical personnel, that data was not explicitly addressed in this paper. Biographical details for all interviewees cited in the text is provided in Table 1.
Biographical details of interviewees.
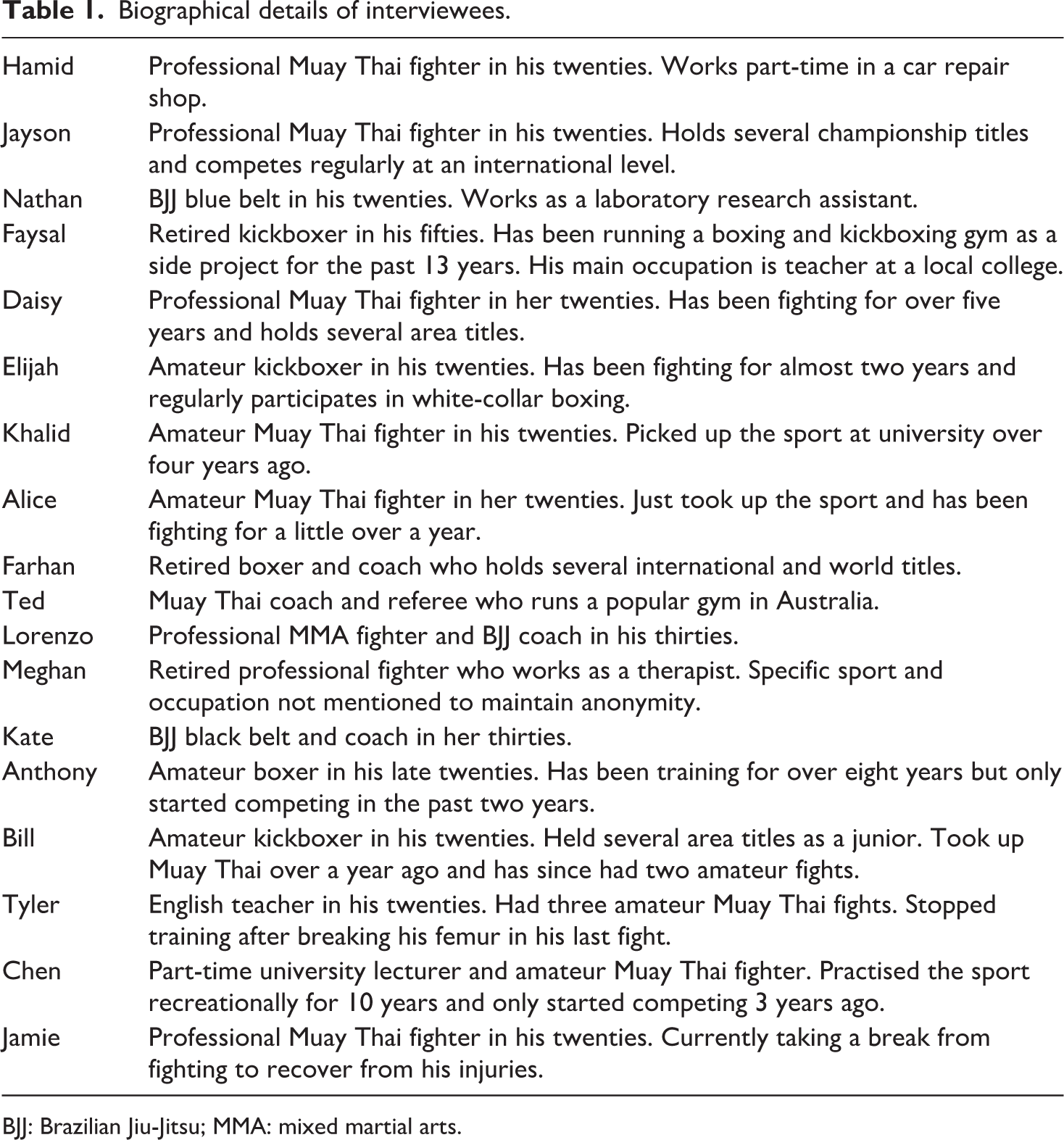
BJJ: Brazilian Jiu-Jitsu; MMA: mixed martial arts.
One hundred and seventy-nine hours were spent conducting observational research across 18 combat sport events (162 hours, 5 multidisciplinary, 1 MMA, 4 boxing and 9 Muay Thai/kickboxing) and training/sparring sessions (17 hours, across 3 gyms, 1 MMA/boxing and 1 kickboxing/boxing, and 1 mixed discipline). Alongside this, AlHashmi trained in a fight gym 5 to 6 times a week for around 2 to 3 hours each day over the course of 18 months. Data was mainly recorded as field notes typed on AlHashmi’s phone with the participants’ consent. As with the interviewees, the observed participants were given pseudonyms.
