
Abstract
Colorectal cancer incidence in patients undergoing screening protocols is decreasing because of the higher rate of discovered preneoplastic colonic lesions; however, adenomatous polyps may not always be removable endoscopically and surgery may still be necessary. The aim of this study was to assess the vascular endothelial growth factor expression in the different steps of colorectal carcinogenesis to explore its potential role as a marker of malignancy in polypoid lesions. A total of 92 subjects with colonic adenoma or cancer who underwent screening colonoscopy or surgery were prospectively enrolled. Real-time reverse transcription polymerase chain reaction for VEGF-A messenger RNA expression and immunohistochemistry for VEGF-A were performed. Immunoassays for VEGF-A, VEGF-C, VEGFR-1, VEGFR-2, and VEGFR-3 were also performed. Non-parametric statistics, receiver operating characteristic curve analysis, and logistic multiple regression analysis were used. VEGF-A messenger RNA expression was higher in patients with high-grade dysplasia or colorectal cancer than in those with low-grade dysplasia adenomas (p = 0.01). At immunohistochemistry, VEGF-A expression was significantly higher in colorectal cancer patients compared to dysplastic adenomas (p < 0.001), and the accuracy of VEGF-A expression for prediction of malignancy was 91.7 (95% confidence interval = 78.7–97.9). VEGF-C protein expression was lower in colorectal cancer patients than in simple adenomas (p = 0.02). VEGF-A levels were directly correlated to polyp size (rho = 0.73, p = 0.0062). Multivariate analysis demonstrated that malignancy and polyp size were independent predictors of VEGF-A mucosal levels. This study demonstrated that the VEGF-A expression changes along the colorectal carcinogenesis pathway showing a neat step up at the passage from high-grade dysplasia to invasive cancer. This feature might potentially be useful to stratify colorectal polyps in different risks of progression classes. Moreover, the high level of VEGF-A expression predicted the presence of lymphovascular invasion with good accuracy.
Introduction
The incidence of colorectal cancer (CRC) in patients undergoing screening protocols is decreasing because of the higher rate of colonic lesion discovered at a preneoplastic stage.1,2 Even though the majority of polyps can be removed endoscopically with different techniques of polypectomy in some cases (due to dimension or site), surgery is still necessary. In these cases, a radical surgical procedure is indicated because a significant percentage of polyps (13%–22%) can be an invasive carcinoma.3–12 In 2012, Jang et al. reviewed a series of patients who underwent colonic resection for polyps that were not considered amenable for endoscopic removal. The rate of malignancy in the group of patients with adenomas was 16%. Moreover, the rate of adenocarcinoma on polyps (with or without dysplasia) varied from 0% to 36%, while the rate of adenocarcinoma on polyps with dysplasia varied from 32% to 60%. 13
However, in most of these polyps, radical surgery can be considered an overtreatment and colonic resection is burdened by a significant complication rate. According to the most recent National Comprehensive Cancer Network (NCCN) guidelines in case of endoscopic removal of polyps with adenocarcinoma foci at histology, clinical follow-up is indicated if the grading is G1 or G2, and there is no angiolymphatic invasion and negative margin of resection. 14 In fact, several endoscopic techniques, such as endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD), can radically remove even polyps of conspicuous dimensions. Furthermore, some hybrid techniques (endoscopic and laparoscopic) have been developed.15–17 However, if at histology, foci of invading carcinoma are present in association with unfavorable risk factors, an oncological resection with proper lymphadenectomy of the involved segment becomes mandatory. Therefore, a correct diagnosis and precise staging of the adenoma/CRC at the moment of the first endoscopy are essential to establish the correct therapeutic strategy.
Vascular endothelial growth factor (VEGF) is an important proangiogenic growth factor and its expression is upregulated by most cancer cell types. The different forms of VEGF bind to transmembrane receptor tyrosine kinases (vascular endothelial growth factor receptors (VEGFRs)) on the cell surface. This results in receptor dimerization, activation, and autophosphorylation of the tyrosine-kinase domain which triggers downstream signaling pathways. A Finnish study found that the VEGF expression was higher in tumors of the left colon and it significantly correlates with disease stage and 10-year survival rate. 18 High levels of VEGF-A in the tumor are considered a marker of unfavorable prognosis and aggressive phenotype. The aim of this study was to assess the VEGF expression in the different steps of colorectal carcinogenesis to explore its potential role as a marker of malignancy in polypoid lesions.
