
Abstract
This study aimed to estimate the prevalence of current smoking among medical students in mainland China through a systematic search across 6 electronic databases for English or Chinese studies published before May 25, 2018. A total of 79 studies were included; 26 had a high risk of bias. The overall pooled prevalence of current smoking was 10.93% (7460/68 253; 95% confidence interval = 0.09%, 13.08%, I2 = 98.6%). This study found a decreasing prevalence of current smoking over the period studied (survey year range of 1988-2014). More specifically, the current smoking prevalence in males decreased progressively across time, while the prevalence in females remained relatively constant. The overall prevalence in the west was higher than in the middle or east of mainland China (P = .0061). The overall prevalence of current smoking increased with year in school (P = .0028). The present study provides a comprehensive synthesis of current smoking prevalence among medical students in mainland China. Although there have been some improvements in the status of tobacco use among medical students, given the leading role of physicians in tobacco control, sustained efforts are needed to curb the tobacco epidemic among medical students.
Introduction
Worldwide, tobacco use constitutes one of the greatest public health threats, accounting for 7 million deaths annually. 1 In China, the largest tobacco consuming nation in the world, over 1 million people die from tobacco use each year.2,3 Though the Chinese government has made great efforts to control tobacco use, the epidemic of use barely changed during the years 2010 to 2015.4,5 The overall prevalence of current smoking was 27.7% in adults aged 15 and older (52.1% male and 2.7% female), with an estimated 316 million current smokers by the end of 2015. 4 Among all age groups, current smoking prevalence was lowest in young adults aged 15 to 24 years, of whom 36.5% of the males were current smokers. 4
The importance of health care providers (HCPs) in tobacco control has been well documented.6,7 It is expected that medical education should serve to prevent HCPs from tobacco use. However, the rate of tobacco use among HCPs, especially male HCPs, is comparable with that of the general population in mainland China.8,9 Meanwhile, there has been increasing concern about smoking behavior among Chinese medical students, the future HCPs. A study indicated that the prevalence of lifetime smoking among male medical students increases significantly after the freshman year. 10 Data from a study involving 12 Chinese universities showed that the prevalence of lifetime smoking and current smoking among medical students was 53.9% and 26.8%, respectively. 11 Additionally, studies found that there was no difference in the smoking behaviors between medical students and nonmedical students.12-14 The entrance to college marks the transition from adolescence to adulthood, when risk-taking behaviors, such as smoking attempts, increase.15-17 As college is an important period when students initiate smoking and develop lifelong smoking habits, it is of strategic significance to implement antitobacco interventions during college.18,19
There are about 1.2 million medical students in mainland China. It is an urgent and challenging task to strengthen tobacco control in this population. Systematic estimates of current smoking prevalence during medical training are important to inform efforts to prevent and control the epidemic among medical students. National data for the past decade are missing, but a number of studies have addressed tobacco use among Chinese medical students in different cities. We conducted a systematic review and meta-analysis of published studies of current smoking among medical students in mainland China.
Methods
Search Strategy
We designed the protocol and data extraction forms according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (the PRISMA Statement20,21). We systematically searched the following databases for studies published prior to May 25, 2018: PubMed, Medline, Web of Science-Core Collection, China National Knowledge Infrastructure Project (CNKI), China BioMedical Literature Database (CBM), and Digital Journal of Wanfang Data (Wanfang). The literature was searched by combined keywords from the following concepts: population (medical student), outcome (tobacco, cigarette, or smoking), and study location (mainland China). Complete details of the search strategy appear in Appendix S1 (available in the online version of the article).
Study Selection and Eligibility Criteria
Inclusion criteria were studies that (1) reported data on Chinese medical students; (2) were conducted in mainland China; (3) provided a prevalence estimate or sufficient information from which the prevalence of current smoking could be calculated; and (4) were written in either English or Chinese.
In this study, current smoking was conceptually defined as “having ever smoked in the past 30 days.”18,22,23 In the literature, some studies defined current smokers by asking if a person had smoked at least 1 cigarette in 1 day in the past 30 days, whereas other studies classified current smokers into frequent/regular smokers (having smoked at least 1 cigarette per week) and occasional smokers (having smoked less than 1 cigarette per week). We included these modalities to maximize the number of included studies for estimation.
Studies that did not provide a prevalence estimate or sufficient information from which a prevalence could be calculated were excluded. Articles were also excluded if they were qualitative studies, literature reviews, conference abstracts, or intervention evaluations. In terms of duplicated data, the study with the maximum sample size and the most comprehensive results was included.