This data was analysed through a process informed by Blumer’s (1969) discussion of ‘sensitising concepts’. Prus (1996: 132) neatly captures our use of these ideas:
Blumer uses the term ‘sensitising concepts’ to refer to these tentative, analytical notions. Sensitising concepts suggest subsequent lines of inquiry and assessment, but in each case the researcher has the obligation of making the concept match up with the circumstances at hand rather than making the data fit the concept.
In this regard, Blumer encourages scholars to ensure a relentless interaction between their academic ideas about the social world and data. In order to produce findings which are informed by concepts, the specifics of this process resulted in us meeting regularly during the data collection period. During this time, AlHashmi was surveying relevant literature in the field while also comparing and contrasting the ideas embedded in this work to the experiences, thoughts and ideas of her participants. Matthews largely acted to encourage clarification over the use of concepts and data. This often took the course of lengthy discussions where the limitations of both data and extant concepts within the literature were reflected upon. This process highlighted apparent gaps in the literature which could be neatly addressed by the data that was being collected and also opportunities for conceptual refinement and redevelopment. We now turn to this data as a means of outlining some key findings in relation to the notion of team-doctoring.
Team-doctoring in combat sports
Team-doctoring is the process whereby apparent medical knowledge is (mis)understood, recommended, transferred, interpreted and developed within a somewhat coherent team. While there might be more or less opportunity for those with formal medical knowledge to influence this process, the term is most usefully applied to groups of athletes who exist in relative isolation, for one reason or another, from formal medical expertise. Within these teams, gyms, groups or sportsnets, what Fleck would call a ‘thought collective’, we can see the generation of a ‘thought style’ which shapes the way individuals think about and attempt to manage various injuries and illnesses associated with their participation in the sport. We will unpack these assertions in what follows.
Ordinary ‘run of the mill’ ways of thinking about risk and (ill) health shaped the process of team-doctoring. As with other research on similar sporting spaces (Curry, 1993; Hughes and Coakley, 1991; Matthews, 2020; Waldron and Krane, 2005), symbolic messages that normalised certain health-compromising behaviours were accepted as ‘part of the game’.
This was evident in the way most fighters rationalised their experiences of pain and injury. These three examples are indicative:
Hamid: [Injuries are] something us Muay Thai fighters class as normal. I presume that being in that gym, it’s something that you gotta take up the chin. You know, Muay Thai is known to be a hard man’s sport meaning if you get injured, you got to weather the storm kind of thing. If you watch traditional Muay Thai, it’s not about who is the most technical but it’s who’s the toughest. It’s who’s the last man standing Jayson: So, you’re always going to be sore. There’s always going to be something. You’re never going to be 100%. There’s always going to be something that comes up. You’re going to be sore. You’ll have a little injury. You’re going to be tired. You just gotta learn to deal with it Nathan: You’ve been in the ring yourself, like you’re not meant to show any like reaction, like, you know, when you check a kick and your face is all like ‘oh that didn’t hurt’ you know. So you don’t acknowledge the pain, you don’t acknowledge them for landing a good strike. You know, you have to seem invulnerable. It’s the combat sport mentality, innit? You have to be the toughest motherfucker in the room.
Waddington (2012) suggests that athletes’ efforts to deal with risk, pain and injury are likely to reflect beliefs held by prominent members of their sportsnet. This was mostly evident in gym observations, where coaches frequently communicated their expectations of what their fighters must do to remain in the sport. Take Faisal’s speech to his fighters after what appeared to be an unforgiving sparing session:
Stop feeling sorry for yourself. We are all injured. It is how it is. You’re not fuckin’ Gavin or Sally trotting on a horse for a dressage rehearsal on a Sunday morning are you? We’re fuckin’ fighters. See the difference? If you’re 100% when you fight then you’re doing it wrong. When I’m injured I take it as an opportunity to work on other things. There is always a way round it. No one is gonna feel sorry for ya on fight night. (Fieldnotes, winter 2020)
This is one way that coaches were able to shape the ‘thought style’ of their team. Most of the fighters in this study tended to accept these health-compromising norms. As such, it appeared that they mainly understood how to manage the injuries that seemingly followed these practices by turning to their team for advice, support and ‘medical’ knowledge.