Patients and methods
Study design
This study was performed according to the principles of the Declaration of Helsinki, and all those participating had given their consent to have their data and anonymized specimens used for scientific purposes. The study was notified to the Ethical Committee of the Treviso Regional Hospital. A total of 92 consecutive subjects who underwent colonoscopy for screening or were operated on for colorectal adenoma or CRC at the Gastroenterological and the Surgical Departments of the Treviso Regional Hospital from 2009 to 2010 were enrolled.
Inclusion criteria included the presence of polypoid colorectal lesion at endoscopy or at operation and patients’ consent to participate in the study, and patients were excluded if any kind of neoadjuvant therapy had been administered or if the patients had any synchronous neoplasm. A group of healthy subjects undergoing colonoscopy for screening was enrolled as controls. Setting alpha (probability of type I error) at 0.05, beta (probability of type II error) at 0.20, and an expected effect size of 1, the final minimal sample size for each group was 19 subjects.
Data collection and sample retrieval
Family and medical history were retrieved: in particular, the presence of positive Bethesda criteria, tumor size and stage, tumor site, and preoperative therapy were taken into consideration. Mucosal samples were taken from healthy mucosa of the sigmoid colon in healthy controls or from the top of the polyp in case of adenoma or CRC during colonoscopy of colectomy (in case of large polyps or CRC). Samples were subdivided into two and then stored in formalin 10% and sent for regular pathology assessment or snap frozen at −80°C for molecular biology analysis. Immunohistochemistry (IHC) analysis was performed on paraffin-embedded tumor samples from these patients.
External validation series
A validation analysis was performed on a series from Hungary accessed from the Gene Expression Omnibus (GEO) databank. In this series, data about VEGF-A, VEGF-C, VEGF-R1, VEGF-R2, and VEGF-R3 messenger RNA (mRNA) levels were retrieved from a microarray dataset and compared. Validation series consisted of gene expression data from 96 samples accessed from the GEO databank (dataset ID: GSE37364 19 ). According to the GEO entries, total RNA was extracted from colonic biopsy samples of histologically negative patients (n = 38) and of patients with adenoma (n = 29) or CRC (n = 27) and were hybridized on Affymetrix HG-U133 Plus 2.0 microarrays. Our selected gene panel was tested on the downloaded dataset, and their expression in invasive cancer compared to adenoma was tested with non-parametric Mann–Whitney U test adjusted for multiple comparison (p value < 0.001).
Pathology assessment and IHC
Histology sections (3 µm), obtained from formalin-fixed, paraffin-embedded specimens, were stained with hematoxylin–eosin. CRC staging was classified by a single expert gastrointestinal pathologist (F.C.) using the Vienna classification of gastrointestinal epithelial neoplasia. 20 The tumor infiltrating mononuclear cells (TIMC) infiltration was graded on a semi-quantitative scale (negative, low, moderate, or high). Immunohistochemical analyses were performed using tissue array procedures. The VEGF-A expression was graded on a semi-quantitative scale (negative, low, moderate, or high). Immunocomplexes were detected using an avidin–biotin–peroxidase conjugate and 3-3′diaminobenzidine-tetrahydrochloride chromogen as a substrate (ABC Kit; Vector Laboratories, Burlingame, CA, USA; DAB Kit; Dako, Glostrup, Denmark). The IHC methods and antibodies used were reported in Table 2. Each slide contained a unique number that enabled blinding as for patients’ identity and clinical characteristics. In all, 10 random fields (×63) from each sample were examined.
