
Abstract

Introduction
Hand, foot, and mouth disease (HFMD) infection is mainly due to enterovirus 71 (EV-A71) and coxsackievirus A16 (CVA16). 1 Hand, foot, and mouth disease is usually a mild disease and characterized by fever and a blistering rash, mostly on the hands, feet, and oral cavity but at times can have severe clinical manifestations such as meningitis, encephalitis, and myocarditis especially in children. The incubation period of disease is three to seven days. The transmission is through direct contact with mucus, saliva, fluid from blisters, or feces of an infected patient and indirectly by fomites.
India reported the first outbreak of HFMD from Kerala in 2003. 2 During 2004 to 2006, significant morbidity and mortality were reported in children with EV-A71 infection from Uttar Pradesh (UP) during 2004 to 2006. 3 In 2007, an epidemic of HFMD was reported in children with mild symptoms from West Bengal. 4 Herein, we report the epidemiological and molecular characterization of four cases of HFMD reported from central India (Jhansi, UP), wherein no case was reported earlier (outbreak).
Methods
An epidemic investigation was carried out by a team, comprising of medical officer, public health specialist, pediatrician, and epidemiologist. An active surveillance for cases of fever among children up to 15 years of age was done in the community. All doctors in the local area were requested to report any case of fever with rash to the epidemic investigation team. The active surveillance was conducted till 15 days after the last case.
Clinical specimens including oropharyngeal swab (OPS), nasopharyngeal swab (NPS), ethylenediaminetetraacetic acid (EDTA) blood, serum, and lesion crust/scabs of the four suspected cases were referred to Indian Council of Medical Research (ICMR)-National Institute of Virology, Pune, India. These were tested using Pan-Enterovirus–specific real-time polymerase chain reaction (PCR). Nested reverse transcription polymerase chain reaction (RT-PCR) for genotyping of the cases was further carried out using the Sanger sequencing method as well as next-generation sequencing approach. The ethical clearance for the study was provided by Institute Ethics committee vides their letter no. IEC/2022/121 dated on May 29, 2022.
Results
Four cases investigated during this study were in age group two to five years (two males and two females) (Table 1). The first two cases were reported to Medical Inspection (MI) room on May 25, 2022 (May is summer season and is usually very hot) with travel history in same train to Vishakhapatnam (May 21-22, 2022/1100 hour) to Jhansi which is the nearest railway station from Babina. Contact history of these cases with children less than 10 years old having similar illness at hometown on during their stay (May 17-19, 2022) for family get together was also noted. The remaining two cases reported on May 29, 2022 were epidemiologically linked with the first two reported cases.
Clinical Presentation of Hand, Foot, and Mouth Disease (n = 4).
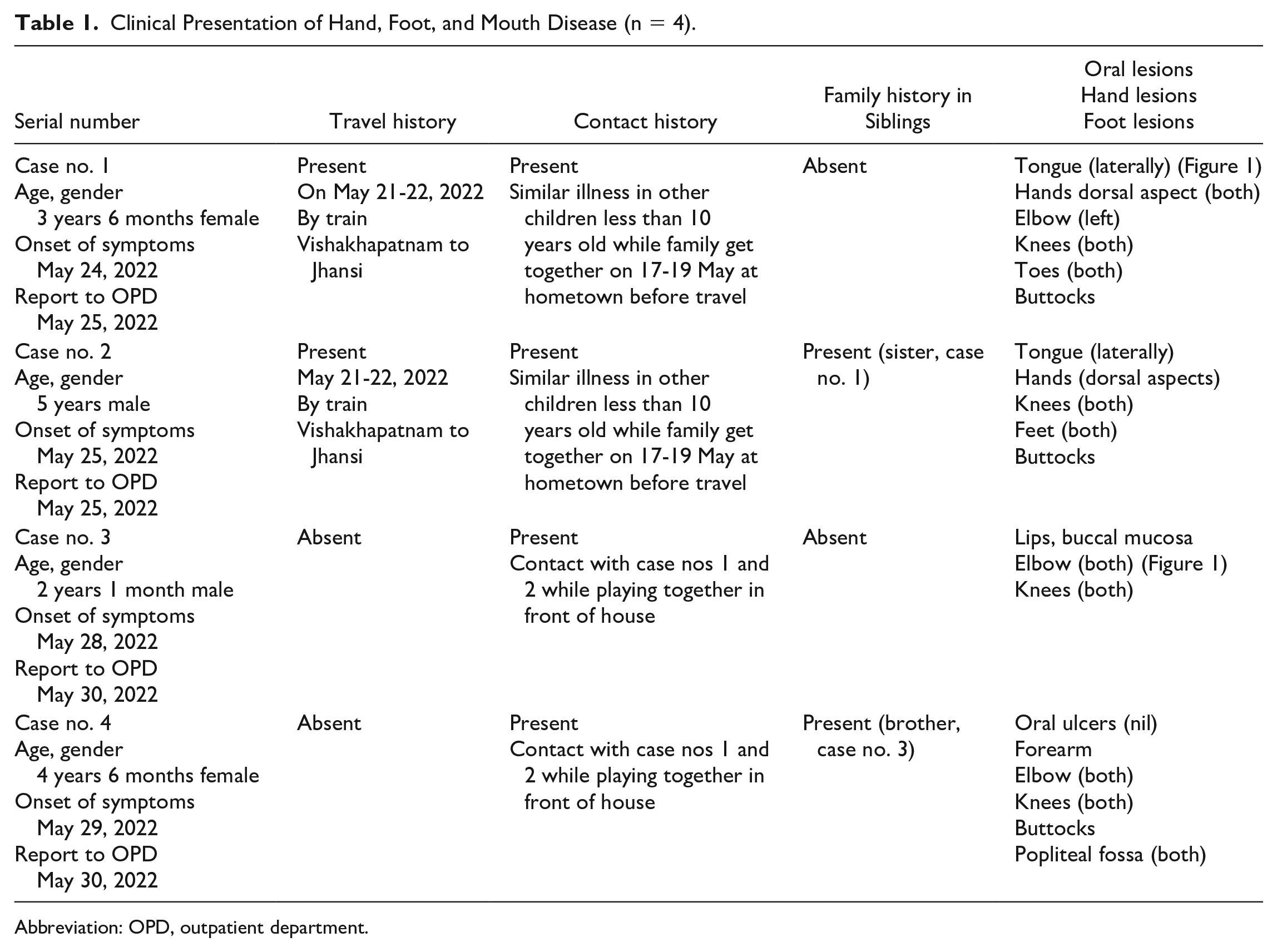
Abbreviation: OPD, outpatient department.
The cases presented with a mild prodrome of one to two days, followed by the appearance of oral lesions. Apthous-like ulcers were present on tongue, lips, and buccal mucosa and led to feeding difficulty. Skin lesions appear one to two days later and were seen as oval or circular vesicles on erythematous bases. In all these cases, the diagnosis was made on clinical grounds (Figure 1). All four cases had mild illness and resolved without any sequel. The patients were treated symptomatically.

