
Abstract

Introduction
The national government of the Federated States of Micronesia (FSM) has targeted 1 a 5% reduction in tobacco smoking prevalence by 2024 (adult baseline: 30.8%, and youth: 27.3% in 2014). 1 The WHO Framework Convention on Tobacco Control (FCTC), ratified by FSM in 2005, facilitates the reduction of tobacco use through the implementation of evidence-based policies, such as the ban of tobacco advertising, promotion, and sponsorship (TAPS; Article 13). The national report (2020) 2 to the WHO FCTC Secretariat on domestic TAPS policies does not provide a qualitative assessment of the legislative context, the existing loopholes, or how the local policy environment affects implementation and enforcement. This qualitative health policy analysis aims to fill in these gaps.
Methods
We employed the health policy triangle model 3 on 308 documents collected from publicly available resources (see online Supplementary Appendix 1). We excluded 269 irrelevant documents or with repeat information. We collected the data between November and December 2020 (except the Global Youth Tobacco Survey, 2019, 4 collected in 2022). The thematic framework approach 5 informed the study analysis of 39 documents (see framework index in data availability statement).
Results
Adoption of TAPS Provisions due to International Commitments
All TAPS-related provisions were adopted and implemented in FSM due to commitments developed with international organizations. For example, following the Regional WHO recommendations for TAPS bans, several TAPS provisions were introduced during the 1993-1994 period (see Supplementary Appendix 2).
Five years after the WHO FCTC ratification, specifically, between 2010 and 2012, misleading descriptors on tobacco packaging were banned nationally, Chuuk State banned tobacco industry sponsorship and introduced fines for any violations, while Pohnpei State prohibited tobacco advertising and promotion, exempting advertising that either originated outside the state or was due to incidental media placement.
The WHO FCTC Secretariat’s assessment (2012) 6 identified policy gaps and areas requiring further action (see Table 1). These recommendations facilitated the FSM Congress to create the Tobacco Control Act of 2016. The same year, Pohnpei also banned tobacco product displays at retail outlets.
