
Abstract
Reducing nosocomial transmission within health care facilities is important, but the number of negative-pressure airborne infection isolation rooms for SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) is limited. It is a daunting challenge to cope with a surge of suspected infectious patients in hospitals. We installed air exhaust fans on the windows to change the pressure direction within the wards rapidly. The best location for the fans was 90 cm from the floor and 90 cm from the edge of bed whether the indoor air conditioners were on or off. The noise level should be <60 dB(A) as per government regulations. General wards can be transformed into makeshift negative-pressure rooms easily and effectively within 24 hours, which is really the simple, fast, and effective way for the transformation being applied.
Keywords
Most Taiwan hospitals have used negative-pressure airborne infection isolation rooms (AIIRs) to house patients with suspected or confirmed airborne transmissible infections since the 2003 severe acute respiratory syndrome epidemic, 1 but the number of AIIRs is limited. With the ongoing novel coronavirus disease 2019 (COVID-19) pandemic, the number of individuals who need to be tested for COVID-19 has been increasing rapidly, while there are no regulations stipulating capacity requirements for hospitals, especially tertiary care (medical center) institutions. To cope with a surge of patients in hospitals who are suspected of the infection is challenging. 2 In addition, suspected cases should not be permitted to wait alongside other patients seeking medical care for other complaint diseases. They should be placed in a separated, fully ventilated room and approximately 2 m away from other patients with convenient access to respiratory hygiene supplies. 3
Kaohsiung Medical University Hospital (KMUH) started to prepare for COVID-19 on January 21, 2020, and infection control measures were tightened to limit nosocomial transmission and health care–associated infection within health care facilities.
With an average of 9,838 people per square kilometer at Kaohsiung city, the population density of Taiwan ranks second highest worldwide, with 80% of its population concentrated in six municipalities. Moreover, Taiwan is one of only five countries and regions in the world that had not yet announced full suspension of schools and classes or required citizens to stay at home by March 31, 2020. Consequently, when it comes to the reception and treatment of suspected cases with SARS-COV-2 (severe acute respiratory syndrome coronavirus 2; COVID-19), it is not feasible to build mobile cabin hospitals with makeshift isolation wards or walk-through negative-pressure booths by expropriating hotels, schools, parks, or spacious buildings within cities, walk-through, 4 or drive-through experience.5,6 How to designate a specific hospital to diagnose and preempt quarantine patients with suspected COVID-19 and acute respiratory symptoms as a COVID-19 hospital is an essential challenge. This COVID-19 safety hospital will also operate a screening center during the COVID-19 epidemic. At the screening centers, prompt screening and specimen collection are important, but the safety of medical staffs and testees is the top priority. 6 Cross-contamination should also be minimized during the specimen collection process 7 and while waiting for the test result.
It is suggested that we either make use of existing wards in hospitals, as their utilization rate has fallen due to the COVID-19 outbreak, or build outdoor parking lots or transform them into makeshift quarantine observation wards. This would be the only way to respond to the influx of suspected cases into hospitals and to contain further infection as patients have to stay in negative-pressure booths while waiting for test results.
KMUH, a medical university affiliated hospital, has twice obtained Joint Commission International accreditation. It is a large-scale hospital with 1,710 beds, which provides outpatient services for 1.98 million person-times annually, and its annual length of stay is 546,500 days. In response to a surge in suspected patients after the outbreak of COVID-19, the hospital has been using general wards as quarantine observation wards for suspected patients while they wait for the test results of second-time screening.
The partitions in the wards are closely connected to the floor slabs, and windows stay tightly closed. Each ward is equipped with small and independent air conditioners (12 m3, including 2 m3 air supplement system for precooling external fresh air) for indoor circulation, airflow speed control, and cooling. Air exhaust fans are installed on the windows to change the pressure direction within the wards rapidly. Mist generators with 0.58 CC mist/minute and a maximum jet height of 50 cm based on ultrasonic wave oscillation are used to measure and optimize the direction of airflow so as to identify the best location for exhaust fan installation. After testing, the results are as follows:
Installation height of exhaust fans (Table 1)
1.1. Installed at a height of over 90 cm above the ground, the exhaust fan is unable to effectively expel the mist over a standard hospital bed and the mist scatters in a nondirectional way, which indicates that the droplets from the patients are likely to scatter and drift indoors, causing higher risk of infection for the health care workers attending patients. 1.2. Installation height of exhaust fans has no effect on the airflow from corridor into the ward. As the mist from the nursing station to corridor and into the ward keeps flowing in the correct direction, it means contaminated air in the ward is under effective control without outflow. 1.3. Regardless of the installation height of exhaust fans or the distance between the fan and the bed, indoor conditioners being on or off and air volume have no effect on mist flow direction. Therefore, when the patients or family members turn off the indoor AC, outflow of air from the contaminated zones to the corridors and nursing stations is not an issue for concern.
Distance between the bed and the exhaust fan
2.1. Exhaust fans installed 60 cm from the bed edge work best to expel mist. However, when the patient is in bed, the level of noise from the fan (63 dB(A)) exceeds the legal limit. 2.2. If the distance is 90 cm, the noise level will decrease to 58.2 db. On one hand, we should not move the bed so as not to compromise air-exhaust performance. On the other hand, noise level should be under control so that it will not cause discomfort or anxiety to patients.