Within these relatively stable sportsnets the coaches were usually on hand and easily approached by the athletes – in Nixon’s (1992) language, ‘reachable’. The fighters found the coach’s experiences of pain and injury relatable and tended to trust their advice over that of medical professionals. This appeared to be connected to the time they spend training together. Jayson’s thoughts about his coaches captures this really well:
100%, 100% I trust my coaches more. They train with me every day. They watch me. And they’ve been in the sport. They’ve done it themselves. I go to a doctor, obviously, they know what they’re talking about when it comes to the human body but never met them before. They’ve never seen me train, they’ve never seen me fight. They don’t know who I am or anything.
This kind of relatively unrestrictive access to someone with what we tentatively call ‘expert lay knowledge’ stood in sharp contrast to the fighters’ lack of access to formally qualified medical experts.
Unlike much of the published literature on the medical supervision of sports, where athletes can draw on medical advice from various sources (Safai, 2003; Walk, 1997, 2004), the fighters’ access to medical care was predominantly through their primary health care providers (general practitioners) – who are not part of their sportsnet. Interestingly, the fighters did have access to ringside medical personnel at fight events during pre-fight screening; however, the tone for these interactions was often shaped by the need to be passed as ‘fit to fight’ which encouraged them to hide or otherwise downplay any medical problems (see Channon, Matthews and Hillier, 2020a for a more fully developed discussion around this topic).
The majority of fighters interviewed in this study considered their coaches to be experts in the sport:
Hamid: Well, in a training camp or in any gym you realise that the coach is the backbone. He knows the ins and outs. He’s been there, he’s done that. He’s seen things happen. He knows the best. All over, he’s the top guy. Daisy: So, he’s my coach, so within that dynamic, within the gym and that relationship that you have with someone who’s – he’s the head honcho, he knows. He’s been there, done it.
These statements neatly align with Fleck’s ([1935] 1979) notions about ‘special experts’ being classed as main sources of knowledge within a thought collective. In this way, despite coaches not being medical experts in any formal sense, they played a pivotal role in team-doctoring, as fighters tended to rely on them as their first point of reference for obtaining information about injuries and sport-related health issues.
While team-doctoring is not limited to coaches, the athletes in this study felt more comfortable approaching them. Ryan’s statement is particularly illustrative: ‘I’d only go to them [other fighters] if they’re like really, really experienced and been around for as long as my coach like, do you know what I mean? But in general, I’ll just go chat to my coach.’ It appears, then, that previous experiences (or, in Matthews’ (2020) terms, ‘experiential knowhow’) were an important qualification to occupy a central position within team-doctoring.
Given that the coaches had more experiential knowledge in the sport, their fighters assumed that they were familiar with common injuries. And when AlHashmi pointedly questioned their ‘medical expertise’, fighters were often quick to defend them:
AlHashmi: Why do you think he [coach] knows all those stuff about the body? Elijah: Probably because he’s probably experienced most of it being a fighter. I don’t know, but he was obviously a coach for loads of years as well. He’s probably seen it all. AlHashmi: Even if he’s not a medical person? Elijah: Yes, even if he’s not a medical person. He’s still got the knowledge of everything. He may not be qualified in it, but I think he’s still got the knowledge. AlHashmi: Is he [coach] a medical person? Khalid: I mean how do you define who’s a medical person? [laughs] I think he is in what he does at least. He was a professional Thai boxer when he used to compete, he was a world champion facing up toughest people on the planet. And so, I think he does know the, you know, the body pretty well, how it reacts in a fighting situation.
These statements illustrate that the fighters accepted their coaches’ lay expertise in sports medicine by associating it with their embodied experiences as current and former fighters.
Some fighters even attached medical terms to their injuries based on their coaches’ ‘lay diagnosis’. For example, Alice revealed how her coach ‘diagnosed’ her with ‘fluid retention’:
AlHashmi: Was that fluid retention diagnosed? Alice: My coach told me so. But I trust him. AlHashmi: Why do you trust him? Alice: Mainly from his own fighting experience, years of professional fighting, and years of coaching professional fighters. It’s something he’s come across very often and he explained why it might happen to me and it’s more common in people with higher levels of oestrogen. So that fit me. [laughs] AlHashmi: Does he have a medical background? Alice: No, he doesn’t. So, I guess I wouldn’t say it was a medical diagnosis, it was just I didn’t feel like I needed a medical opinion on it, because it wasn’t influencing any other part of my life, just my training. Also, my dad’s a doctor so sometimes I’d ask him things, but not all the time cause sometimes, he just – he goes over the top.