Quantitative reverse transcription polymerase chain reaction
Total RNA was extracted and purified using an RNeasy Mini Kit (Qiagen, Valencia, CA, USA), and any residual genomic DNA was removed by RNase-Free DNase digestion (Qiagen) according to the manufacturer’s instructions. First-strand complementary DNA (cDNA) was synthesized from 1 µg of total RNA using 50 ng of random hexamers, 40 U RNase Out (Invitrogen, Carlsbad, CA, USA), and 200 U SuperScript™ II (Invitrogen) in a final volume of 20 µL. The reaction was incubated at 25°C for 10 min, at 42°C for 50 min, and at 70°C for 15 min. Primers and TaqMan probes for quantitative reverse transcription polymerase chain reaction (RT-PCR) were designed using the Primer Express™ software (version 3.0; Applied Biosystems, Foster City, CA, USA). Sequences of primers and probes are reported in Table 1. Standard curves were generated from decreasing amounts of cDNA diluted at two-fold intervals to evaluate the efficiency of real-time RT-PCR. The quality of each real-time assay can be evaluated from standard curve slopes and correlation coefficients (r). Intra-assay precision (among triplicates over standard curve molecular range) and inter-assay reproducibility (among three runs) were also evaluated as coefficient of variation (% CV). Quantification of VEGF-A mRNA was carried out in StepOnePlus™ Real-Time PCR System (Applied Biosystems) programmed for an initial step of 2 min at 50°C and 5 min at 95°C, followed by 45 cycles of 15 s at 95°C and 1 min at 60°C. The PCR reactions were carried out in a 20 µL reaction volume with TaqMan® Gene Expression Master Mix (Applied Biosystems) with optimized concentrations of specific primers and 2 µL of cDNA. Each plate included triplicate of the calibrator cDNA, test cDNA samples, and no template controls. Relative quantification of gene expression was made by means of StepOne Software v2.3 (Applied Biosystems) according to the comparative threshold cycle (Ct) method, 21 using a mixture of RNAs from normal tissue as calibrator. RPLP0 gene was used as endogenous reference.
Sequences of primers and probes.

Immunoassays
Tissues were mechanically homogenized in 500 µL of phosphate-buffered saline (PBS) (1:10 wt/vol ratio) containing a protease inhibitor cocktail (Roche Applied Science, Penzberg, Upper Bavaria, Germany). Protein concentration was determined using the bicinchoninic acid (BCA) Protein Assay kit (Pierce, Rockford, IL, USA). Mucosal levels of VEGF-A, VEGF-C, VEGF-R1, VEGF-R2, and VEGF-R3 were measured by immunometric assay according to the manufacturer’s instructions. Data are expressed in picogram per microgram of total proteins.
Statistical analysis
Statistical analyses were carried out with STATISTICA 5.1 software, StatSoft, Tulsa, OK, USA. The results are presented as mean ± standard error of mean (SEM) unless otherwise specified. Non-parametric Mann–Whitney U test for independent variables or Kruskal–Wallis analysis of variance (ANOVA) for multiple variables was used for comparison as appropriate. Kendall’s correlation test was used to assess the association between variables. Receiver operating characteristic (ROC) curve analysis was performed to assess the accuracy of the VEGF-A levels as predictor of malignancy and of lymph vascular invasion. Statistical significance was set at p < 0.05 unless otherwise specified.
Results
Patients’ characteristics
We enrolled 92 subjects in this prospective study: 19 of them were healthy subjects who underwent negative colonoscopy for screening; 34 subjects had colorectal adenoma, and 39 had invasive adenocarcinoma. Of them, 60 subjects were male and their median age was 77 (65–82.5) years. Of the group, 10 patients who underwent surgery had a colonic lesion that was not considered amenable for endoscopic removal. None of these patients had neoadjuvant therapy. Patients’ characteristics are shown in Table 2.
Patients’ characteristics.

LGD: low-grade dysplasia; HGD: high-grade dysplasia.
VEGF-A expression along the colonic carcinogenesis pathway
As shown in Figure 1(a), VEGF-A mRNA expression resulted to be higher in invasive carcinomas (p = 0.01). Similarly, at IHC, the VEGF-A protein expression was significantly higher in patients with adenocarcinoma than in those with adenoma or in healthy subjects (p < 0.001; Figure 1(b)). The VEGF-A expression along the different steps of the carcinogenesis is shown in Figure 1(c).

