
Abstract
Microtubules are multifunctional cytoskeletal proteins that are involved in crucial cellular roles including maintenance of cell shape, intracellular transport, meiosis, and mitosis. Class III beta-tubulin (βIII-tubulin, also known as TUBB3) is a microtubule protein, normally expressed in cells of neuronal origin. Its expression was also reported in various other tumor types, such as several types of lung cancer, ovarian cancer, and esophageal cancer. TUBB3 is of clinical relevance as overexpression has been linked to poor response to microtubule-targeting anti-cancer drugs such as taxanes. To systematically investigate the epidemiology of TUBB3 expression in normal and neoplastic tissues, we used tissue microarrays for analyzing the immunohistochemically detectable expression of TUBB3 in 3911 tissue samples from 100 different tumor categories and 76 different normal tissue types. At least 1 tumor with weak expression could be found in 93 of 100 (93%) different tumor types, and all these 93 entities also had at least 1 tumor with strong positivity. In normal tissues, a particularly strong expression was found in neurons of the brain, endothelium of blood vessels, fibroblasts, spermatogenic cells, stroma cells, endocrine cells, and acidophilic cells of the pituitary gland. In tumors, strong TUBB3 expression was most frequently found in various brain tumors (85%–100%), lung cancer (35%–80%), pancreatic adenocarcinoma (50%), renal cell carcinoma (15%–80%), and malignant melanoma (77%). In summary, these results identify a broad spectrum of cancers that can at least sporadically express TUBB3. Testing of TUBB3 in cancer types eligible for taxane-based therapies could be helpful to identify patients who might best benefit from this treatment.
Introduction
Microtubules are components of the cytoskeleton formed due to polymerization of dimeric structures composed of alpha- and beta-tubulins playing crucial roles in normal and cancerous cells including maintenance of cell shape, intracellular transport, meiosis, and mitosis. 1 They are dynamical structures that undergo continual assembly and disassembly in a cell. 2 Beta-tubulins exist as multiple isotypes with a complex pattern of distribution among different tissues. 3 Isotypes have been divided into several classes with distinct structural properties. Class III beta-tubulin (βIII-tubulin, encoded by the TUBB3 gene) is normally expressed at high levels in cells of neuronal origin but has also occasionally been found in several extra neuronal tissues including testes, placenta, small intestine, and colon. 3
Aberrant expression of TUBB3 has been reported from a multitude of human cancer types, such as malignant melanoma, 4 non–small cell carcinoma, 4 adenocarcinoma of the colon, 5 ductal adenocarcinoma of the pancreas, 6 renal cell papillary carcinoma, 7 medulloblastoma, and oligodendroglioma 8 and has been linked to adverse tumor phenotype and poor clinical outcome in some of them.7,9
Alteration of TUBB3 in human cancers is of considerable clinical interest, because it has been linked to reduced response to taxane- and epothilone-based therapies.10,11 For example, poor efficacy of microtubule-targeting anti-cancer drugs was reported from cancers with TUBB3 overexpression including non–small cell lung cancer, 12 uterine serous carcinoma, 11 advanced gastric cancer, 13 breast cancer,13,14 and ovarian cancer. 15
Tubulin-binding drugs inhibit microtubule dynamics required for DNA segregation and cell division, and, as a result, kill cancerous cells. 16 As the number of studies suggesting biological and clinical relevance of βIII-tubulin is rapidly increasing, there are also a growing number of reports showing considerable discrepancies with respect to the frequency of expression in various cancer types. For example, reported frequencies on βΙΙΙ-tubulin expression ranges from 17% to 85% in non–small cell lung cancer,17,18 from 20% to 67% in serous ovary cancer,15,19 from 10% to 100% in colon adenocarcinoma, 5 and from 12% to 100% in prostate cancer.19,20 These discrepancies are obviously due to the use of different antibodies and staining protocols in these studies.