Lesion images of the 4 HFMD cases. (a) Tongue ulcer. (b) Rashes over hand. (c) Rashes over knee. (d) Healing lesions over hands.
Out of 24 specimens of these suspected four cases, three specimens (oral swab and crust/scab of the lesions) showed presence of EV RNA (CVA16) by RT-PCR of real-time PCR positive samples were further processed for genotyping. For positive samples, PCR amplification and sequencing targeting a part of VP1 region was done. Partial VP1 viral capsid gene region could be amplified and sequenced from two cases using primers AN88 and AN89. The sequence identity of EV strains was determined through the BLAST search tool (http://www.ncbi.nlm.nih.gov/blast). The next-generation sequencing could not yield the reads for the EV which might be due to the low viral loads in the clinical specimens.
The preventive measures were instituted to prevent spread of cases and included strict home isolation, sensitization of parents, and community. Active surveillance was done for around 100 houses by health staff every third day to find out children with similar illness. The school authority was informed to screen the children and report any case of fever to the authorities. However, no further cases were reported from school or the community.
Discussion
In this study, the cases were clinically suspected and were confirmed by molecular methods. Sequence analysis revealed the presence of CVA16 in three cases in our study. Hand, foot, and mouth disease is commonly caused by CVA16 and EV-A71 but is also reported with coxsackievirus A5, A7, A9, A10, B2, B3, and B5. Hand, foot, and mouth disease caused by CVA16 is usually a mild disease and patient recovers in five to seven days without any complications. The cases followed in this study also recovered without any sequelae.
The geographic distribution of cases in India showed that they have been reported from nearly all states of India. The increase in reporting of cases of HFMD from India may be due to increase in awareness and improvement in molecular diagnostics. Moreover, in today’s era, it is very easy for organisms to be transferred from one part to another part of our country, spreading the disease, and this is applicable to army personnel and families who are regularly travel by road/train/air due to leave, postings, and temporary duties.
Conclusion
It is important for health care workers like dermatologists, pediatrician, general dentist as well as physician to be aware of this disease as they may be the first health care professional to be consulted in such cases. Also, day care and nursery teachers, Accredited Social Health Activist (ASHA) workers, Anganwadi workers, and multipurpose workers working on ground must be aware of this disease and timely isolation and reporting of such cases to nearest health facility. Many authors have proposed the development of multivalent vaccines for the control of HFMD. 5 It is proposed that improved hand-washing and related hygienic improvement be incorporated in the community, nursery schools, and kindergartens. The surveillance of HFMD must be maintained as there is no effective chemoprophylaxis or vaccine available as of today.
Footnotes
Acknowledgements
The author wishes to thank Major Anil (Pediatrician) for immediate notification; health superintendent Mr Abhilash and health inspector Mr Asif for ground work and photography, health awareness in surrounding parents, IEC Material distribution; laboratory assistant Naik Nagaraju for lab investigations and packaging material; and Team NIV, Pune, for virological identification.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.