
Abstract
The achievement of Universal Health Coverage, including quality services, is high on the international agenda. Cambodia aims to expand social health protection and is committed to improving the healthcare service quality. We review the country context and propose five policy approaches to accelerate progress on healthcare quality improvement in Cambodia. These approaches aim to augment the profile and continued focus on quality while leveraging and optimizing existing systems to incentivize improvements and increase value for money.
Keywords
What We Already Know
Healthcare quality is a core element of Universal Health Coverage; it is key to building public confidence and an efficient, effective healthcare system.
Quality improvement is a complex process which can be enhanced through various policy levers.
What This Article Adds
This article provides a summary of some of Cambodia’s systems that can be leveraged to improve healthcare quality.
This article suggests five policy approaches to accelerate progress on healthcare quality improvement in Cambodia.
Introduction
Sustainable Development Goal (SDG) 3 calls for the achievement of “universal health coverage, including financial risk protection, access to quality essential health care services, and access to safe, effective, quality and affordable essential medicines, and vaccines for all.” The importance of improving quality as a core component of Universal Health Coverage is affirmed by The Lancet Global Health Commission on High Quality Health Systems in the SDGs Era. 1 Population coverage of social health protection in Cambodia is currently 30% with nearly 54% of Cambodians having no potential coverage mechanism. 2 The country is working toward expanding coverage; however, health service quality remains a significant challenge. 3 Quality of care has been identified as one of the pressing imperatives in health system strengthening. 4 Improvements in health care delivery require a deliberate focus on quality of health services. 5 This necessitates strong governance and leadership, particularly for the development of quality management infrastructure. 6 Moreover, external pressures and incentives can stimulate performance improvement and quality. 7
National Context
Cambodia’s population in 2020 is projected at 16.5 million with about 9.8% of the population under 5 years of age. 8 Since 2000, the country has significantly improved several key health measures, including achieving high coverage of maternal and child health services. 9 The infant mortality rate in 2019 was 22.8 deaths per 1000 live births. 10 Life expectancy is 67 years for males and 71 years for females. 11 However, a study comparing the Universal Health Coverage service coverage index among 52 countries found Cambodia to have one of the highest disparities between the national average and the poorest wealth quintile. 12
The Royal Government of Cambodia’s National Social Protection Policy Framework aims to “give more attention to improving the quality of health care services.” The recently established National Social Protection Council and its Executive Committee have an important oversight and coordination role to play in the implementation of the Framework. The Minister of Economy and Finance chairs the Council, which is constituted by 10 other Ministers including the Minister of Health and the Minister of Labor and Vocational Training. The same ministries also have high-level representation on the Council’s Executive Committee.
Concurrently, the Ministry of Economy and Finance is advancing its Public Financial Management Reform Program. Presently, the process is focusing on program-based budgeting and budget-policy linkages. The country’s National Health Strategic Plan (2016-2020) describes the strategic intent of the program-based budget: “to directly link policy to budget performance, ensuring that planned budget investments in health are well organized and wisely used in pursuit of achieving the stated policy outcome within mandates of the Ministry of Health and Budget Entities.” The process is expected to improve allocation and predictability of funding for the health sector and link allocated resources with outcomes of health service delivery. The Public Financial Management Strategy Framework also describes a shift in focus from input and output to outcome and results.
The Ministry of Health recently expanded its decentralized service quality monitoring system. The system is implemented by trained evaluators from the Provincial Health Departments and the Operational Districts. This system provides health service quality scores for all public health facilities (exempting national hospitals) on a quarterly basis. Quality scores are checked by a semi-independent certification agency. A composite score is calculated by weighting three indicators that align with the three dimensions of health care quality: structure (30%), process (60%), and outcome (10%). 13 Structure assesses management, financing, staff, infrastructure, and equipment using direct observation, record review, and checklists. Process assesses technical competency and interaction between patients and providers using vignettes. Outcome assesses patient perception of quality collected through patient interviews using a standardized tool. The approach has some limitations including potential bias among interviewed patients, particularly for those who are interviewed at the health facility. Another challenge is the difficulty with finding patients who have left the facility. The quality scores are used to (partially) adjust payments of quarterly Service Delivery Grants made to health facilities. These grants are intended to provide health facilities with an additional and flexible budget for meeting urgent and necessary operational expenditures to improve minimum conditions for delivering quality health services while incentivizing quality improvement. 14 This system provides an opportunity to advance strategic purchasing: the purposeful approach to purchasing health services to get more value for money spent which, in the context of efforts at quality improvement, means resources can be channeled to promote quality in health care.15-17 Regulatory mechanisms including the monitoring of care processes, and measurement of patient satisfaction and health outcomes are necessary for case-based payments to be effective. 18
Another important development for health services quality improvement in Cambodia is the drafting of the Law on Administration of Health Services. The law is being developed “to ensure and promote quality of health care services provided by health facilities to ensure health and safety of clients” (Article 1). The draft is presently under final review and will apply to all health care services provided by public and private health facilities at all levels (Article 3). Requirements and procedures for management of health care service quality assurance shall be determined by Sub-decree, and assessment tools shall be determined by legal directive (ie, Prakas) issued by the Minister of Health (Article 26). In addition, when promulgated, the law will officiate the establishment of a National Accreditation System (Chapter 6, Articles 33-43). The draft law also states that the accreditation organization will be an independent public institution. Once promulgated, the law will allow for the formulation of regulations to enable implementation of accreditation.