TAPS-Related Policy Gaps and Recommendations as Drawn by the WHO FCTC Secretariat’s Tobacco Control Policy Assessment in 2012, in Comparison With the Adopted National “Tobacco Control Act of 2016” (CB 19-132).
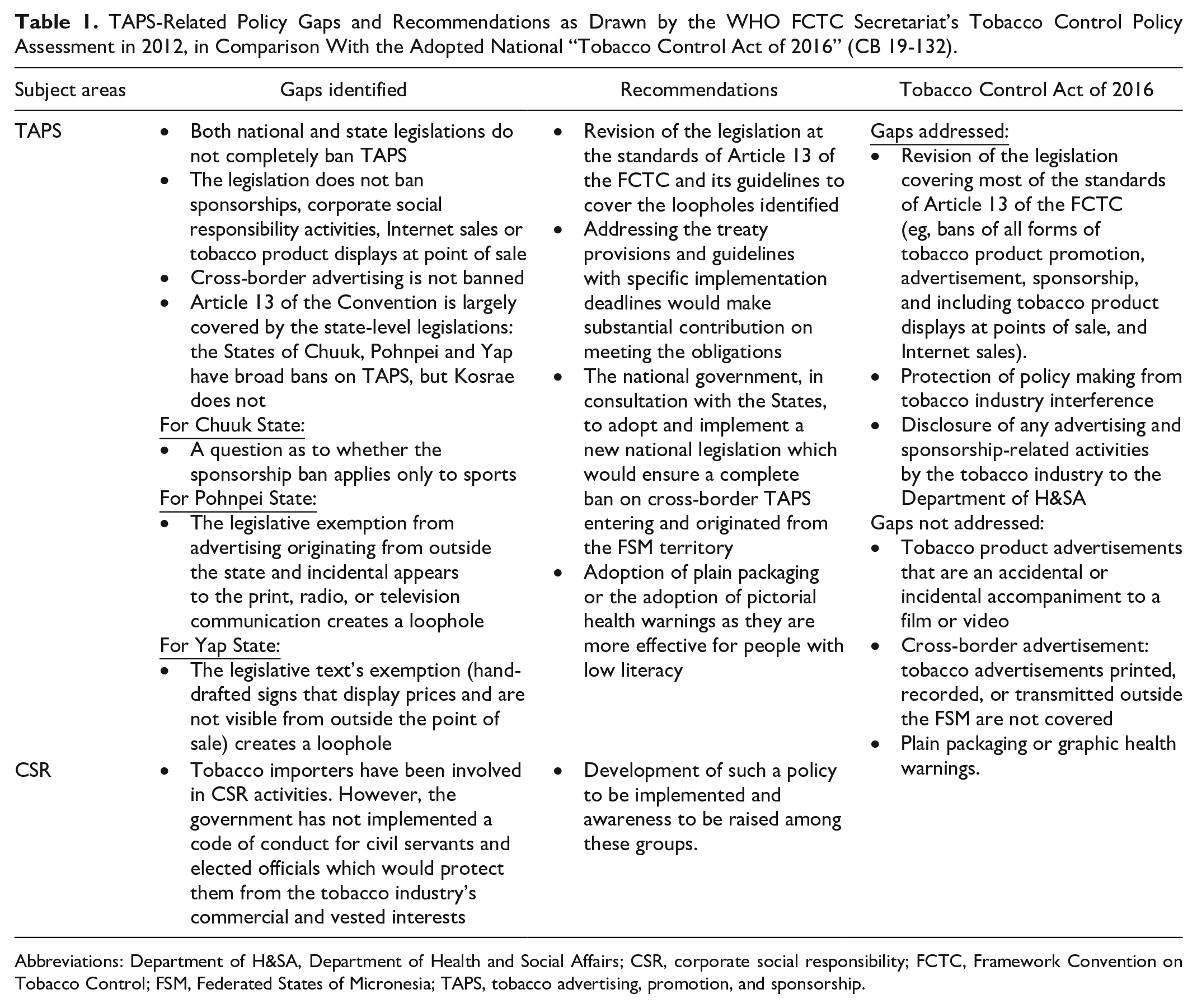
Abbreviations: Department of H&SA, Department of Health and Social Affairs; CSR, corporate social responsibility; FCTC, Framework Convention on Tobacco Control; FSM, Federated States of Micronesia; TAPS, tobacco advertising, promotion, and sponsorship.
Limited Involvement of Sub-National Actors
At the national level, the WHO country office assisted FSM to develop Non-Communicable Diseases (NCD) national strategies 1 with TAPS-related content, and the WHO FCTC Secretariat, via its policy assessment team, 6 prompted the formulation of national and state legislation.
At the sub-national level, there are community health coalitions; however, their involvement is limited. We identified only one example of engagement. Specifically in 2012, the health coalition of Kosrae met with pastors, women leaders, mayors, council members, and youth representatives; discussed Article 13; and jointly developed an advocacy plan for the adoption of a comprehensive TAPS ban. At the time of writing, a policy has not been adopted.
Problematic Tobacco Control Program Funding and Administration
Tobacco control program funding and administrative issues highlight the constrained role of the community health coalitions. The FSM receives an annual grant from the United States, a porting of which fund the FSM Tobacco Control Program. The funds from the national level, where fewer tobacco control activities are conducted, are not decentralized to the States, hence the fund award has limited reach to the tobacco community activities.
Incomplete Documentation of TAPS
The tobacco industry’s marketing practices are not systematically documented, and the documentation of the FSM population exposure to TAPS is limited. The most recent Global Youth Survey (2019) 4 indicates that FSM adolescents are exposed to TAPS at points of sale (44.3%) or on television, videos, or movies (76%), by being offered a free tobacco product (17.6%) or owning an item bearing a tobacco brand logo (21.3%).