One author (YL) ran the literature search strategy. All studies were imported to the literature management software EndNote (version X7, Thomson ResearchSoft) to eliminate duplicated records. Two authors (LN and YL) independently reviewed titles and abstracts to remove studies that failed to meet the eligibility criteria. Two authors (LN and YL) then individually reviewed the full texts in detail to confirm eligibility. Inconsistencies were discussed, and wherever a consensus could not be reached by mutual discussion, the matter was referred to a third author (DL).
Data Extraction and Risk of Bias Assessment
Two authors (LN and YL) extracted data from the eligible studies including the following: name of the first author, year of publication, study year, study site, study design, sampling method, study population (sample size, gender distribution, and age/grade), and current smoking data.
The same 2 authors independently assessed the risk of bias of the included studies. As we focused on the prevalence of current smoking for this review, a 5-item appraisal checklist based on the scoring systems developed by Loney et al 24 and Kim et al 25 was applied. The checklist evaluated sample size (>700 vs ⩽700), sampling method (random vs convenience or unclear), participation rate (reported vs unreported or <80%), study year (provided vs not provided), and study site (provided vs not provided). Total scores ranged from 0 to 5, such that the lower the score, the higher the risk of bias. A third author (DL) resolved discrepancies through discussion and adjudication. Data extraction and risk of bias assessment were performed with Excel (version 2013, Microsoft Corporation).
Data Synthesis and Analysis
We applied the MetaProp module in the R version 3.2.3 (R Foundation for Statistical Computing) for the meta-analysis of current smoking prevalence. The prevalence reported in each study was logit transformed prior to computing the pooled prevalence. We used random-effect models to compute the pooled estimates of prevalence. Statistical heterogeneity was assessed using I2, with thresholds of ⩾25%, ⩾50%, and ⩾75% indicating low, moderate, and high heterogeneity, respectively. We conducted a sensitivity analysis by excluding studies with a high risk of bias and used Egger’s test to assess publication bias. To investigate heterogeneity, we performed subgroup analyses by study year, gender, region, and grade, using random-effects meta-regression analysis to explore the subgroup differences.
Results
Search and Study Selection
Our electronic search yielded 1013 hits, of which 427 duplicates were retrieved and 358 irrelevant articles were excluded by review of the title or abstract. We assessed 228 full-text articles for eligibility. Of these studies, 33 studies used duplicated data; 79 did not specify definitions/measures of smoking behaviors; 26 did not provide data on current smoking; 1 was not conducted in mainland China; and 10 used an irrelevant study design. After removal of these studies, a total of 79 studies published between 1990 and 2016 were included in this systematic review; 74 of these publications were in Chinese and 5 in English11,26-29 (Figure 1).
