
Abstract
This study aimed to determine the potential predictive value of four noninvasive anthropometric indices in screening for the risk of diabetes and hypertension in the Lao population. The data used for this study were collected as part of the National Health Survey which used the World Health Organization’s stepwise approach, covered 17 provinces and Vientiane capital, and had a representative sample of 3240 participants above 18 years old. Among the anthropometry indices tested, waist-to-height ratio (WHtR) had the highest predictive power for the prevalence of diabetes (area under the curve [AUC] = 0.73) and hypertension (AUC = 0.70). It is suitable for use in urban or rural areas and for fieldwork. The WHtR can serve as a public health and clinical screening tool, as there are no differences between sexes, ages, and ethnicities when monitoring diabetes and hypertension risk in Lao PDR, using the optimal cutoff point of 0.5 for both diabetes and hypertension.
What We Already Know
Prevalence of diabetes and hypertension is high, with many unaware of disease status.
Body mass index (BMI) is not a good indicator of obesity; nutrition research and policy are still inconsistent in the use of BMI as the obesity index.
Other studies suggest that local or at least Asian cutoff values should be used.
What This Article Adds
This is the first study to report the performance of the waist-to-height ratio (WHtR) in the Lao population; among obesity indices, it had the highest predictive power for the prevalence of diabetes and hypertension.
Although the Lao population includes many ethnic groups, the WHtR was equally useful in different ethnic groups.
We could show that there was no gender difference in the usefulness of the WHtR as an indicator of obesity and related risk of NTDs.
WHtR can be measured using a flexible measuring tape in both urban and rural areas.
A cutoff value of 0.5 has been shown to be effective predictor in detecting risk of diabetes and hypertension.
The cutoff value can provide a clear call-to-action message such as, “A healthy waist is less than half your height, so get moving and eat right”.
Introduction
The highest prevalence and mortality of non-communicable diseases (NCDs) are found in low- and middle-income countries, including Lao PDR. 1 The top ten causes of mortality in Lao PDR include stroke, which increased by 19.5% between 2009 and 2019, and diabetes, which increased by 30% in the same period. 2 Stroke and heart disease are both influenced by hypertension (HTA), diabetes (DM), and other lifestyle and behavioral risk factors. 2 In a recent Thai study, half of the patients with diabetes had HTA, whereas 14% of hypertensive patients had DM; 80% were unaware of their disease status. A similar situation prevailed in Lao PDR: only 42% of patients were aware of their DM and 29% of their HTA status.1,3 The co-existence of these two diseases is thought to increase the risk of cardiovascular disease. Overweight, especially abdominal obesity, is a strong risk factor for both DM and HTA. 4 It is useful to be able to identify persons at risk for these potentially serious conditions.
In Lao PDR, overweight and obesity are usually (but not consistently) measured using body mass index (BMI), despite evidence that BMI is not always a good indicator of obesity, and that it may need different definitions in certain populations. 5 Asian studies have recommended lowering the BMI cutoff that defines obesity, to be different from the standard used for Caucasians.6,7 Alternatives to BMI include waist circumference (WC) and waist-to-hip ratio (WHR), a simple obesity index for public health screening; a meta-analysis, mainly in Asian countries, suggested that waist-to-height ratio (WHtR) could be a simple noninvasive tool for identifying obesity and therefore cardiometabolic and DM risk with unisex cutoff.8-11
Identifying noninvasive indicators to screen for DM and HTA risk in low-resource settings is a priority topic in the Lao PDR health research agenda. 12 Research should inform strategies to prevent and control NCDs in both communities and hospitalized patients. 13 Information on suitable indicators is limited in Lao PDR. This study aimed to determine the predictive potential of noninvasive anthropometric indices: BMI, WC, HC, WHR, WHtR, and weight (with appropriate cutoff points for best indices and the standard indices), to screen for risk of DM and HTA in Lao PDR, to identify which should be recommended for future use in Lao PDR.