The optimal approach for assessing the relative importance of a potentially relevant molecule across human tumor types includes the analysis of as large as possible number of different cancer types and subtypes together with a systematic evaluation of corresponding normal tissues. Moreover, it would be necessary to ensure a maximal standardization of all these analyses. The tissue microarray (TMA) technology is a suitable tool for such studies, as a large number of tissues can be analyzed on few TMA sections that are cut and stained in one day and in one set of reagents at completely identical staining conditions.
In this study, we took advantage of a set of preexisting TMAs containing more than 3900 samples from 100 different tumor types and subtypes as well as from 67 different normal tissues including more than 600 normal cell types. These tools enabled us to generate a comprehensive report on the frequency and levels of TUBB3 expression across tumor entities and normal cell types.
Materials and methods
Tissues
Two different sets of TMAs made from surgically removed organ parts, which were formalin-fixed and paraffin-embedded tissue samples, were used to study βIII-tubulin expression. The first was a normal TMA: Healthy tissue taken from organs operated for non-tumor reasons were composed of 8 samples each of 76 different normal tissue types (608 samples on one slide). The second TMA contained 3–92 (total: 3911) samples each from 100 different human tumor types and subtypes. 21 The samples of this second TMA were distributed among 8 different TMA blocks each containing between 454 and 532 samples. The exact composition of the TMA is given in the Results section. For both the TMA sets, tissue cylinders with a diameter of 0.6 mm were punched from tumor areas of each tissue block and brought into a recipient paraffin block using the paraffin sectioning aid system (adhesive-coated slides (PSA-CS4x), adhesive tape, and ultraviolet (UV) lamp; Instrumedics, Inc., Hackensack, NJ, USA). All tumor samples represented in these TMAs were obtained from the archives of the Institute of Pathology of the University Medical Center Hamburg-Eppendorf. Archived diagnostic leftover tissues were used to prepare TMAs and analyzed as approved by the local ethics committee (Ethics commission Hamburg, WF-049/09 and PV3652). According to local laws (HmbKHG, §12,1) informed consent was not necessary. All work has been carried out in compliance with the Helsinki Declaration.
Immunohistochemistry
Freshly cut TMA sections were stained on one day and in one experiment. Primary antibody specific for TUBB3 (clone EPR1568Y rabbit monoclonal antibody; dilution 1:150; Abcam, Cambridge, MA, USA) was added; slides were deparaffinized by 3× xylene washings for 3 min and 100%, 96%, 80% ethanol washings for 3 min; and exposed to heat-induced antigen retrieval for 5 min in an autoclave at 121°C in Tris-ethylenediaminetetraacetic acid (EDTA)-citrate buffer (pH 7.8). Bound antibody was then visualized using the EnVision detection system Kit K5007 Peroxidase/DAB+, rabbit/mouse (Dako, Glostrup, Denmark). Staining in nerves and axons served as a positive control. The pathologist recorded staining intensity (0, 1+, 2+, 3+) and fraction of positive tumor cells for each tissue spot. A final score was built from these two parameters according to the following criteria: negative scores had staining intensity of 0; weak ones had a staining intensity of 1+ in ≤70% of tumor cells or 2+ in ≤30% of tumor cells; moderate had staining intensity of 1+ in >70% of tumor cells, staining intensity of 2+ in >30% and ≤70% of tumor cells, or staining intensity of 3+ in ≤30% of tumor cells; and strong scores had staining intensity of 2+ in >70% of tumor cells or staining intensity of 3+ in >30% of tumor cells. 22
Results
βIII-tubulin protein expression in normal tissues
The TUBB3 positive cell types in normal tissues are summarized in Table 1. Examples of TUBB3 positive normal tissues are given in Figure 1 and Figure S1.
Expression of TUBB3 in human normal tissues.

–: no detectable staining; +: weak staining; ++: moderate staining; +++: strong staining.