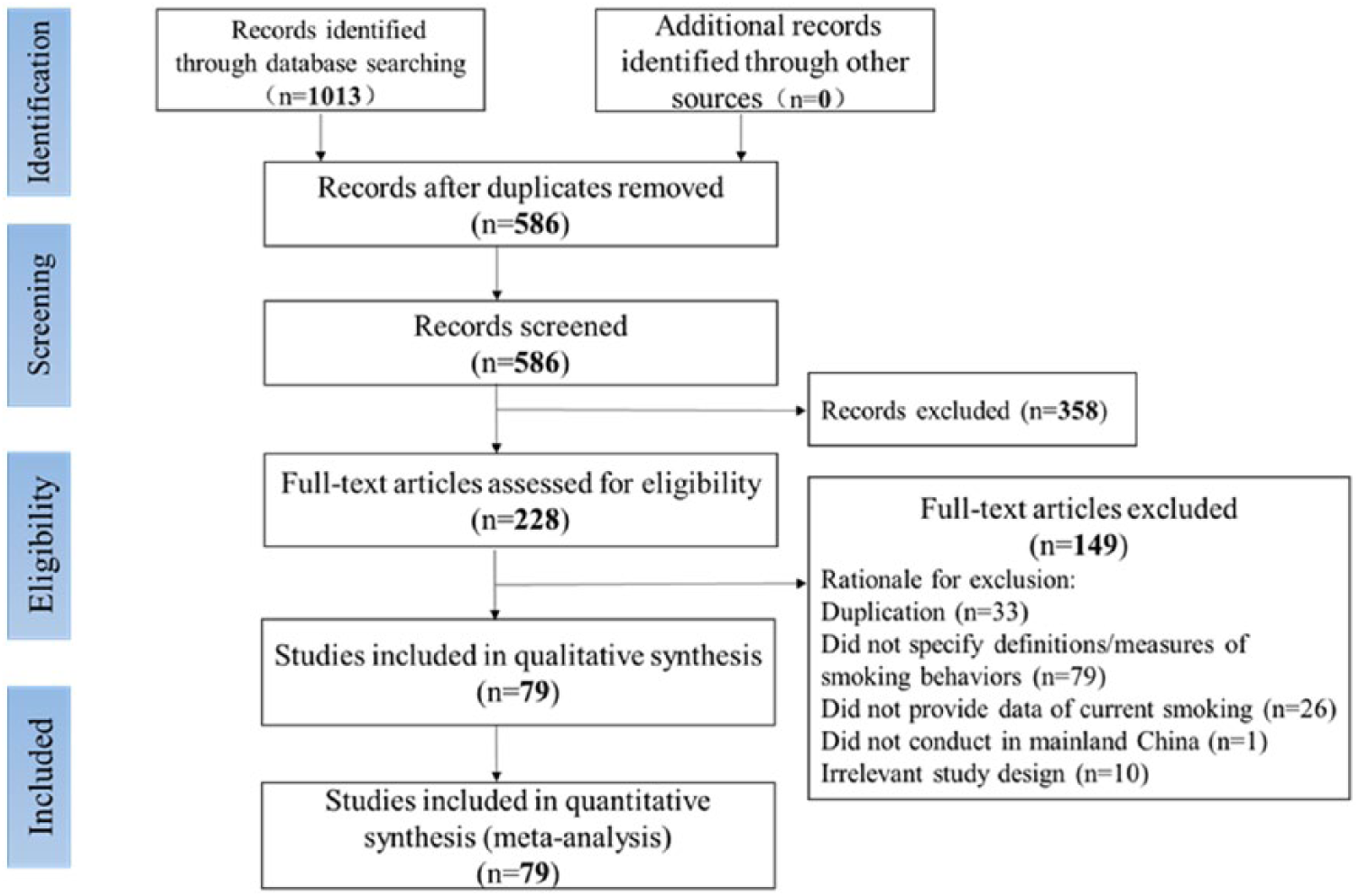
Flowchart for study selection of smoking behaviors among medical students in China.
Characteristics of Studies
All 79 studies were cross-sectional and used self-administered questionnaires to collect data. Eighteen studies (22.7%) were conducted in 1988 to 1999,11,26,30-45 14 (17.7%) in 2000 to 2009,14,46-58 and 11 (13.9%) in 2010 to 2014.28,29,59-67 By region, 33 studies (41.8%) were conducted in the east of China,* 14 (17.7%) in the central region, † 13 (16.5%) in the west, ‡ and 2 in multiple regions.29,96 The samples of most studies included both female and male subjects (n = 65), among which males were ⩾50% of the sample in 42 studies (53.2%), and 7 (8.9%) did not specify the gender distribution § ; 12 studies included only male medical students ‖ and 1 study included only females. 57
With regard to the risk of bias, the mean score was 3 (interquartile range = 3-4), and 26 studies (32.9%) were at high risk of bias, having scores lower than 3. Moreover, 36 studies (45.5%) did not specify the study date and 17 (21.5%) did not specify the study site, while 31 studies (39.2%) used convenience or nonrandom sampling and the methods of data collection were unreported or unclear in 14 studies (17.7%).¶28,37,38,41,42,46,49,68,69,71,85,97,99,100 Sample sizes ranged from 59 97 to 7135, 96 and 42 studies (53.2%) had a sample size larger than 700. Responses rates ranged from 79.2% to 100%, while 15 (19.0%) did not specify the response rates.#11,31,34,35,39,40,42-44,47,68,71,72,85,93 Characteristics and risk of bias scores of the 79 studies are provided in Supplementary Table S1 (available in the online version of the article).
Prevalence of Current Smoking Among Medical Students
There were 65 studies that reported the overall prevalence of current smoking in Chinese medical students,** which ranged from 0.81% 72 to 50.37%. 35 Significant evidence of between-study heterogeneity was found (I2 = 98.6%, P < .001). As shown in Table 1, sensitivity analysis did not identify any significant pattern (ie, removal of the identified study with the factor did not result in a substantially reduced I2). Thus, all 65 studies involving a total of 68 253 individuals were included in the meta-analysis. The overall pooled prevalence of current smoking was 10.93% (95% confidence interval [CI] = 9.09%, 13.08%). Among current smokers, we defined people who had smoked over 4 times or 4 cigarettes every week in the past 30 days as current frequent smokers. Seventeen studies reported the prevalence of current frequent smoking, †† which ranged from 0.81% 72 to 39.4%. 38 The pooled prevalence of current frequent smoking was 8.59% (95% CI = 6.20%, 11.78%) with high heterogeneity (I2 = 97.9%, P < .001).