Methods
Study Area and Population
The data were collected as part of a national health survey, comprising a series of cross-sectional population surveys to track health status and risk factors and to provide information on the prevalence of NCDs such as DM and HTA in a representative sample of the Lao population. The survey covered 17 provinces and the capital city Vientiane, and included 3240 participants aged above 18 years, with proportional representation of males and females and urban and rural residents.
Study Design
A cross-sectional study was implemented between March and August 2020 (details in Supplementary material, Annex 1: Sample Size Calculation, Annex 2: Sampling Procedures, Annex 3: Field and Laboratory Procedures).
Data Collection
The six-member team of data collectors (nurses or other health workers) was trained to use the World Health Organization’s (WHO) stepwise approach 1 : (1) structured face-to-face interviews including socio-demographic questions; (2) physical measurements—blood pressure (BP), height, weight, and waist and hip circumferences; (3) biochemical measurements—fasting blood glucose (FBG) and HbA1c. Participants signed a consent form before interviews; they returned the next day for biochemical examinations, after fasting for 8 to 10 hours.
Definition of Variables
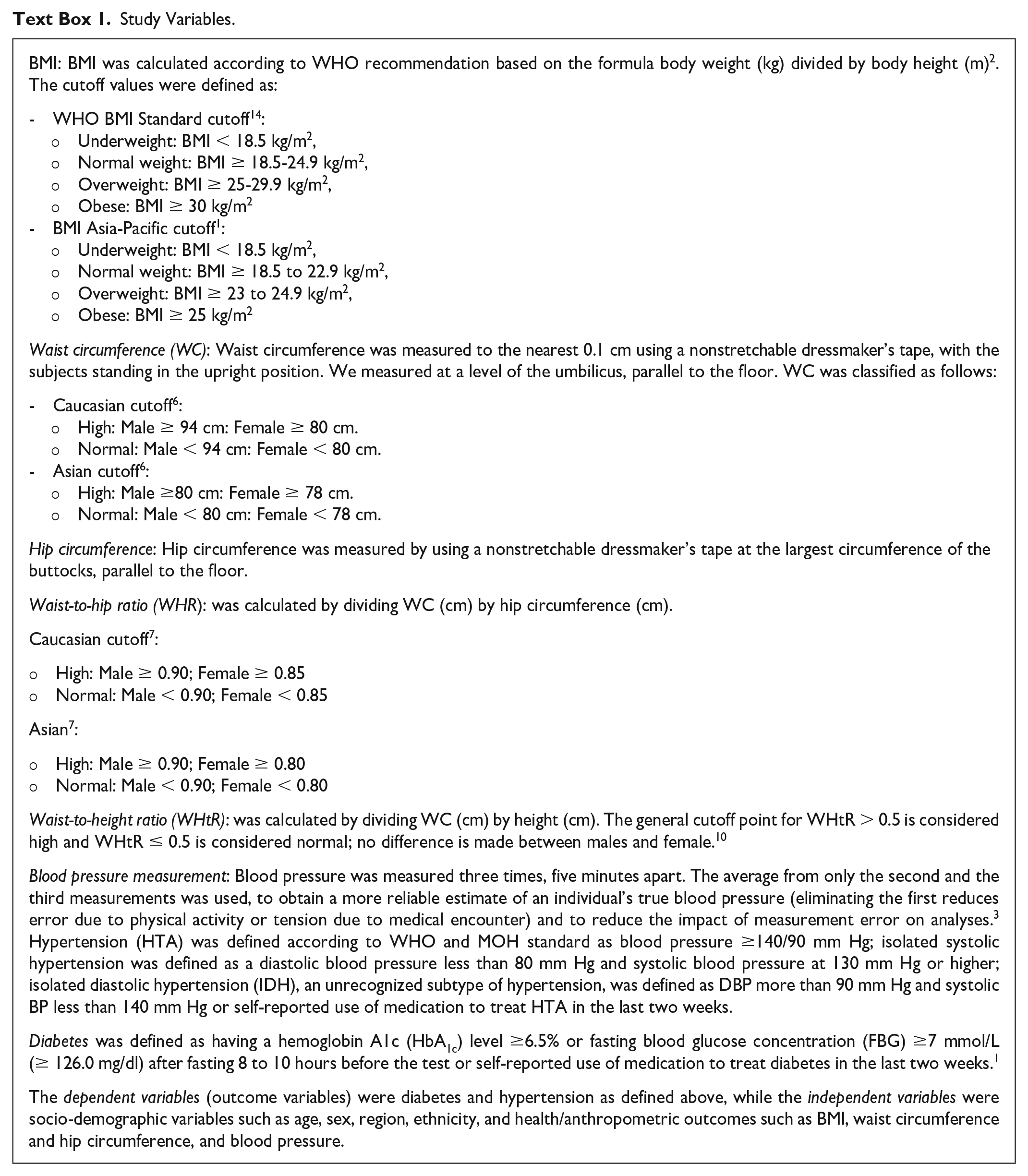
Standardized WHO definitions and cutoff values for variables have been used. See (Text Box 1) for more information.