8
Therefore, a designated area for the bed should be marked on the floor.
Testing Results in Makeshift Quarantine Observation Wards After Installation of Exhaust Fans.
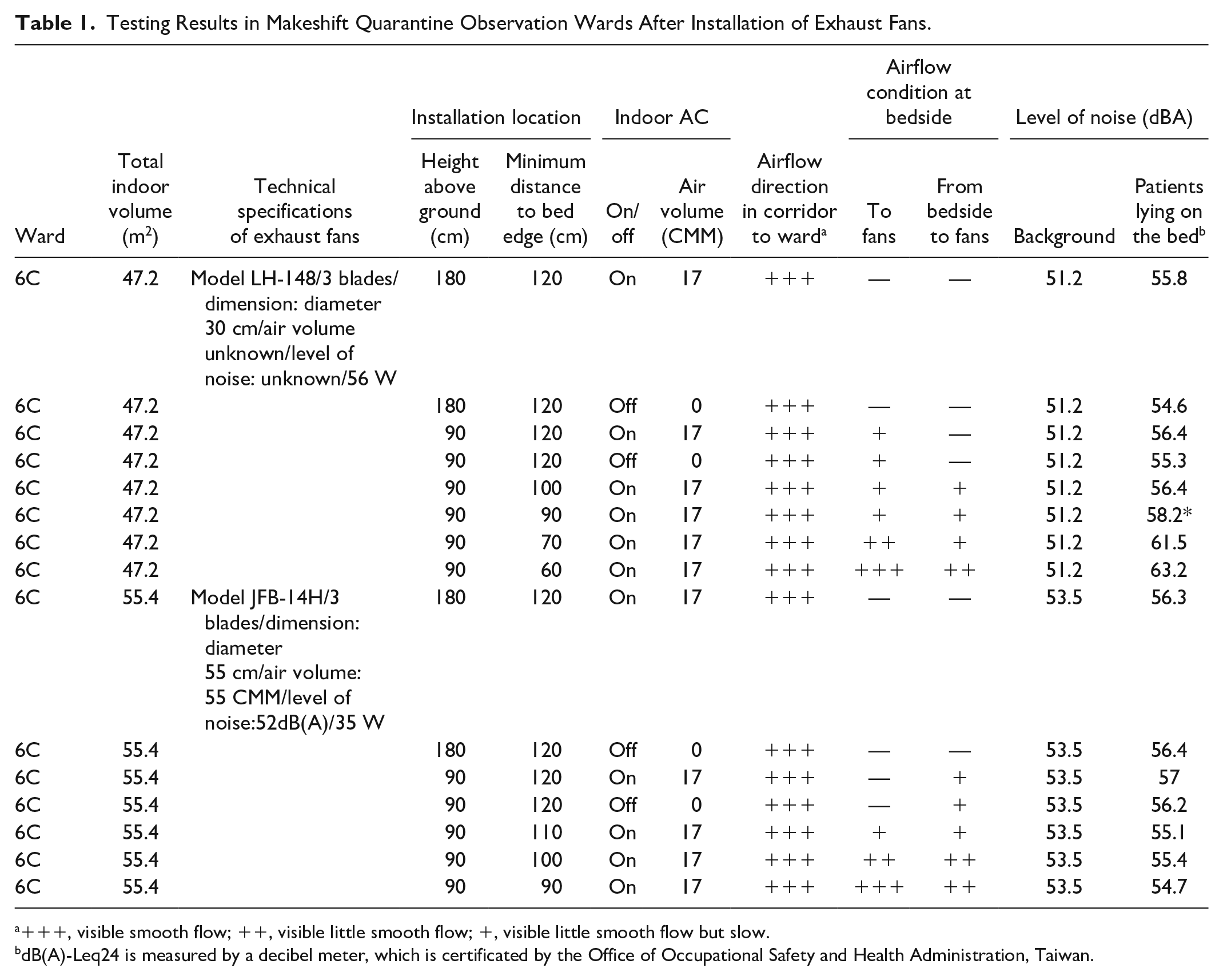
+++, visible smooth flow; ++, visible little smooth flow; +, visible little smooth flow but slow.
dB(A)-Leq24 is measured by a decibel meter, which is certificated by the Office of Occupational Safety and Health Administration, Taiwan.
There were a lot of empirical studies discussing and demonstrating how to build AIIRs,9-11 but to build a new AIIR is time consuming. The above-mentioned measures have been applied in the transformation of general wards into negative-pressure isolation rooms in Taiwan. Despite COVID-19 virus, exhaust fans are available on the market as they are not affected by international logistics and there is no need of customization or waiting for resumption of production lines. We found that a general inpatient ward area with 30 beds can easily, quickly, and effectively be transformed into makeshift negative-pressure rooms within 24 hours.
Footnotes
Acknowledgements
We thank the Institute of Public Health of Kaohsiung Medical University for use of their decibel meter to measure fan noise. We also thank all staff of the Infection Control Office, Occupational Health and Engineering & Maintenance Departments, and the COVID-19 Rapid Response Commission of Kaohsiung Medical University Hospital for their professional advice on setup of quarantine observation wards.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.