The coaches acknowledged that their experiential knowledge in both fighting and coaching have helped them recognise and manage certain injuries sustained by their fighters. This was particularly evident in conversations about concussion:
Farhan: I think because I’ve had that experience, I feel like I’ve dealt with it [concussion] better because even if they [fighters] haven’t even told me, I’ve noticed it, I’ve seen their eyes, I’ve seen them dazed. Ted: Concussions, you know . . . it’s a very untapped subject. I know how to pick it, one of my fighters has got it.
These examples indicate the important place that the coaches’ long-term engagement in the sport play in the development of lay knowledge around risk, injuries and (ill) health, which also served as a key element of the socialisation of athletes into these sportsnets. This process of ‘medical’ lay knowledge exchanging and developing across generations of fighters and coaches is a hallmark of team-doctoring and aligns neatly with Fleck’s ([1935] 1979) conceptual analysis of the circulation and maintainence of thought styles within ‘dense’ thought collectives. Indeed, Freidson (1960: 377) argued that ‘the extensiveness of the lay referral structure has relevance to the channelling and reinforcement of lay culture’.
The choice to seek medical advice from coaches was largely a function of ease of access in combination with an assumption that the coach would have context-specific advice due to their personal experiences in sport. As such, the fighters hardly had any contact with formally qualified medical personnel, and rarely spoke about them; when they did, these doctors were often classed as outsiders due to their lack of apparent ‘fight’ knowledge and experience:
Nathan: They [doctors] don’t let you work around something you truly know that you can work around. I think the problem is that they won’t even let you try work around it. So, I think most people don’t wanna go to a doctor because they kind of already had this preconceived notion that the doctor is just gonna tell them to stop doing what they love. And obviously they’re not gonna stop doing what they love, so they stop going to the doctor. Lorenzo: Doctors always want you to stop, it make their job easy. I actually think some doctors are pretty lazy. All they say is put ice and rest. I don’t need to rest. I need to go fight so fix me. [laughs] Do you know what I mean? Give me a solution, give me something.
This ‘preconceived notion’, described by Nathan, was a commonly occurring element of the thought style that the fighters developed from their interactions with the sportsnet. In this regard, fighters almost always associated ‘doctors’ with treatment options that prevented them from fighting, which is why they tended to avoid them. In turn, fighters favoured team-doctoring because they knew that the knowledge they would gain was more likely to enable them to ‘work around’ their injuries and continue to compete.
Interestingly, there were exceptions that in some ways ‘proved’ this rule of fighters valuing lay knowledge. On some occasions, fighters would seek advice from fellow members who held relevant medical qualifications. Meghan, a retired fighter and qualified therapist, provided a good example of this:
AlHashmi: Did people at the gym ask you for general medical advice or like how to deal with certain injuries because you’re a therapist? Meghan: All the time! [laughs] Yeah, yeah, all the time. Ever since when I was first training to be a therapist.
Meghan later explained that this was one of the reasons why most of her patients happen to be fighters: ‘I think, partially because I was a fighter, I mean, I know one of the reasons that people come to see me is because they trust that I would understand what they need to be able to do.’
While it was relatively rare for members of martial arts clubs to have medical qualifications, on occasion this was the case. Due to their connection to these sports, these formal medical personnel, or in Fleck’s ([1935] 1979) terms ‘general experts’, were not seen as outsiders and their knowledge was often welcomed by fighters and coaches:
Kate: And also we have few doctors here in the gym, thankfully. So I usually consult with them and what would be the best course of action. So, they tell me I should see a specialist, or get a scan done then I do that. Faisal: We’ve got a doctor who trains in our gym sometimes, I sometimes speak to him. There’re times we’ve had injuries while training like in sparring if there’s an injury and if the doctor is in the room he actually puts on what we call ‘medical masterclass’ [laughs] and everybody gathers round while he explains the injury.
Such members not only shared medical advice but also offered their services when appropriate, both of which coaches and fighters seemed to take on board because, unlike primary healthcare providers and ringside medical personnel, they were considered as ‘fighters’ who were part of the team. And with this, members assumed that they were more likely to understand and comply with the team’s thought style in relation to largely valuing athletic performance over health.