Study Variables.
Statistical Analyses
Post-stratification weighting accounted for population distribution by districts, sex, and age groups from the National Population Census based on the 2020 National Census. Individual weighting was performed with the inverse of the probability of selection for each respondent, which was considered as the weight for the individual household. Receiver operating characteristics curve (ROC) analysis was performed to predict the sensitivity and specificity, of the studied measurements, using the Youden index (sensitivity + specificity - 1) 15 to calculate the optimal cutoff of anthropometry indices. The area under the curve (AUC) from the ROC analysis with 95% CI was estimated for six anthropometric indices (BMI, WC, HC, WHR, WHtR, weight). The ability of the different indices to identify the risk of DM and HTA was compared according to Hanley and McNeil 16 and the AUC prediction performance was classified as excellent (AUC ≥ 0.9), considerable (0.8 ≤ AUC <0.9), fair (0.7 ≤ AUC <0.8), poor (0.6 ≤ AUC <0.7), or failed (0.5 ≤ AUC <0.6). 17 All statistical analyses were performed using Stata for Windows version 17.0.
Results
Among 3242 participants, 1820 (58.22 %) were female; average age was 46 ± 14.65 years. Average weight, height, WC, and WHR were higher in males than females, but hip circumference and BMI were higher in women. There was no significant association between sex and the average obesity index (Annex 4).
Comparing BMI cutoff points used for Caucasians and Asians, the prevalence of obesity was >30% in both sexes using the Asian cutoff point, but only 4% (males) and 10% (females) using the Caucasian cutoff point. There was no difference between males and females using the Asian cutoff, but when the Caucasian cutoff was used, significantly more females were obese (P < .001) (Annex 5).
The mean weight of participants with DM only was 59.33 ± 12.38 kg, and for those with HTA only was 61.19 ± 12.19 kg. The mean BMI of individuals with both DM and HTA (26.07), HTA only (25.22), and DM only (24.35) was higher than that of healthy individuals (23.0). Similarly, WHtR was also higher among those with both DM and HTA (0.56), HTA only (0.54), and DM only (0.53) compared with the healthy group (0.50) (Table 1).
Characteristics of Obesity Index and Health, DM, HTA, and Both DM and HTA.