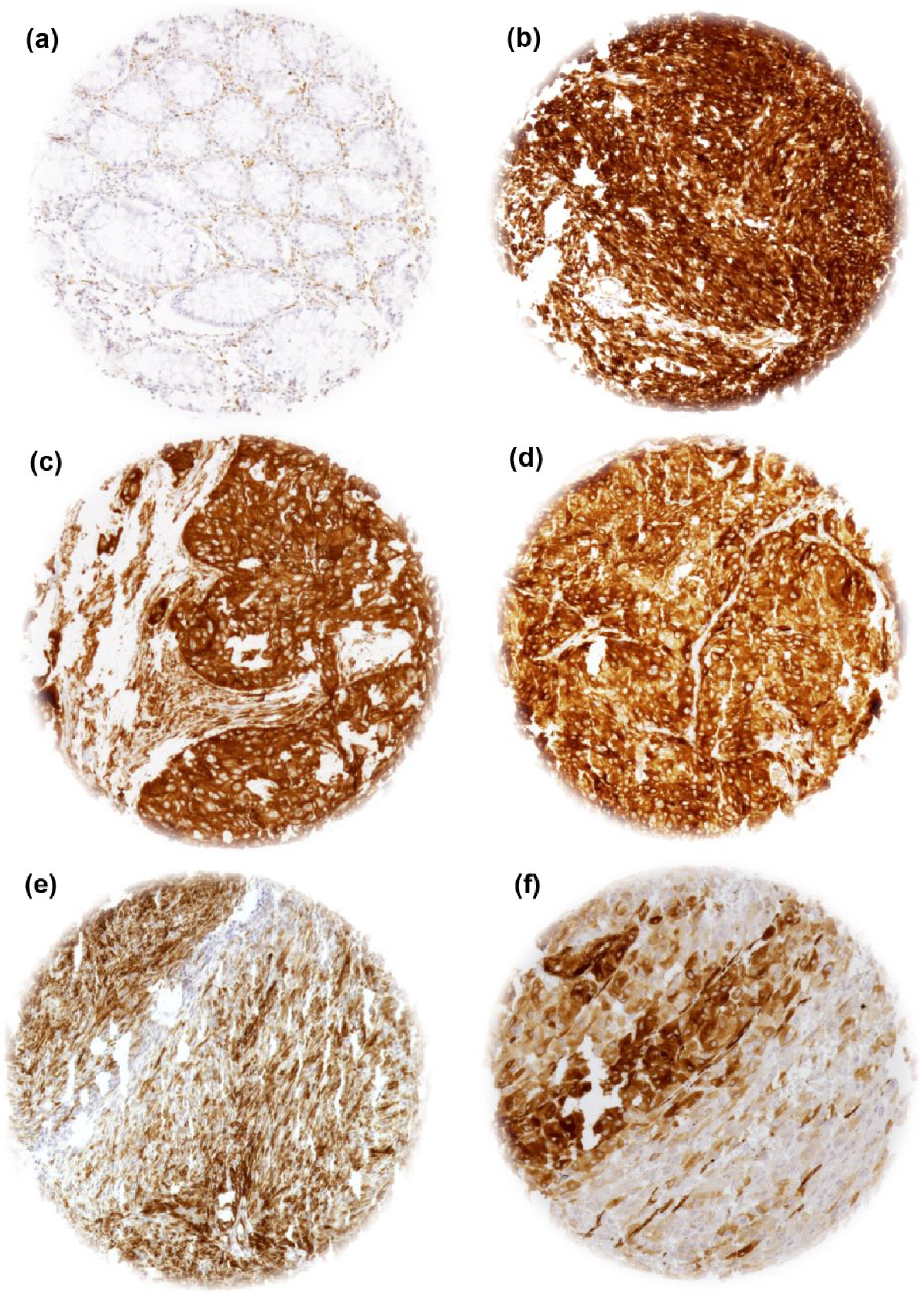
Representative images of TUBB3 staining in normal tissues and tumors: (a) normal colon, TUBB3 staining in endothelial cells and neurons, (b) gastrointestinal stromal tumor (GIST), (c) esophageal adenocarcinoma, (d) gall bladder cancer, (e) basalioma, and (f) malignant melanoma.