A dimension of this process was that some fighters conducted a self-assessment of sorts in order to classify injuries as ‘serious’ or ‘playable’ before speaking with fellow team members:
AlHashmi: Did you tell the coach that you got dazed when he [sparring partner] caught you with that uppercut? Anthony: [scoffs] No, why would I? AlHashmi: Cause you just said that you tell him everything – Anthony: I do, but (long pause), it depends really . . . So maybe not everything, cause it depends how serious it is Cause you know getting into it that you’re bound to get hurt. It’s just how much your body can take on, you know? Like I can tell him if I want but I personally don’t. But I definitely tell him when something is getting serious, definitely. Jayson: It’s not that I hide, but I feel that it’s not necessary for him [coach] to know because . . . it’s because it’s part of the sport . . . you don’t have to tell him everything but, you know, if it’s a legitimate injury that will have an impact on your training of course you have to let him know so we can work around that.
Most fighters were generally inclined to share more ‘serious’ injuries and hide ‘playable’ ones. Curry (1993) evidenced that such behaviours were often encouraged in aspiring wrestlers. Similarly, Prior (2003) argued that personal motivations and experiences largely shape individuals’ lay understanding of disease.
Furthermore, and similar to Kotarba’s (1983) athletic trainers, some fighters revealed that they chose to hide certain injuries from their coaches, because they did not want to be stigmatised as ‘nongamers’:
Bill: Well I see him [coach] bollockin’ other guys at the gym sometimes and I think ‘I don’t want to be that guy’. Tyler: Even when I feel like death I go [to the gym], I always go. AlHashmi: So what will happen if you don’t go? Tyler: Dunno, but like my coach says showing up is half the battle and if you good enough to show up then you good enough to train, so yeah. AlHashmi: Even when you ‘feel like death’ – [both laughing] Tyler: Not like ‘death, death’ but you know how coaches can be like. AlHashmi: Yeah, but can you give me an example? Tyler: So you know how sometimes the coach takes a mick outta people who whinge a lot? So you sort of push through when you can cause otherwise you’ll be known as the gym’s ‘sick note’ and no one wants that.
In line with this, there was also a general consensus amongst fighters that their coaches might think that they were unfit to fight if they kept on returning to them for advice about recurrent injuries:
Bill: Like if I complain about something a lot he might think that I’m not good enough to fight or I am not taking it serious. Elijah: You don’t want to seem [pause] weak is the wrong word, but you don’t want to seem like you’re trying to get out of doing the work just because your leg hurts a little bit, but you can get through it. He’d think I’m not cut to fight if I come to him for every little thing.
None of the fighters reported not being allowed to fight because of ‘too much’ team-doctoring. However, such messages were clearly implied by their coaches during training sessions. This example from AlHashmi’s observations is particularly illustrative:
We were sat on the mats chatting as we wrapped our hands getting ready for sparing. The coach came and showed us a text message on his phone and said ‘look at that . . . what a load of bollocks’. It was from Oscar, it was the third time that he texted this week saying that he cannot come to training because of his shins. Nodding in disapproval, the coach then walked back to the ring and said ‘seeya Monday he says [scoffs] let’s see how his shins feel come Monday when I tell him that I’ve pulled him out’. (Fieldnotes, autumn 2019)
Collectively, these examples show that the athletes’ motives behind seeking team-doctoring are not only influenced by their interpersonal relationships with their coaches, but are also dependent on normative ways that their team thought about risk, pain and injury. This ‘thought style’ was developed over time and shared through chats, texts, and ways of behaving during and after training sessions.
In addition to hiding injuries, some fighters also expressed that they were more likely to seek team-doctoring from other athletes in situations where they thought that their coach’s advice did not fit their needs, which was apparent in conversations about weight cutting. For example, Chen chose to follow diets recommended by her female teammates despite the multiple health implications she had suffered by following their advice:
AlHashmi: Why do you go to the girls then? Does he [coach] not help you with your weight cut? Chen: He does, but it’s very basic. But my body is different than the young men [at the gym], what works on them doesn’t work on me. I’m a 44-year-old woman, you see? It’s not the same.
Like Chen, Jamie preferred to seek advice from a more experienced teammate because he thought that his coach’s weight-cutting methods were ‘dated’:
Jamie: Like, [teammate], he’s a Bellator [popular MMA promotion] fighter now, so it’s like the biggest show in Europe right now. He’s got experience though I can trust him. Plus, my coach, he’s a bit older. So when he was fighting the training methods and the weight cutting methods were a bit different, a bit older and could be a bit dated. Now [teammate] he’s up to date with everything. So I know he’s taking it 100% serious and I can trust him and his methods are most likely gonna be best for me as well cause he’s similar in height and stature and frame.