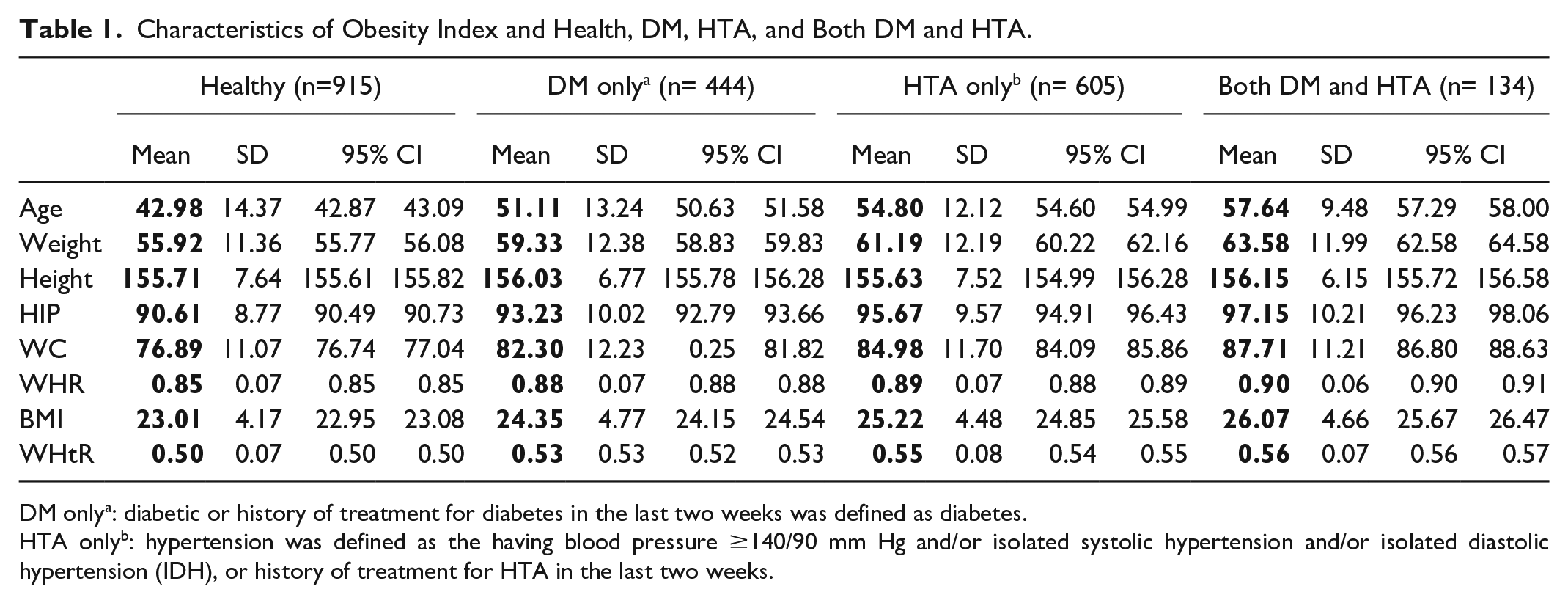
DM onlya: diabetic or history of treatment for diabetes in the last two weeks was defined as diabetes.
HTA onlyb: hypertension was defined as the having blood pressure ≥140/90 mm Hg and/or isolated systolic hypertension and/or isolated diastolic hypertension (IDH), or history of treatment for HTA in the last two weeks.
Prediction of DM: Sensitivity and Specificity
The WHtR was found to have higher AUC in predicting DM, based on HbA1c, than did FBG or combined HbA1c with FBG and treatment history. It was also better than BMI, with the AUC = 0.73; 95% CI [0.70, 0.76] for WHtR compared with AUC = 0.70; 95% CI [0.67, 0.73] for BMI (Figure 1).