(a) VEGF-A mRNA and (b) protein expression at different stages of tumoral progression. (c) VEGF-A staining in different steps of carcinogenesis.
As shown in Figure 2(a) and (b), in polypoid lesions, both VEGF-A mRNA and protein expression at IHC were significantly higher in CRC than in adenomas (p = 0.02 and p < 0.0001, respectively). On the contrary, VEGF-A levels at immunoassay were not different between CRC and adenomas as well as VEGF-R1, VEGF-R2, and VEGF-R3 mucosal levels. The specificity of the VEGF-A protein for the diagnosis of adenocarcinoma in colonic polypoid lesions (with a threshold of 2+) was 100% (confidence interval (CI) = 87.9–100), sensibility was 66.67% (CI = 34.9–89.9), and the overall accuracy was 91.7 (CI = 78.7–97.9). On the other hand, the overall accuracy of VEGF-A mRNA for the diagnosis of adenocarcinoma in colonic polypoid lesions (with a threshold of 1.7461) was 72.2% (CI = 56.9–84.5); the sensitivity was 58.33% (CI = 27.8–84.7) and the specificity was 84.85% (CI = 68.1–94.8).
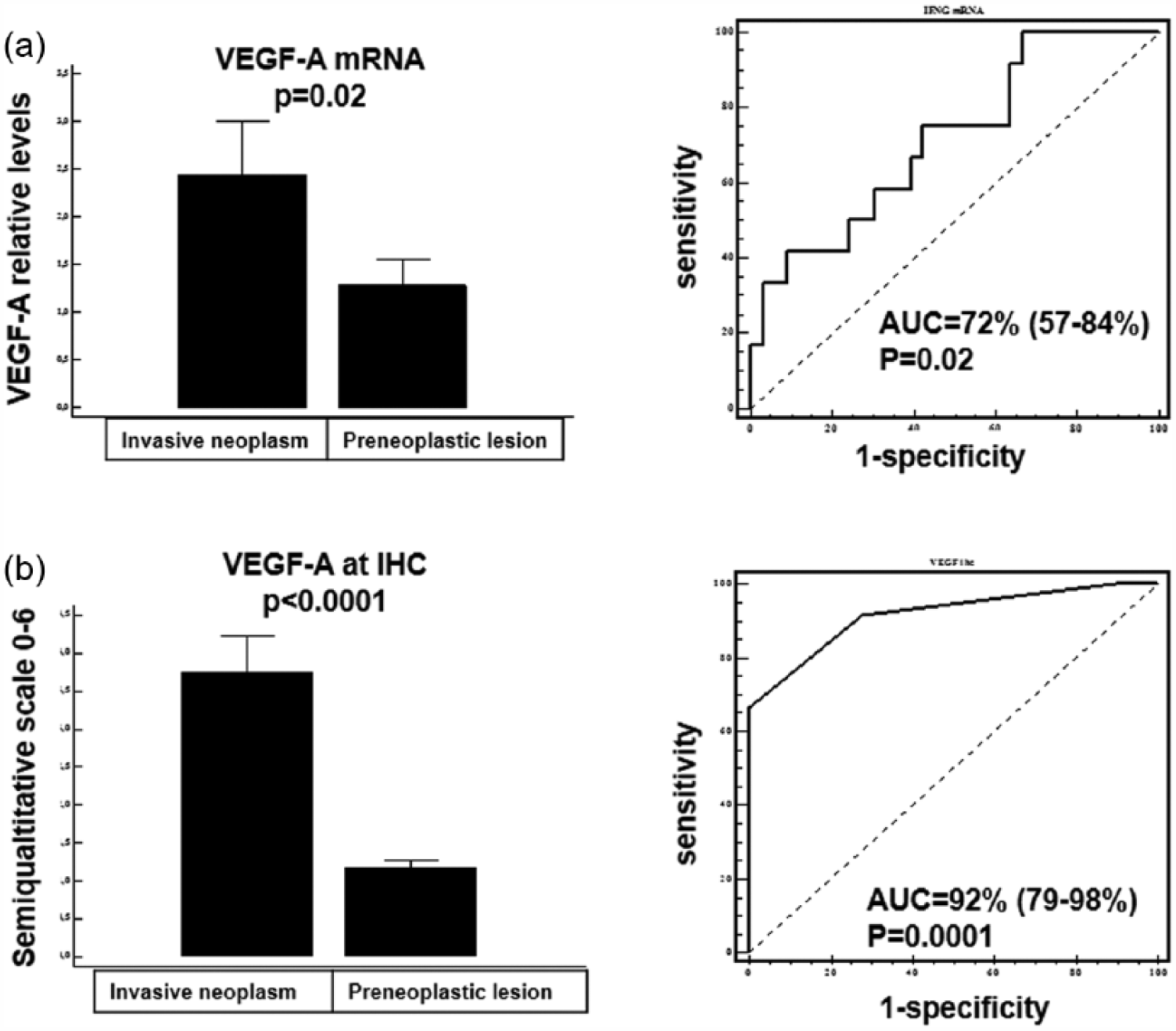
VEGF-A as predictor of malignancy in colonic polypoid lesion. (a) VEGF-A mRNA expression in invasive neoplasm and preneoplastic lesions and its accuracy (ROC curve) in predicting malignancy in polipoid colonic lesions. (b) VEGF-A protein expression as detected by immunohistochemistryin invasive neoplasm and preneoplastic lesions and its accuracy (ROC curve) in predicting malignancy in polipoid colonic lesions.