βIII-tubulin protein expression in tumors
βIII-tubulin expression was analyzable in at least 1 sample in 99 of the 100 arrayed tumor types. No result could be obtained from chrondrosarcomas, because the tissue spots were exhausted or lacked sufficient numbers of tumor cells. At least a weak βIII-tubulin protein expression could be detected in virtually all (93 of 98, 95%) of the analyzable tumor categories, all of which also contained at least one tumor spot with strong positivity. The immunohistochemical results are given in Table 2 for all tumor types having at least one positive case. βIII-tubulin positivity was most striking in neuronal tumors, including oligodendrogliomas and neuroblastomas, where all examined tumors showed strong positivity. As expected, other neuronal tumors, such as astrocytomas and pheochromocytomas, were also among the most frequently positive tumors. Frequent strong βIII-tubulin protein positivity was further seen in medullary thyroid cancers (17/20, 85%), malignant mesotheliomas (11/13, 85%), Hodgkin’s lymphoma (10/13, 77%), seminomas (44/66, 67%), and small cell lung cancers (8/10, 80%). Representative image of tumor types with strong βIII-tubulin positivity are shown in Figure 1. Tumor types without detectable βIII-tubulin protein expression under the selected experimental conditions included non-Hodgkin’s lymphomas (0 of 5), adenomas of the thyroid gland (0 of 48), lymphoepithelial carcinomas (0 of 1), leiomyomas (0 of 16), and haemangiopericytomas (0 of 4). However, the number of examined cases of several of these tumor types is low. These data therefore do not rule out that βIII-tubulin expression can sometimes also occur in these tumor types.
Expression of TUBB3 in human cancers.

IHC: immunohistochemistry; n: number of analyzed samples; SqCC: squamous cell carcinoma; NSCLC: non–small cell lung cancer; GIST: Gastrointestinal stroma tumor; nos: not otherwise specified.
Discussion
The study shows that high levels of βIII-tubulin protein expression are seen in a large variety of cancer types and subtypes suggesting that this protein may have considerable general importance in cancer biology. There were 66 tumor types that were newly identified as having at least an occasional βIII-tubulin protein overexpression in this study. These included many important cancer types such as squamous cell carcinoma of the skin, squamous cell carcinoma of the vulva and vagina, gastrointestinal stroma tumor (GIST), adenocarcinoma of the gall bladder, papillary adenocarcinoma of the pancreas, neuroendocrine carcinoma of the pancreas, seminoma, urothelial carcinoma, thyroid cancer, neuroblastoma, desmoid-tumor, and stroma-sarcoma.
A protein may have a particularly strong role for cancer biology in tumors where the target expression is substantially higher or lower than in its corresponding normal tissues. Such a result was found for overexpression in lung, thyroid gland, kidney, gastrointestinal tissues, and the breast. In particular, βIII-tubulin protein was overexpressed in lung cancer, breast cancer, thyroid cancer, squamous cell carcinoma of the skin, and basalioma, while lung tissue, thyroid tissue, and skin epithelium were largely βIII-tubulin protein negative. A significant role of βIII-tubulin protein in lung cancer, 12 ovarian cancer,15,19,23,24 and breast cancer 19 was already suggested demonstrating an independent prognostic impact in malignant melanoma, 25 ovarian cancer, 26 and non–small cell lung cancer. 27 Moreover, Zhang et al. 28 had shown that TUBB3 might be used as a prognostic marker for biomarker-guided chemotherapy in non–small cell lung cancer. A comparison of the results of earlier studies on TUBB3 expression with our own study is given in Figure 2.