Sensitivity Analysis.
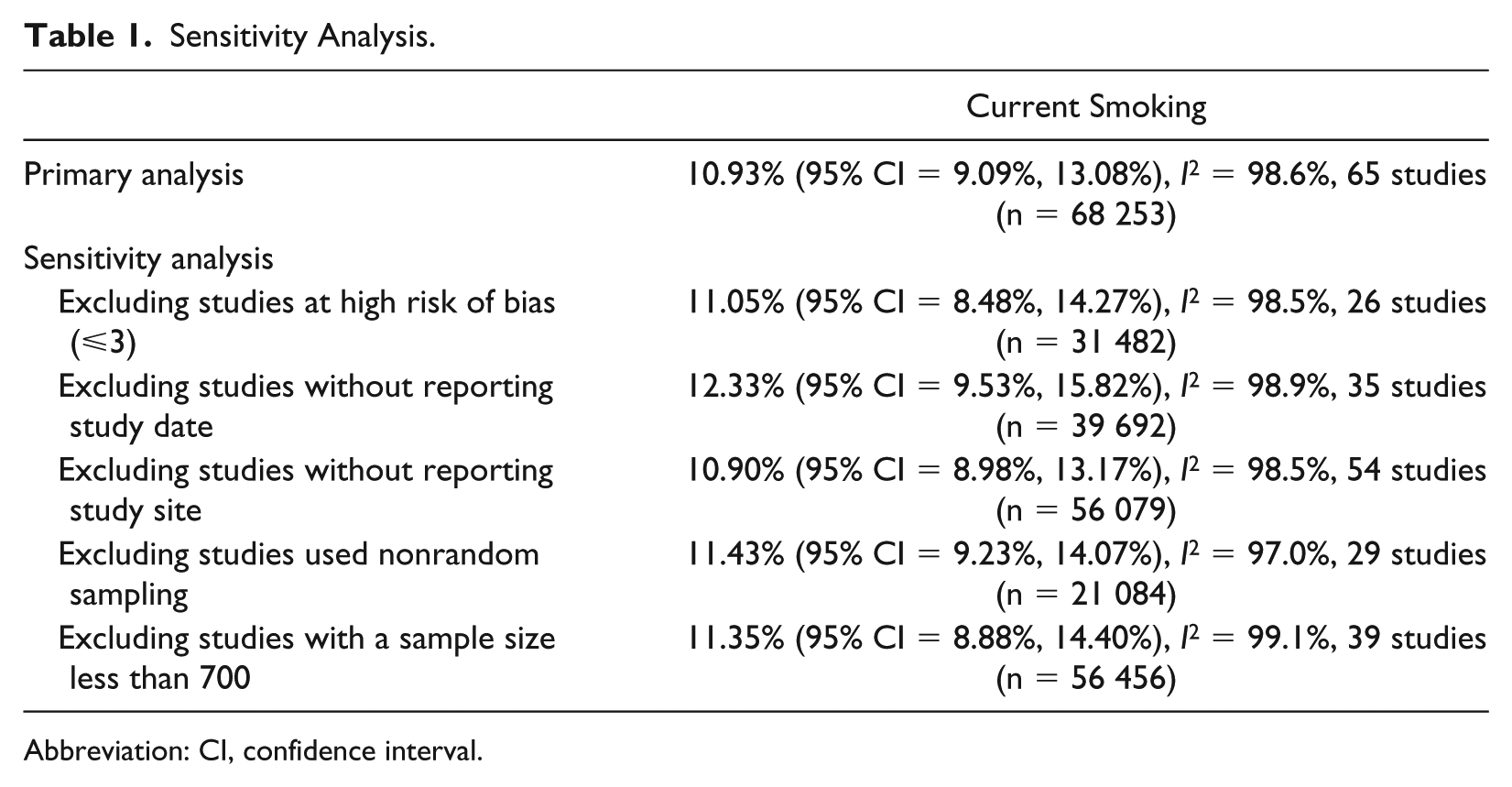
Abbreviation: CI, confidence interval.
According to Egger’s test, significant publication bias was found among the 65 studies, with smaller studies yielding more extreme prevalence estimates (Egger’s bias = −10.57, t = −4.59, P < .001).
Time Trend in Current Smoking Among Medical Students
As shown in Figure 2 and Table 2, the overall prevalence of current smoking among medical students decreased from 17.22% (95% CI = 12.17%, 23.81%) in 1988 to 1999 to 7.64% (95% CI = 5.60%, 16.74%) in 2010 to 2014 (P = .021).