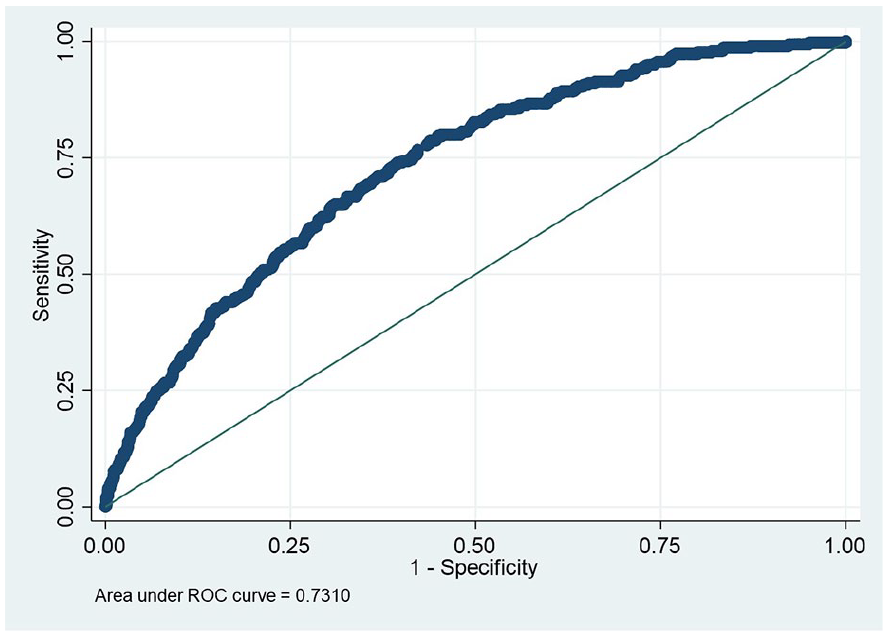
WHtR and DM (HbA1c), AUC = 0.73; 95% CI [0.70, 0.76].
Using the WHtR to Predict DM by Sex, Age Group, and Ethnicity
The WHtR had better performance in predicting DM in males (AUC = 0.77; 95% CI [0.73, 0.82]) than in females (AUC = 0.69; 95% CI [0.65, 0.73]). It could also better predict DM at a younger age (18-34, AUC =0.90; 95% CI [0.82, 0.97]) compared with older age (AUC = 0.71; 95% CI [0.68, 0.75]) for 35- to 60-year-olds and (AUC = 0.66; 95% CI [0.60, 0.73]) for >60 years (Annex 6).
Predicting HTA: Sensitivity and Specificity
The WHtR was also better than other anthropometry indices at predicting risk of HTA, with AUC = 0.70; 95% CI [0.67, 0.72] (Figure 2).
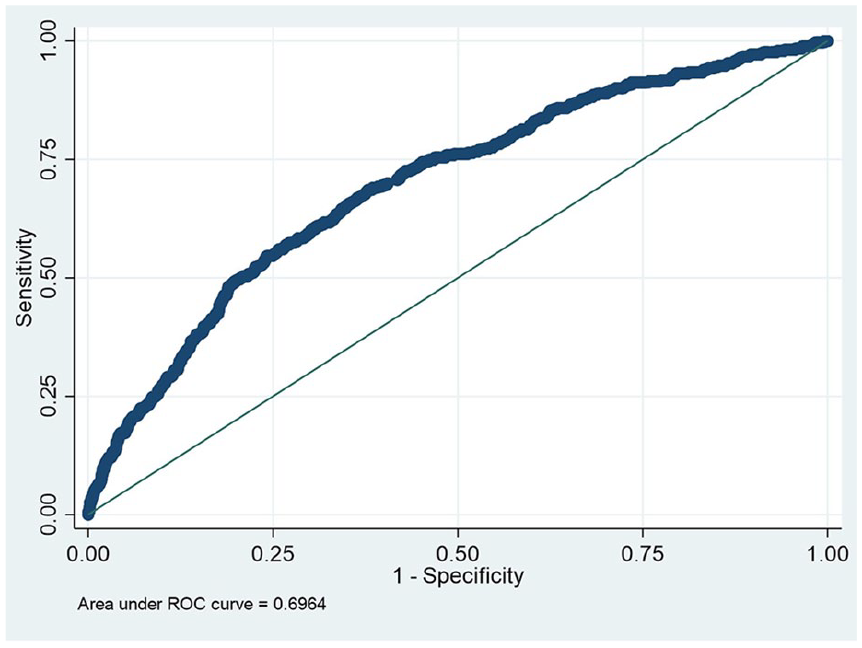
WHtR and HTA by measurement, AUC = 0.70; 95% CI [0.67, 0.72].