Discussion
The Tobacco Control Act of 2016 is significantly more comprehensive than the preceding acts; however, loopholes still exist. For example, the Act allows any advertising material created abroad to enter the country. It also requires the tobacco industry to declare all its marketing activities to the Department of Health and Social Affairs, which should make this information publicly available. At the time of writing, the Department has not published any related information. Last, the Act mentions the establishment of a “Tobacco Control Inspector” to monitor compliance; however, it does not detail its role nor how inspections could be achieved in isolated island locations.
The regional networks, which FSM belongs to, limit their involvement to tobacco taxation and the restriction of the tobacco industry interference. Neglecting TAPS-related initiatives limits the opportunities for best practice exchanges within the region. Other archipelagic countries, such as Indonesia, are participating in Mayor Alliance Schemes 7 which empower municipal leaders for tobacco control reforms. Transferring such activities to the FSM setting could initiate a horizontal diffusion of TAPS policy implementation among the islands. This would enhance FSM’s objective of tobacco control activities consistently reaching all citizens in every island. 8
The present study is limited to data that were publicly available, and it includes a relatively small amount of available information about TAPS in the FSM. The inclusion of primary data (e.g., interviews of stakeholders) and an intensification of the domestic tobacco control advocacy efforts on TAPS could provide additional information for future studies.
Conclusion
Small island nations’ unique context offers opportunities for creative enforcement. Tapping into community networks and expanding enforcement authority to encompass volunteers can expand the reach of compliance monitoring. The inclusion of traditional or faith-based leaders, and church communities can yield promising results. 9 Finally, capacity building for advocacy, data collection, and surveillance is essential to track progress in all tobacco control areas, and community-based programs can assist to augment tracking of WHO FCTC compliance. 10
Supplemental Material
sj-docx-1-aph-10.1177_10105395221134554 – Supplemental material for Tobacco Control Legislation in Small Island Nations: Adoption of WHO FCTC Article 13 in the Federated States of Micronesia
Supplemental material, sj-docx-1-aph-10.1177_10105395221134554 for Tobacco Control Legislation in Small Island Nations: Adoption of WHO FCTC Article 13 in the Federated States of Micronesia by Arsenios Tselengidis, Sally Adams, Becky Freeman, Annette Mascunana David, Sarah Dance and Jo Cranwell in Asia Pacific Journal of Public Health
Supplemental Material
sj-docx-2-aph-10.1177_10105395221134554 – Supplemental material for Tobacco Control Legislation in Small Island Nations: Adoption of WHO FCTC Article 13 in the Federated States of Micronesia
Supplemental material, sj-docx-2-aph-10.1177_10105395221134554 for Tobacco Control Legislation in Small Island Nations: Adoption of WHO FCTC Article 13 in the Federated States of Micronesia by Arsenios Tselengidis, Sally Adams, Becky Freeman, Annette Mascunana David, Sarah Dance and Jo Cranwell in Asia Pacific Journal of Public Health
Footnotes
Acknowledgements
We would like to thank Dr Allen Gallagher for proofreading support and for providing comments on the paper. Any mistakes are entirely the authors’ own.
Author Contributions
All authors conceived the idea for the study. AT, BF, SA, and JC developed the research design. AT, collected and analyzed the data, produced the first draft. SD reviewed all coded data and the developed themes. AMD provided national and regional expertise in several manuscript versions. All authors edited the paper. All authors approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AT and SD acknowledge the support of Bloomberg Philanthropies Stopping Tobacco Organizations and Products project funding (![]() ). The funders played no role in the study design, analysis and interpretation of data, or writing of the report or the decision to submit the article for publication.
). The funders played no role in the study design, analysis and interpretation of data, or writing of the report or the decision to submit the article for publication.
Supplemental Material
Supplemental material for this article is available online.
Data Availability
Data are available in a public, open access repository. The reference for this dataset is: Tselengidis, A., Adams, S., Freeman, B., David, A., Dance, S., Cranwell, J., in press. Framework Index for Tobacco Control Legislation in Small Island Nations: Adoption of WHO FCTC Article 13 in the Federated States of Micronesia. Bath: University of Bath Research Data Archive. ![]() .
.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.