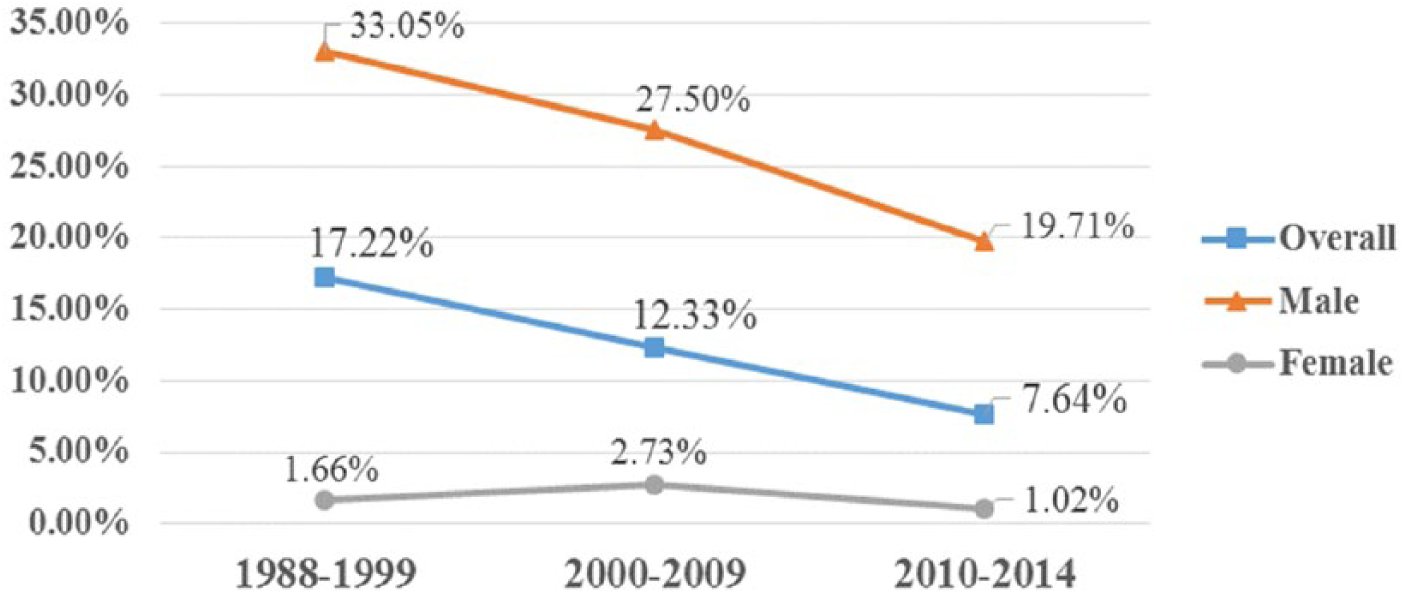
Time trend in current smoking among medical students.
Pooled Estimates of Current Smoking Among Chinese Medical Students.
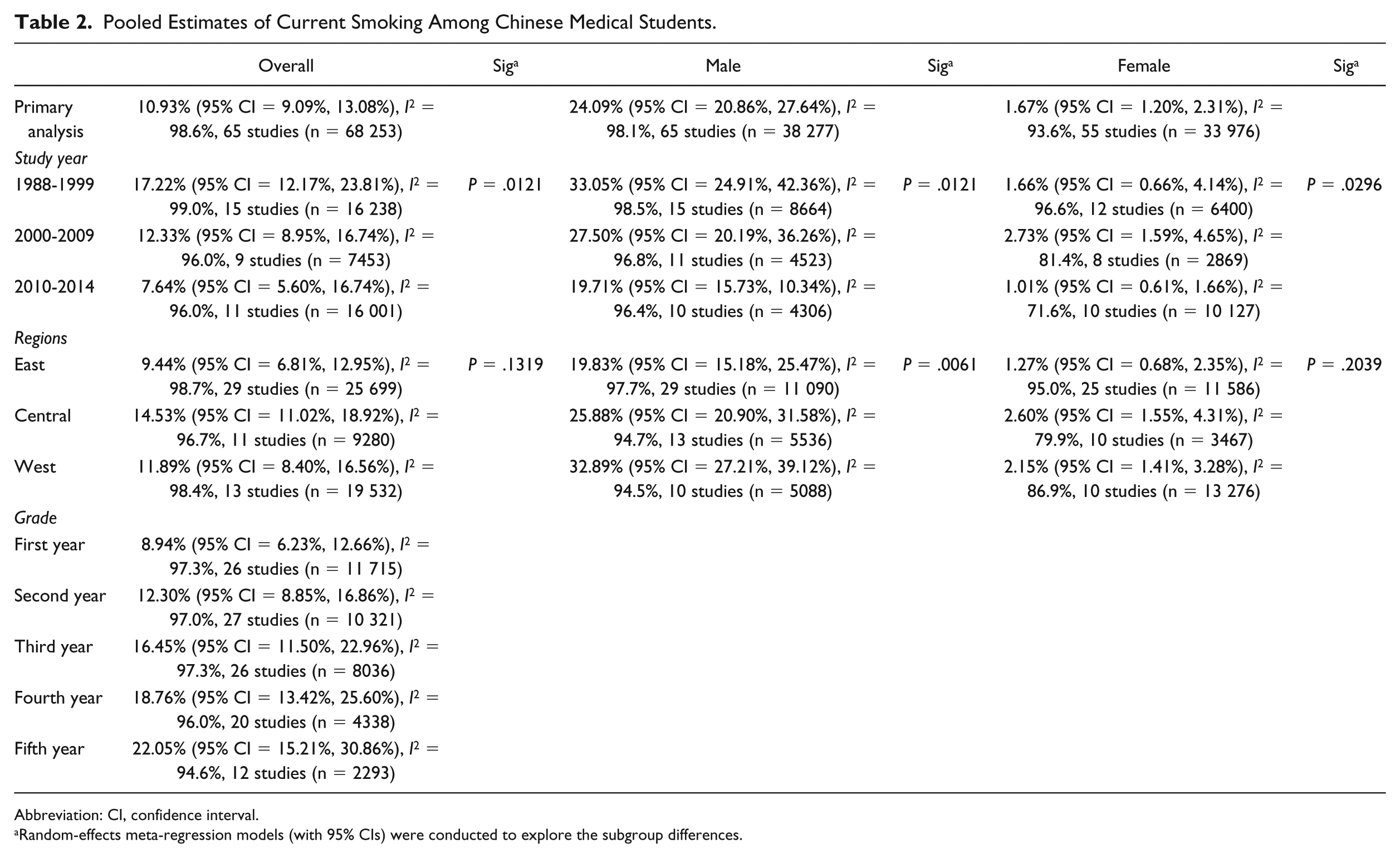
Abbreviation: CI, confidence interval.
Random-effects meta-regression models (with 95% CIs) were conducted to explore the subgroup differences.
Prevalence of and Time Trends in Current Smoking by Gender
Significant gender differences were found; 67 and 55 studies reported the smoking prevalence in male ‡‡ and female §§ medical students, respectively. The pooled prevalence of current smoking was 24.09% (9221/38 277; 95% CI = 20.86%, 27.64%, I2 = 98.1%) in male medical students and 1.67% (567/33 976; 95% CI = 1.20%, 2.31%, I2 = 93.6%) in female medical students.
As shown in Figure 2 and Table 2, the current smoking prevalence among male medical students decreased progressively from 33.05% (95% CI = 24.91%, 42.36%) in 1988 to 1999 to 19.71% (95% CI = 15.73%, 10.34%) in 2010 to 2014 (P = .0121). Compared with the prevalence in males, the current smoking prevalence in female medical students remained relatively constant. The prevalence in females was 1.66% (95% CI = 0.66%, 4.14%) in 1988 to 1999, which increased slightly to 2.73% (95% CI = 1.59%, 4.65%) in 2000 to 2009, and then decreased to 1.01% (95% CI = 0.61%, 1.66%) in 2010 to 2014.
Prevalence of Current Smoking by Region
As shown in Table 2 and Figure 3, no statistically significant regional differences in overall prevalence estimates were noted (P = .1319). Regional differences in current smoking prevalence were found in male medical students (P = .0061), among whom the prevalence in the west was higher than that in the middle and the east of China. The prevalence in females did not differ statistically by region (P = .2039).
