
Abstract

Introduction
Diabetes in older adults is a leading global population health problem and trending upward in China and elsewhere around the world. 1 However, substantial urban-rural disparities exist in diabetes management and care. 2
Metformin has been the most widely prescribed initial glucose-lowering medication for diabetes management, and metformin-related adverse drug reactions (ADRs) are also commonly reported including various gastrointestinal complaints (such as diarrhea, nausea, vomiting, and abdominal pain). 3 Previous studies have reported a higher burden of metformin-related ADRs in urban residents than their rural counterparts 4 but did not characterize variation of such disparity in duration of metformin use, and concomitant medication use, as well as the potential changes over time. In this study, we aimed to extend our knowledge by describing rural-urban disparities in relation to different patient characteristics, exploring such disparities in the occurrence of metformin-related ADRs, and evaluating the trends in ADR occurrences during a 10-year period.
Methods
Data Source
Based on the ethics approval and data use agreement with Jiangsu Center for ADR Monitoring [JSADR#2021/0101], we obtained the information of “certain,” “probable,” and “possible” metformin-related ADRs in adults older than 45 years from 1 July 2010 to 30 June 2020 from the spontaneous reporting system (SRS) in Jiangsu Province. 5
Definitions
We used the location of reporting hospitals as the best available proxy to categorize the geographic area where a patient was attached to as being urban or rural. Seriousness of metformin-related ADRs as serious or non-serious. Time to onset was calculated as the time between the reported first date of metformin treatment to the first date of ADR occurrence. Outcomes of ADRs were categorized as recovered, improved but not fully recovered, or unable to trace. We categorized age group as 45 to 64 years, or 65+ years; sex as male or female; concomitant medication use as yes or no; duration of metformin use as 0 to 1, 2 to 7, 8 to 30, or 31+ days; and reporting hospitals as Tier 1: primary, Tier 2: secondary, or Tier 3: tertiary institution.
Statistical Analysis
We calculated the crude incidence rates of using the population estimates by calendar year as the denominator. We used the Joinpoint Regression to estimate the annual percent change in age-standardized incidence rates of metformin-related ADRs. 6 We calculated the age-, sex-, and year-adjusted incidence rate ratios (RRs) and corresponding 95% confidence interval (CI) to explore rural-urban disparities using the negative binomial regression model with an annual population offset.
Results
During the 10-year study period, a total of 3786 metformin-related ADR incidents were identified in diabetic patients aged 45 years and older. Of these cases, approximate 85.0% (n = 3218) were attached to urban areas (Table 1).
Number (%) and Adjusted Rate Ratio (RR) a for Metformin-Related ADRs Crude Incidence Rate (per 100,000) Among Adults in Rural and Urban Areas According to Population Characteristics in Jiangsu Province of China, July 2010 to June 2020.

Rate ratio (RR) was calculated using metformin-related ADRs incidence rate of the urban population as the referent after adjusting for age, sex, and year.
Calculation was not carried out for small number (<5) in relational cells.
Significant metformin-related ADRs incidence rate ratios are in bold.
The incidence of metformin-related ADRs among older adults increased by 16.9% per annum (95% CI: 7.6-27.0%) during 2010-2018 and then remained little change (Figure 1). While metformin-related ADRs demonstrated a similar pattern in urban areas, that in rural areas appeared an annual marginal increase by 6.5% (−1.8% to 15.5%), although not statistically significant (Figure 1).
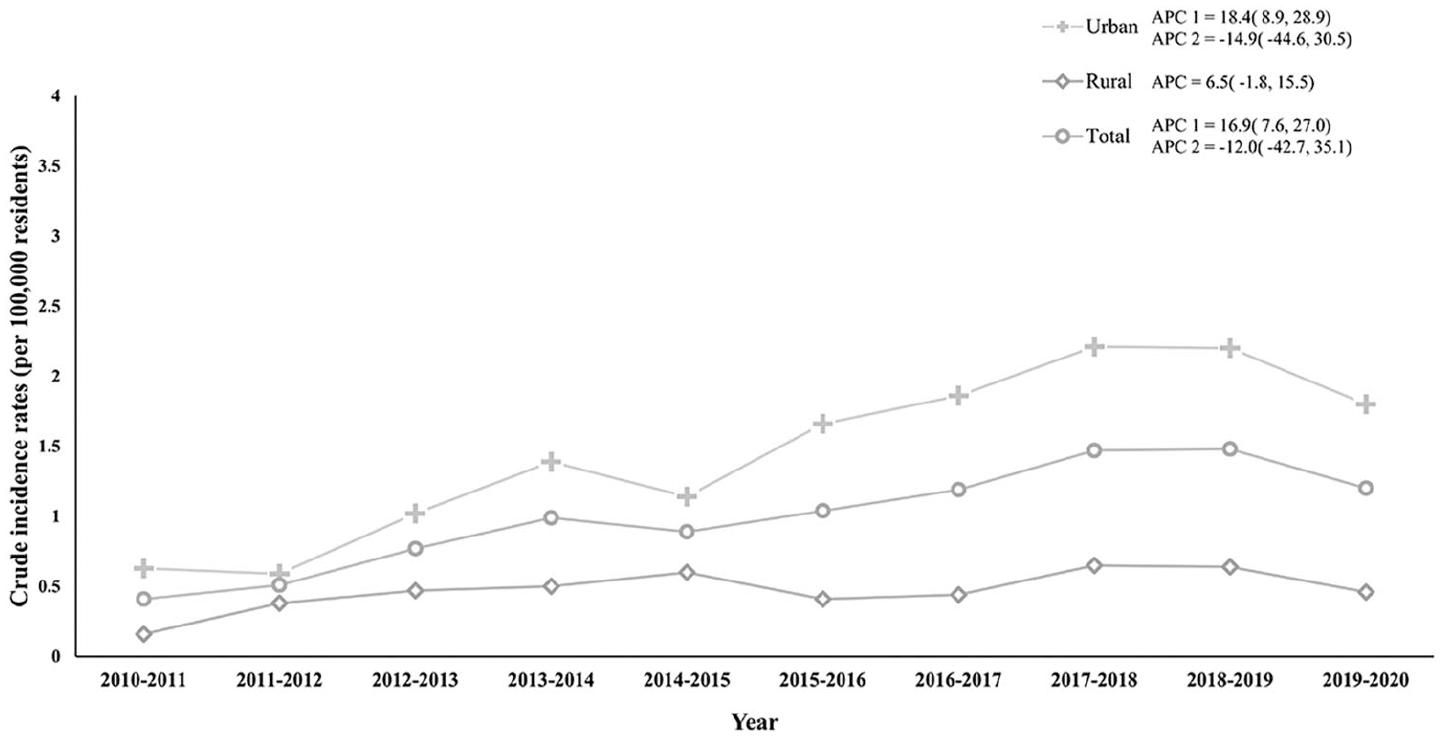
Trends and annual percentage change in incidence rate of metformin-related adverse drug reactions by rurality of residence in Jiangsu province of China from July 2010 to June 2020.