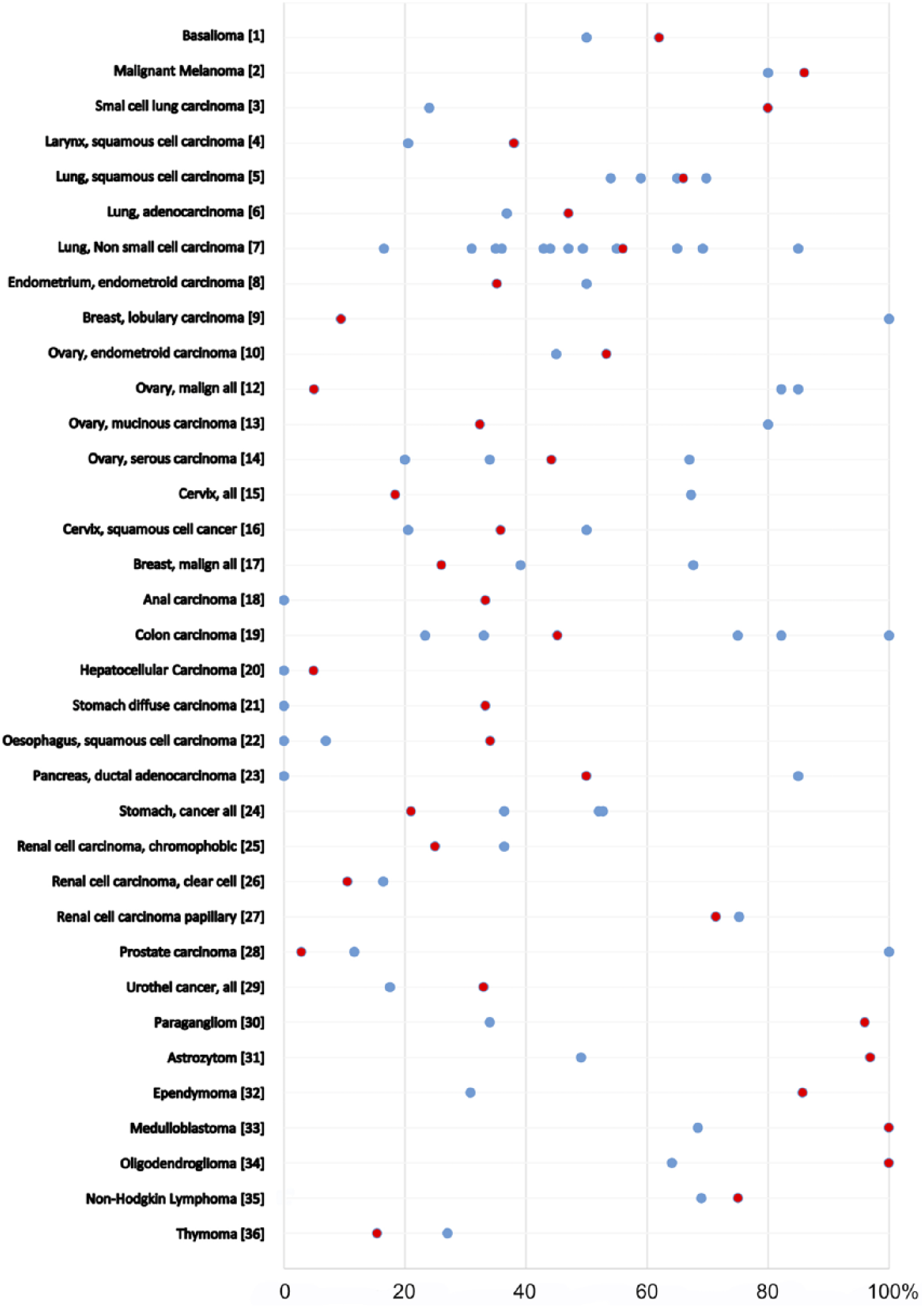
Percentage of TUBB3 cancers in previous studies (blue dots) as compared to the results of our study (red dots). Figures [1], 29 [2], 4 [3], 30 [4],31,32 [5],32,33 [6], 33 [7],5,12,18,34–42 [8], 19 [9], 19 [10], 15 [12], 15 [13], 15 [14],15,19,43 [15], 44 [16],19,31 [17],45,46 [18], 19 [19],5,19,47–49 [20], 50 [21], 19 [22],19,51 [23],6,19 [24],52–54 [25], 7 [26], 7 [27], 7 [28],19,20 [29], 55 [30], 56 [31], 8 [32], 8 [33], 8 [34], 8 [35],54,57 and [36]. 39
Importantly, TUBB3 showed marked expression differences between tumor types that are sometimes difficult to diagnose based on histological examination alone. This was most evident for thyroid gland lesion, where benign adenomas and carcinomas share similar histological features. Under the selected experimental conditions, TUBB3 staining was absent in thyroid gland adenomas (0/48) but present in a relevant fraction of thyroid papillary carcinomas (21/44, 48%) and thyroid follicular carcinomas (3/38, 8%). TUBB3 immunohistochemistry might thus be helpful to secure the diagnosis of thyroid carcinoma in case of positive staining. Potentially relevant differences in the TUBB3 expression frequency were also seen between papillary (11/14, 79%) and clear cell kidney cancers (5/38, 13%). This finding is in agreement with an earlier study on TUBB3 expression in a larger number of renal cell cancers by our group, 7 demonstrating that the results from the comparatively small numbers of samples per cancer type in this study are largely representative for the analyzed cancer types.
TUBB3 is of high clinical importance because overexpression has been linked to reduced response to taxane- or epithelione-based therapies.10,11 In fact, all cancer types with reported poor response to these drugs also showed high level and frequent TUBB3 staining in our TMA study, including, for example, non–small cell lung cancers, 12 breast,13,14 bladder, 55 prostate,19,20 esophageal, 51 testicular germ cell tumors, 58 penile cancer, 59 and ovarian cancers. 