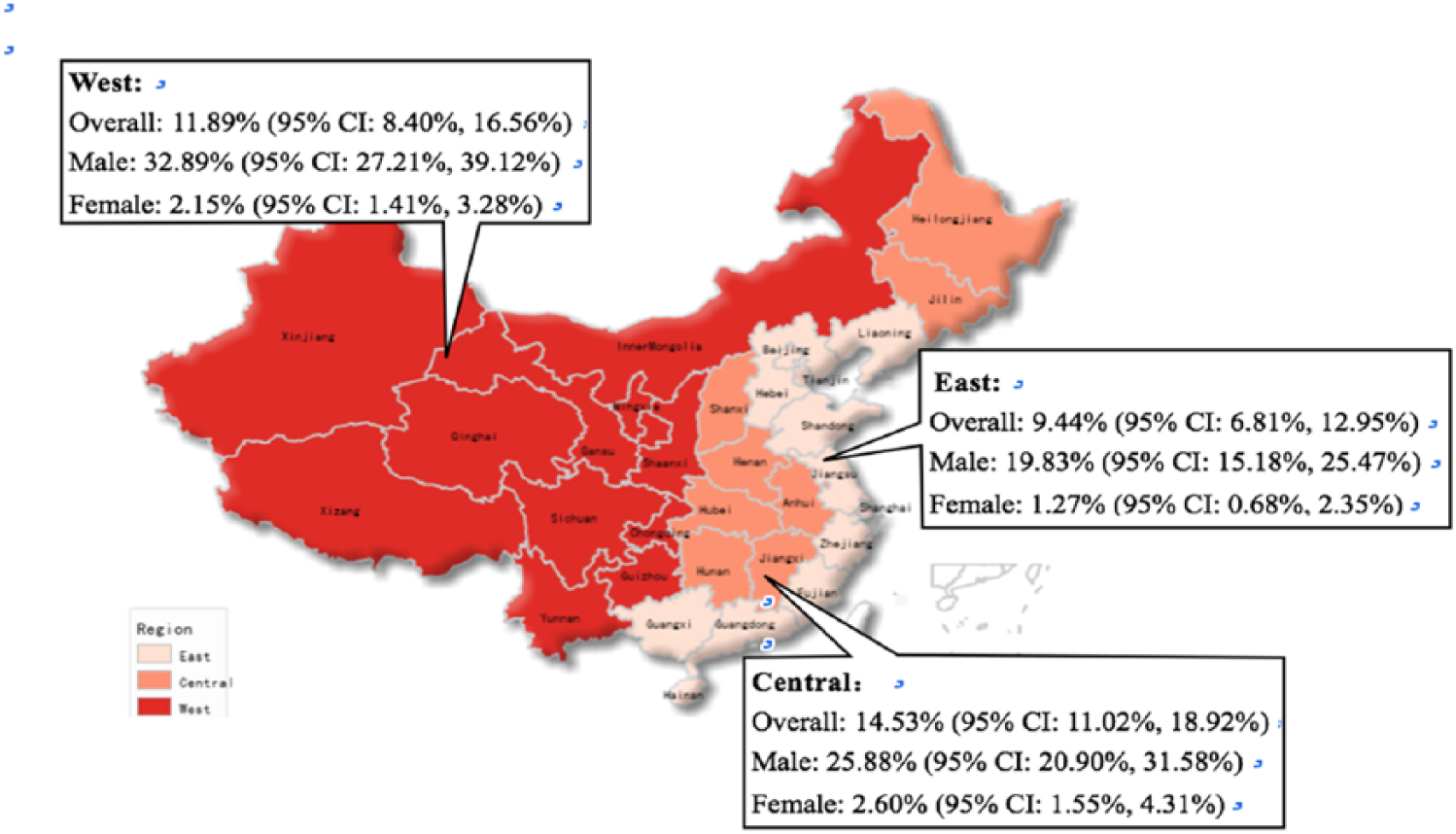
Prevalence of current smoking by regions in mainland China.
Prevalence of Current Smoking by Year of Study
As shown in Table 2, the overall current smoking rate increased with the year of medical school (P = .0028), from 8.94% (95% CI = 6.23%, 12.66%) among first-year students to 22.05% (95% CI = 15.21%, 30.86%) among fifth-year students.
Discussion
This systematic review and meta-analysis aimed to provide an overview of current smoking among medical students in mainland China. The overall pooled prevalence of current smoking derived from 65 identified studies involving 68 253 medical students was 10.93% (range = 0.81% 72 to 50.37% 35 ), which was lower than the corresponding prevalence among Chinese undergraduates (22.8%) 23 and American college students (28.5%). 18 Current smoking prevalence has decreased over the following 3 periods: 1988 to 1999, 2000 to 2009, and 2010 to 2014.
These findings reflect the long-term joint efforts of the Chinese government, researchers, and respective HCPs. Take the smoke-free campus campaigns as an example. According to the latest survey conducted by the Chinese Association on Tobacco Control about the smoke-free environment in campus, all universities have been equipped with smoke-free signs, no cigarette advertisements are allowed on campus, and decreased numbers of cigarette butts and smoking sets have been found. 103 However, smoking was still frequently observed in school cafeterias and male dorms. 103 In the present study, we have also found that current smoking rates were higher in medical students in the higher years of study, which demonstrates a deficiency in current education on tobacco control. Given that current smoking behavior is also still highly prevalent among Chinese physicians5,104 and teachers in medical schools, 105 and that preventing young people from smoking represents the best strategy against the epidemic of tobacco use, there is an urgent need to strengthen tobacco control education among medical students.