Using the WHtR to Predict HTA by Sex, Ethnicity, and Age Group
The WHtR is the better predictor of HTA in females (AUC = 0.72; 95% CI [0.69, 0.76]) compared with males (AUC = 0.67; 95% CI [0.63, 0.71]); in younger age (aged 18-34 years, AUC = 0.70; 95% CI [0.59, 0.81]) compared with older age (aged ≥60 years, AUC = 0.62; 95% CI [0.57, 0.68]) and in other ethnicities (Minority, AUC = 0.71; 95% CI [0.65, 0.78]) compared with Lao-Tai (Lao-Tai, AUC = 0.68; 95% CI [0.65, 0.72]) (Annex 7).
Optimal Cutoff Points for WHtR to Identify DM and HTA
The optimal cutoff points for WHtR to identify DM in the Lao population (compared with those who have high HbA1c) is 0.5 (exact value = 0.497006). The AUC was 0.6723 (95% CI [0.64, 0.69]), indicating moderate discriminative ability.
The optimal cutoff point for WHtR to screen for HTA is also = 0.5 (exact value = 0.505992); the AUC of 0.6459 (95% CI [0.64, 0.69]) indicates fair discriminative ability.
Optimal Cutoff Points for BMI to Identify DM by HbA1c and HTA
The optimal BMI cutoff point for screening for DM in the Lao population, compared with patients having high HbA1c, is BMI >23.6 (exact value = 23.61164) with the AUC = 0.6573 (95% CI [0.63, 0.69]).
The optimal BMI cutoff point for screening for HTA in the Lao population is also BMI > 23.6 (exact value = 23.58833), with an AUC = 0.6307 (95% CI [0.61, 0.66]).
Discussion
This study identified WHtR as the best anthropometric index with predictive power for DM and HTA in the Lao population. It is recommended for health workers to assess risks in the population and among patients, who are often unaware of their disease status.1,3
In Lao PDR, nutrition research and policy are inconsistent in the use of BMI as the obesity index. Some studies and national nutrition training guidelines use an international standard BMI (Caucasian), 14 whereas others use an Asian BMI cutoff point. 1 The standard BMI cutoff point recommended by WHO might give unrealistic nutritional status results, increasing the normal range and reducing overweight and obesity, compared with results using the Asian BMI cutoff. This was confirmed in our results and others from Asian countries such as Thailand 6 and China. 8 The optimal cutoff point used in Asian countries should be lower compared with the Caucasian BMI (BMI between 23 and 25) considered as a health risk, which corresponds to the Asia-Pacific cutoff point recommended by WHO. Therefore, we recommend using the Asia-Pacific cutoff point to identify the risk of NCDs in countries in this region which have not established their own BMI cutoff point. For Lao PDR, when BMI will be used, the cutoff point of BMI > 23.6 is considered to indicate high risk when screening for NCDs. Using the Caucasian cutoff resulted in missing too many people; patients with DM and/or HTA were classed as overweight or obese by Asian measures, but fell in the normal range using the international standard. We also found that the BMI of the healthy population was slightly higher compared with the Asian cutoff point, possibly because of differences in age, sex, and ethnic group. Other anthropometric indices used to identify DM, HTA, or both also resulted as high risk with the Asian cutoff point but normal with the Caucasian cutoff.