As shown in Figure 3, the external validation of the analysis of the mRNA expression of VEGF gene family as predictors of malignancy in colonic polypoid lesions on the GSE36374 dataset showed that VEGF-A, VEGF-C, and VEGF-R1 mRNA levels were significantly higher in patients with malignant polypoid lesion (MPL) than in those with just preneoplastic lesion (PNL) (p < 0.001, p = 0.001, and p = 0.001, respectively). The ROC curve analysis on the GSE36374 dataset showed a good accuracy for the three markers (area under the curve (AUC) = 85%, AUC = 81%, and AUC = 80%, respectively).
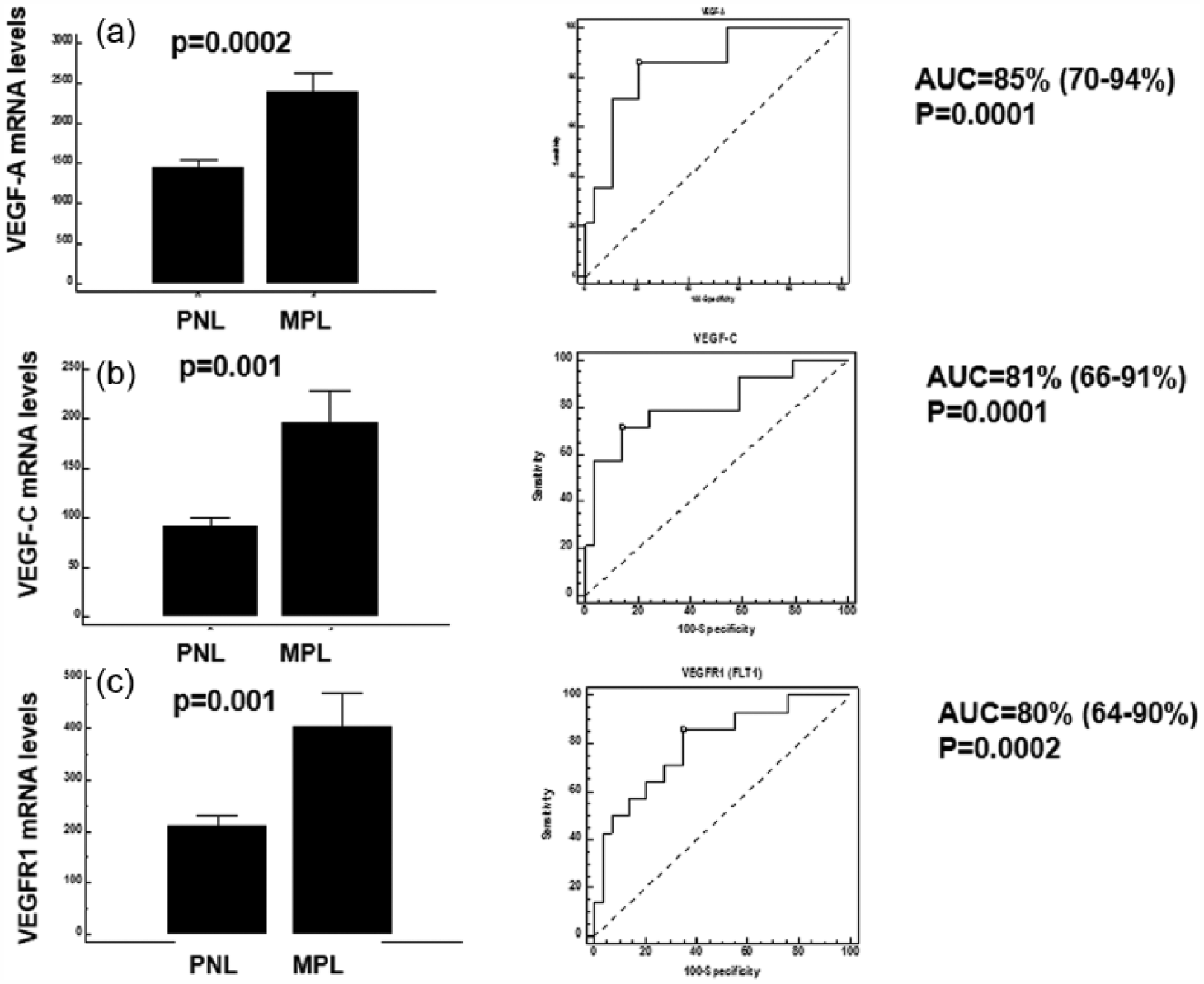
VEGF genes family mRNA expression as predictors of malignancy in colonic polypoid lesions in GSE36374 dataset: validation analysis. (a) VEGF-A mRNA expression in invasive neoplasm and preneoplastic lesions and its accuracy (ROC curve) in predicting malignancy in polipoid colonic lesions. (b) VEGF-C mRNA expression in invasive neoplasm and preneoplastic lesions and its accuracy (ROC curve) in predicting malignancy in polipoid colonic lesions. (c) VEGFR1 mRNA expression in invasive neoplasm and preneoplastic lesions and its accuracy (ROC curve) in predicting malignancy in polipoid colonic lesions.
VEGFs and CRC staging