As observed previously in China and many other Asian countries, large and persistent gender differences in tobacco use have also been found in the present study.7,22,106 Our meta-analysis estimates that 24.09% of male medical students are current smokers, whereas 1.67% of their female counterparts currently smoke. These figures were still higher than the estimated rates among Chinese adolescent males, 22 which indicates that a portion of the students become current smokers after entering college despite their medical education. Among female medical students, the current smoking prevalence has fluctuated around 1% to 2% across time. However, previous studies have found an upward trend of current smoking among female adolescents since the 1980s, which might be related to economic globalization, urbanization, and aggressive promotion by tobacco industries.22,23 Thus, these findings indicate the need for target-oriented programs to prevent male medical students from smoking from their freshman year on and to promote cessation among those who smoke; meanwhile, efforts are continually needed to keep the prevalence of female smokers low.
We also found that current smoking among male medical students in the west of China was most prevalent. This may result from differences in the social, economic, and political environment in different parts of China.23,107,108 First, most of the antitobacco efforts, including tobacco control and prevention as well as the provision and delivery of cessation services, have been implemented in cities with a higher level of socioeconomic development, like those in eastern China. The implementation and supervision of smoking ban policies in eastern China are also better. Second, Chinese social norms have been the subject of much discussion as contributing factors to tobacco use. 105 With the relative lack of efforts to modulate tobacco use, people in the central and western regions of China are more likely to be exposed to a pro-smoking culture than those in the east.109,110 More tobacco control efforts are needed in the central and western regions of China.
This study has some limitations. First, the data were derived from studies that had different designs, smoking definitions, and sample demographics. The substantial heterogeneity among the studies remained largely unexplained by the variables inspected. Second, most studies included in this meta-analysis used convenience or nonrandom sampling without clarification as to when and where the study was conducted. The limited number of studies for several periods prevents this study from being able to systematically assess the impact of geographic differences through meta-regression analysis. Caution is thus needed when interpreting the results. Third, the analysis relied on aggregated published data. A multicenter, prospective study using a standardized definition of current smoking in a random subset of participants would provide a more accurate estimate of the prevalence of current smoking among medical students in mainland China.
Conclusions
The present study provides a comprehensive synthesis of the prevalence and trends of current smoking among medical students in mainland China. Our results have shown a decreasing prevalence of current smoking in general, particularly among male medical students. Still, there is a need for target-oriented programs to prevent male medical students from taking up smoking after entering college and to promote cessation among those who smoke. The prevalence of current smokers in female medical students remained relatively constant. The large and persistent gender differences in tobacco use may be the result of social norms encouraging men to smoke but discouraging women. To change these social norms, continuous effort is needed. Regional differences of current smoking prevalence among male medical students were found as well. More antismoking efforts, including tobacco control and prevention and the provision and delivery of cessation services, are needed in the center and west of mainland China. The prevalence of current smoking is higher in students in later years of medical school, indicating a deficiency in current education on tobacco control. Although there have been some improvements in tobacco use among medical students, given the leading role of physicians in tobacco control, a sustained and comprehensive effort is needed to curb the tobacco epidemic among medical students.
Supplemental Material
Appendix_S1 – Supplemental material for Current Smoking Behavior Among Medical Students in Mainland China: A Systematic Review and Meta-Analysis
Supplemental material, Appendix_S1 for Current Smoking Behavior Among Medical Students in Mainland China: A Systematic Review and Meta-Analysis by Lu Niu, Ying Liu, Dan Luo and Shuiyuan Xiao in Asia Pacific Journal of Public Health
Supplemental Material
Table_S1 – Supplemental material for Current Smoking Behavior Among Medical Students in Mainland China: A Systematic Review and Meta-Analysis
Supplemental material, Table_S1 for Current Smoking Behavior Among Medical Students in Mainland China: A Systematic Review and Meta-Analysis by Lu Niu, Ying Liu, Dan Luo and Shuiyuan Xiao in Asia Pacific Journal of Public Health
Footnotes
Acknowledgements
We would like to express our gratitude to Yang Yu and Yunxiang Huang (Central South University) for their kindest contributions and assistances to this study. We would also like to acknowledge Dr Fengsu Hou (Sun Yat-sen University) and Dr Wei Zhou (Central South University) for their assistance with manuscript editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the China Medical Board (09970).
Supplemental Material
Supplemental material is available for this article online.
**
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.