Although widely used to assess health, BMI has been criticized as a poor predictor of heart disease, DM and certain cancers, because it does not consider the distribution of body fat, muscle mass, and metabolic health.18,19 A person with a high BMI may have a lot of muscle mass and a low body fat, and may not be at risk for NCDs. Conversely, an individual with a “normal” BMI may have a high percentage or unhealthy distribution of body fat, which could increase their risk of NCDs. Studies reveal that BMI can differ significantly among different age, sexes, and ethnic groups 18 based on the regions and demographics. Some ethnic groups are found to have a higher percentage of body fat and abdominal adipose tissue than Caucasians with the same BMI. 19 Therefore, using specifically identified BMI cutoff was recommended. 20
The highest performing anthropometric index to identify DM and HTA in our population was WHtR, with an optimal cutoff point of 0.5 to identify DM and HTA. The next best was WC, followed by WHR then BMI. Evidence from other countries has also suggested that WHtR was better than other anthropometric indices at identifying NCD risk factors.8,9,21 Yet, BMI and WC 10 are still the most commonly used worldwide, also in Lao PDR. 1 Measuring BMI also requires a weighing scale and a measuring board, which may be costly or unavailable, and challenging to transport to remote areas. Budgetary and other limitations restrict the placement of these tools in Lao health centers. 22 Evidence from this and other studies is that optimal BMI cutoffs vary between sex and ethnic groups, which was not a problem with WHtR.18,19
The WC and WHtR have been proposed as alternative tools to measure abdominal adiposity and may be superior to BMI in terms of their performance in predicting NCD risk, 7 as central obesity has been linked to a sedentary lifestyle, poor dietary choices, and stress. These behaviors can contribute to the accumulation of excess fat around the waistline, leading to central obesity and increased risk of NCDs. Central obesity may be a stronger predictor of mortality than other obesity indexes 23 and measuring it is cost-effective, requiring less investment. 21 The WC is suitable for screening NCDs in a large population and in remote areas. However, the international standard cutoff points for BMI and WC are not recommended; any anthropometric measure is associated with ethnic- and population-specific disease risks. 7
The WHtR has been reported to be a more accurate predictor of cardiovascular risk in comparison with WC and other indices,10,21,24 specifically in populations with a higher risk of metabolic disorders and type 2 DM, as often found in urban areas. Our study also found that WHtR is an effective predictor of high HbA1C levels in young patients with DM (18-34 years old). This makes WHtR a valuable screening tool for NCDs. Early identification can reduce complications and treatment costs, which are significant economic burdens due to the chronic nature of these diseases and long-term need for supportive medications as the primary intervention.
The WHtR considers the height, which may provide a more precise reflection of overall body size and fat distribution than WC alone. Adult height is considered to be relatively stable over time, little influenced by nutrition or health. 25 It can also be a predictor for NCDs, with taller people being at increased risk of certain types of cancer 26 and shorter people at increased risk of cardiovascular disease and type 2 DM.27,28
We found that the average WHtR in our study and the optimal cutoff, WHtR = 0.5 (0.497006), were in line with those suggested by WHO and various studies as globally applicable in screening for cardiovascular and metabolic risk7-9 with the ability to screen other health indicators and clinical markers such as the albumin excretion rate and coronary artery disease.29,30 We did not find any significant difference between the majority and minority ethnic groups in Lao PDR, which is consistent with results of a meta-analysis, that WHtR was strongly associated with DM for both Asian and non-Asian populations. It can also provide a clear call-to-action message, like “A healthy waist is less than half your height, so get moving and eat right.” Such a message is simple and can be used universally, also in an NCDs prevention campaign where obesity and NCDs are on the rise, as in Lao PDR.
The technique that we used to obtain WC in this study was to measure parallel to the floor, at the level of the umbilicus, rather than at the narrowest point between the lower costal border and the top of the iliac crest, as recommended by the WHO. 7 There is evidence that measuring the WC at the umbilicus 23 provides higher performance in detecting body fat, especially in women, leading to a recommendation to standardize the measurement location; it proved easy to find the place for measurement in practice. We also found that WHtR was effective in predicting health outcomes regardless of sex; however, its performance was slightly higher in women for HTA and in males for DM. Further studies are recommended to confirm whether measurement of WC at the umbilicus provides higher sensitivity in the Lao population than measuring at the iliac crest, as recommended by WHO.
In the literature, it is not clear whether WHtR is more effective in predictive performance in males or females; the reported results do not reach a consensus. The slight difference in sensitivity that we found may depend on factors such as age and health. However, a systematic review and meta-analysis found that the predictive ability of WHtR did not differ significantly between men and women, suggesting that WHtR may be equally effective in both sexes.10,11
Limitations
This was a cross-sectional study with biological examination at one time point. It did not account for other factors related to increasing obesity or possible risk behaviors related to DM and HTA. The optimal cutoff point was determined by optimizing both sensitivity and specificity to compare the performance of different anthropometric indices. In clinical settings, such as assessing risk for NCDs, the cutoff point could be adjusted to increase the sensitivity of the screening test, thereby enhancing the ability to identify potentially important health outcomes.