A significantly lower incident rate of metformin-related ADRs was observed in rural patients compared with their urban counterparts (RR: 0.31, 95% CI: 0.28-0.34) (Table 1). However, this rural-urban gap was slightly widened in patients aged 65+ years (0.26; 0.23-0.31), with concomitant medication use (0.27; 0.21-0.33), or presented at secondary health care institutions (0.04; 0.02-0.07), comparing with that in a younger patient group (0.34; 0.30-0.38), without concomitant medication use (0.32; 0.29-0.36), or those presented at primary institutions (0.54; 0.48-0.60), respectively. In addition, such rural-urban difference was more evident in for incident use (<7 days) of metformin than regular use (>30 days) in terms of duration of use (Table 1).
Discussion
In this secondary data analysis, the incidence rate of metformin-related ADRs serious enough for hospital care in older adults aged 45 years and above in Jiangsu province of China has increased over time during the first 8 years, and then remained little change. While the entire provincial areas have experienced this overall rising problem, metformin-related ADRs were more common in urban communities than their rural counterparts, which was consistent with previous findings. 4 We also observed that rural-urban disparities varied by patient characteristics including age group, duration of metformin use, and concomitant medication use, highlighting the world wide challenge brought by the urgency of optimal management of diabetes.7,8
In contrast with such forecast that burden of diabetes in rural areas would outpace that in urban areas, we observed more ADR burden to the urban areas rather than rural areas in Jiangsu. We speculated that such disparities might be related to the substantially lower rate of metformin use in rural patients, 9 as evidenced by the current finding that the rural-urban disparity was more apparent in those who used metformin for less than 1 day (<24 hours), perhaps newly diagnosed patients, as well as the previous finding that secondary oral medications such as sulfonylureas were prescribed more frequently than metformin in rural areas of China. 10 We also speculated that the observed urban-rural disparity might reflect a lower willingness to report to and communicate with physicians on their experience of metformin therapies among rural patients in comparison with their urban counterparts.
This study has several limitations. First, rurality was measured by the location of ADR reporting institutions, which might not correspond to the actual area of residence. Second, the current secondary data analysis may result in an underestimation of metformin-related ADR burden due in part to possible underreporting. Third, we cannot identify patients’ level detailed risk factors and determine their contribution toward the observed rural-urban disparities in metformin-related ADRs. In addition to residue confounding due to broad age interval for grouping, data derived from the SRS were a conventionally primary source for investigation on postmarketing drug safety; however, information about time to onset relied on voluntary reporting, which may introduce recall bias. Therefore, results should be interpreted with care.
Conclusion
The rising burden of metformin-related ADRs in rural and urban communities highlighted the need to develop and implement medication safety countermeasures in China.
Footnotes
Contributions of Authors statement
WD, BY, and JZ conceptualized and designed the study. HX and ML conducted the data analysis, and wrote the first draft of this manuscript. All authors contributed to the critical review, interpreted study data, and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Department of Education (grant no. 1125000172, 5725002302), the Natural Science Foundation of China (grant no. 82173899), the National Social Science Foundation of China (grant no. 23CGL072), the Fundamental Research Funds for the Central Universities (grant no. 3225002002A1), the Key Research and Development Program of Jiangsu (grant no. BE2021736), and Jiangsu Provincial Department of Science and Technology.
Ethical Approval
Our study was based on the ethical review and data use agreement with Jiangsu Center for ADR Monitoring (JSADR#2021/0101).
Consent to Participate
Informed consent was not required for this study due to its analytic nature of anonymous and aggregated data.
Consent for Publication
Not applicable.
Availability of Data and Material
The datasets generated during the current study are not publicly available. Aggregated data may be available from the corresponding author upon reasonable request.