Quality Improvement Approaches
First, we suggest the adoption of a strategic purchasing approach whereby facility-level quality scores are applied to health service reimbursements made by government-operated social health insurance schemes (ie, the Health Equity Fund for the poor and the National Social Security Fund for civil servants and the private sector). These schemes pay (mostly public) health facilities established rates for services provided to eligible beneficiaries—collectively covering about 4.3 million people. 2 These case-based payments are intended to replace user fees charged to uninsured patients. Linking quality scores to reimbursements is expected to provide an additional financial incentive to providers to improve quality.
Second, we suggest optimizing the strategic purchasing approach by reforming the reimbursement system. More specifically, the reimbursement rates should be increased and aligned for the two insurance schemes. This will maximize the financial incentive while correcting a 2-tier system, where patients whose services are reimbursed at the higher rate are likely to be prioritized, an approach that undermines the equal provision of quality services.
Third, we suggest that quality monitoring scores as well as other key progress indicators related to the accreditation/licensing system (see Table 1) are integrated into the annual performance-based budgeting process. Annual targets should be mutually agreed upon between the Ministry of Economy and Finance and the Ministry of Health.
Illustrative Cambodia Health Care Accreditation System Establishment Progress Indicators.
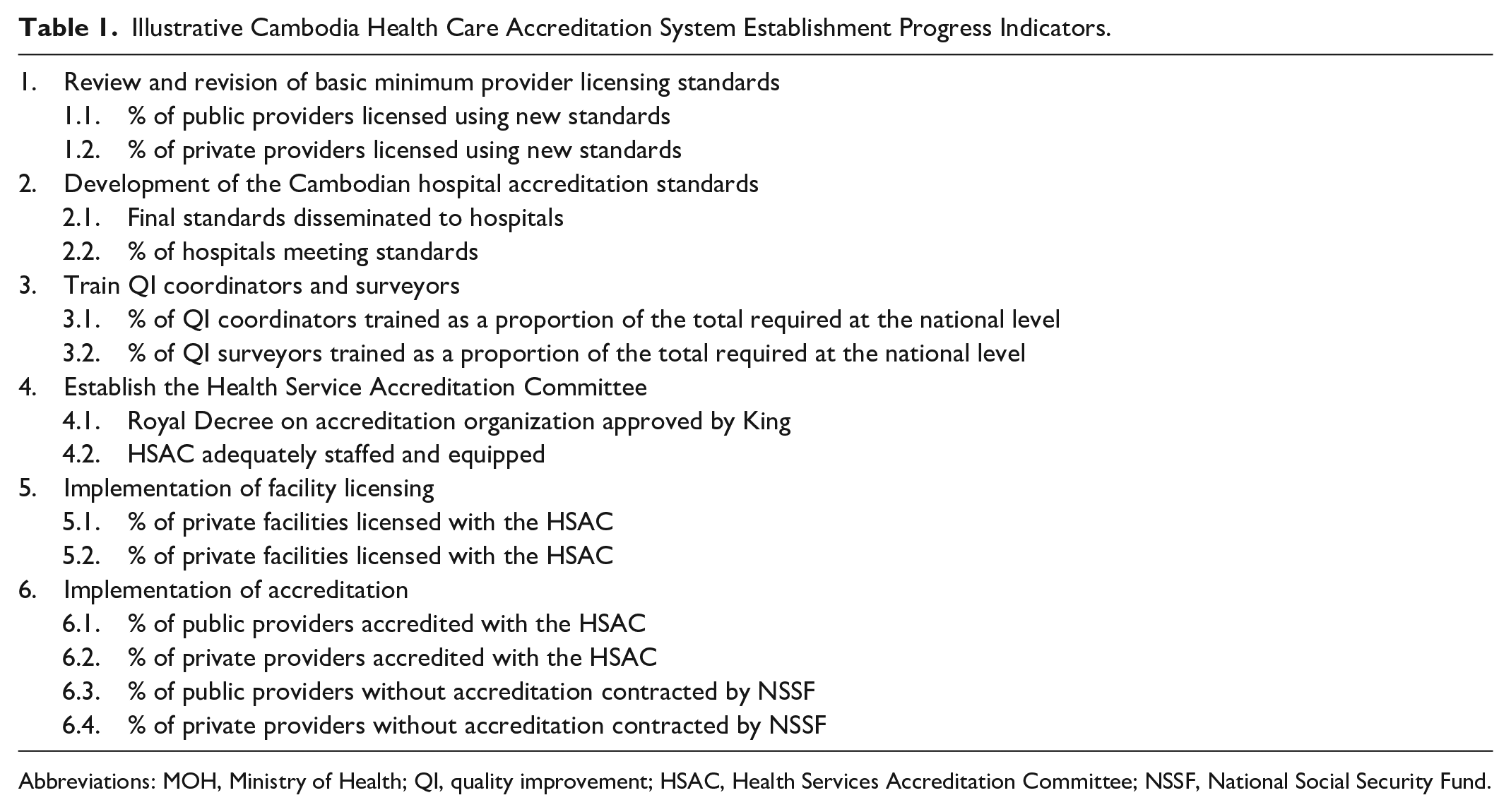
Abbreviations: MOH, Ministry of Health; QI, quality improvement; HSAC, Health Services Accreditation Committee; NSSF, National Social Security Fund.
Fourth, to ensure the independence of the accreditation organization, the drafting of related regulation should involve a neutral entity—specifically the General Secretariat for the National Social Protection Council.
Fifth, we suggest that quality indicators are integrated into the National Social Protection Monitoring and Evaluation system. 19 This will increase the profile of health care quality to the Ministerial level, thus ensuring a continued focus. This would also facilitate the evaluation of the proposed policy changes on improving health service quality.
Footnotes
Authors’ Note
The information and suggested approaches presented in this article do not necessarily represent the view or positions of the authors’ institutions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support for the research, authorship, and/or publication of this article: the USAID paid for the publication.