Recommendations
Waist-to-height ratio is a simple, cost-effective, affordable, portable, and effective way to measure central obesity and is a better predictor of DM, HTA, cardiovascular disease, and other NCDs risk, than BMI. Our results are supported by reports in the literature that recommend using the WHtR as indicator for health promotion and prevention campaigns. The WHtR can also be used as first-stage screening tool for NCDs. The cutoff point of 0.5 was easy to remember and can be included in health promotion slogans, which should be created in cooperation with community members and patients to ensure relevance. The WHtR can also be useful as a target message for NCD patients to monitor their waistline along with regular treatment and changing lifestyles, particularly in urban areas with their ongoing food and lifestyle transition but where people also start to pay more attention to their own health. The index can be used together with standard health examinations during health checks or physical examinations to monitor risk and start to reduce morbidity and mortality. We do recommend using WHtR as a screening tool and in public awareness campaigns for DM and, HTA, in both urban and rural remote areas or in fieldwork under unfavorable conditions.
Conclusion
The research agenda for nutrition, prepared with participation by actors at all levels, led to this research, the results of which in turn will inform planning of health promotion activities, which should also be planned in a participatory way. The WHtR could serve as screening indices for NCDs prevention and control, and can be used in urban areas, with a high prevalence of DM and HTA, and in rural areas, in fieldwork under difficult conditions. We can use the WHtR for health prevention and promotion in urban areas along with appropriate advice about changing lifestyle factors. The WHtR can work both as a public health and a clinical screening tool for monitoring the DM and HTA in Lao PDR, using the optimal cutoff point of 0.5 for both DM and HTA in both sexes and all ethnicities.
Supplemental Material
sj-docx-1-aph-10.1177_10105395241295573 – Supplemental material for Waist-to-Height Ratio as a Key Predictor for Diabetes and Hypertension in Lao PDR National Health Survey
Supplemental material, sj-docx-1-aph-10.1177_10105395241295573 for Waist-to-Height Ratio as a Key Predictor for Diabetes and Hypertension in Lao PDR National Health Survey by Kethmany Ratsavong, D. R. Essink, Manithong Vonglokham, Sengchanh Kounnavong, Somphou Sayasone, Wichai Aekplakorn, Suchin Worawichawong and E. P. Wright in Asia Pacific Journal of Public Health
Footnotes
Acknowledgements
We express our gratitude to the Lao Tropical and Public Health Institute, its collaborators and benefactors who conducted the extensive study that served as the source of our data. We extend our sincere appreciation and special acknowledgment to Ramathibodi University for support in data processing and analysis and technical support. We also acknowledge the valuable assistance of Dr. Latsamy Siengsounthone, Ammarin Thakkinstian and Dr. Anousin Homsana, who provided technical expertise in data management, statistics and advised on data analysis and findings.
Author Contributions
MV was the supervisor supporting the project, managed data collection and coordinated work related to the data; SK provided technical support on the data management and manuscript writing; KR asked the research question, contributed to data analysis, then drafted and revised the article; DE, SS, and EPW supervised data analysis and interpretation, and writing and revising the manuscript. All authors were involved in conception and design and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
To maintain confidentiality, the names of respondents were not included in all questions, and information collected from respondents was kept confidential. The research objectives, methodology usefulness, and potential risks were explained to each respondent before the interview. Informed consent was obtained from all participants.
The protocol of the STEPS survey was reviewed and approved by the Lao National Ethical Committee for Health Research, which gave clearance following regulations in force (Deliberation No. 018/NECHR 03 March 2020). This research was authorized by the General Directorate of Lao Tropical and Public Health Institute.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.