This aligns neatly with Prior’s (2003) examination of the limitations of lay experts in dealing with matters of health and illness by revealing how their ‘expertness’ will always remain invariably subjective to their own experiences. In a similar way, team-doctoring is dependent on the coaches’ lay experiences of pain and injury, and, when those experiences are no longer compatible, athletes choose to seek alternative sources within their fight collective.
Conclusion
Considering the preceding analysis, it is evident that the process of team-doctoring frames how knowledge of lay sport medicine is circulated, (mis)understood and internalised by athletes in somewhat isolated team settings. The purpose of this paper is not to evidence the fighters’ normative overconformity to health-compromising norms that dominate most competitive sports settings, but rather to describe the process of how they come to accept and rationalise those ideas, particularly in the absence of influences from cultural ‘outsiders’.
We have demonstrated that combat-sporting spaces offer an interesting avenue for this type of research given the lack of dedicated medical support in such social settings and where coaches dominate the power relations. Indeed, our data consistently revealed that team-doctoring is heavily structured and centralised around the coach’s lay knowledge and ‘experiential knowhow’. On its own, this element of our analysis echoes Fleck’s ([1935] 1979) unidirectional and hierarchical nature of knowledge transfer within thought collectives. But when aligned with Nixon’s (1992) notion of the sportsnet, we were better able to account for the nuances and complexities of this process as it plays out in a group setting. This analysis is further bolstered by weaving in ideas utilised by Kotarba (1983) and Prior (2003).
Pulling on these theoretical ‘threads’ has helped us to: (a) add theoretical utility to the notion of team-doctoring; (b) provide a conceptual frame which has neatly aligned with the observations and interview data collected by AlHashmi; and (c) demonstrate the continued importance of early work within the sociology of medicine (Arksey, 1994; Fleck, [1935] 1979; Freidson, 1960; Löwy, 1988) and sociocultural explorations of sport (Hughes and Coakley, 1991; Kotarba, 1983; Nixon, 1992, 1993) That such works still hold relevance in the contemporary world of sport demonstrates to us the stubborn nature of the problems we have tried to highlight within the paper. And we hope that others will find utility in the academic ideas we have drawn together here.
When Safai (2003) first introduced team-doctoring, she suggested that being involved in such a process might affect athletes’ expectations about pain tolerance and consequently their judgements about when to seek medical help. Indeed, we found that the ease of accessing knowledge from ‘lay experts’ played a key role in shaping the athletes’ medical ‘fact building’ about how to deal with risk, pain and injury. This contributed to the development of normative ideas about risk and (ill) health in the form of a shared ‘thought style’. As such, these interpersonal relationships are fundamental to how team-doctoring is structured.
Fighters sought out team-doctoring because it was geared towards maintaining and improving their athletic performance rather than general health-related outcomes. In connection to this, when fighters did require formal medical interventions they were largely disregarded and ignored. Similarly, in her work on female rowers, Pike (2005: 213) argues that this ‘communal sense of treatment seemed to be particularly relevant to athletes, for whom activity is central to their self-identity’. As such, this ‘culture of shared decision making’ was largely due to the lack of dedicated medical support along with the athletes’ perceived incompetence of ‘orthodox medical care’ in dealing with their sport-related health issues (Pike, 2005: 213).
The athletes we spoke with almost always gained medical knowledge from people without formal medical expertise. Team-doctoring neatly and efficiently filled in for such qualified advice. This can be problematic, since the basis of medical knowledge in ‘lay experts’ has been shown to be invariably idiosyncratic (Prior, 2003) and clearly open to error and inconstancy, and shaped by cultural ideas not informed by the Hippocratic Oath. This was evident in examples linked to the limitations of the coach’s experiential knowledge where fighters formed networks with one another similar to the ‘athletic subcultures’ described by Kotarba (1983) to try and ‘work around’ their individual issues.
While we are aware that the evidence in this paper implies that team-doctoring appears to be heavily coach-led, we need to keep an open mind as this is one of the first attempts at empirically contextualising this process. As such, it would be somewhat premature to further develop this argument without addressing the ‘teamness’ aspect of this concept. In this regard, it might be useful to explore how team-doctoring is structured in such settings where coaches are no longer the ‘special experts’. This type of athlete-to-athlete communication would show another dimension of team-doctoring that is yet to be fully explored. We have presented here a conceptual framework and initial findings which should help those interested in developing such analysis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.