15 On the other end of the spectrum, our study identified hepatocellular carcinoma as a cancer type showing only occasional (5%) TUBB3 expression. Several in vitro studies have suggested that liver cancers may respond well to taxanes, 60 but the clinical value of taxanes in liver cancer patients is poorly understood. So far, only a small phase II study on 20 patients with unresectable liver cancers was undertaken but did not show a benefit from paclitaxel therapy. 33 The findings of our study may encourage further research on this topic. Our analysis provides an almost complete overview on βIII-tubulin protein expression in normal and neoplastic human tissues. TMAs are an ideal tool to massively accelerate characterization of novel biomarkers. The use of TMAs to screen normal tissues and different tumor types for molecular alterations of interest is an obvious application of this technique. Earlier, we had used comparable multitumor TMAs for the evaluation of calretinin, 61 KIT 62 and ERG. 63 It is a distinct advantage of the TMA technique that all tissues are analyzed under maximally standardized conditions. Although automated immunostainers—despite some remaining day-to-day variability—can provide good standardization of the staining process, TMAs enable a control of several additional important parameters affecting staining. For example, the TMA method enables to cut the sections of TMA blocks containing samples from 5000 samples within 1 h. If these sections were taken from regular tissue blocks, sectioning was likely to last several weeks. Several studies have demonstrated, however, that immunoreactivity of tissue sections decreases markedly over time.64–66 For most antibodies, storage of cut sections for 2 weeks already significantly impacts staining results.
In summary, the results of our study demonstrate that TUBB3 upregulation is a common feature that occurs at different frequencies in almost every type of cancer. Studies are needed to clarify whether TUBB3 testing in patients might predict response to microtubule-targeting anti-cancer drugs in a clinically relevant way.
Footnotes
Acknowledgements
The authors thank Janett Lütgens, Sünje Seekamp, and Inge Brandt for excellent technical support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.