In colorectal adenocarcinoma, VEGF-A levels at IHC were significantly correlated to T stage (rho = 0.31, p = 0.04). No statistical significant difference in the expression of VEGF-A mRNA and protein was observed between patients with or without lymph node involvement and among different cancer stages. Moreover, as shown in Figure 4(a), VEGF-A levels at immunoassay were significantly higher in adenocarcinoma with lymphovascular invasion compared with those without lymphovascular invasion (p = 0.01). High levels of VEGF-A expression predicted the presence of lymphovascular invasion with good accuracy (AUC = 72% (56–85%), p = 0.004). On the other hand, as shown in Figure 4(b), adenocarcinoma with lymphovascular invasion had lower VEGF-C levels than those without invasion (p = 0.01) and low levels of VEGF-C predicted the presence of lymphovascular invasion with good accuracy (AUC = 74% (58%–86%), p = 0.004).

Levels of VEGF-A and VEGF-C secreted proteins within the tumor as predictors of lymphovascular invasion . (a) VEGF-A in lesions with lymphovascular invasion or not and its accuracy (ROC curve) in predicting lymphovascular invasion in polipoid colonic lesions. (b) VEGF-C in lesions with lymphovascular invasion or not and its accuracy (ROC curve) in predicting lymphovascular invasion in polipoid colonic lesions.
VEGFs and adenoma features
As shown in Figure 5, VEGF-A at IHC was significantly lower in patients with multiple adenoma than in patients with single adenoma (p = 0.02). On the contrary, VEGF-A mRNA was not significantly different in the two situations (p = 0.74). Moreover, VEGF-A levels at IHC and VEGF-A mRNA levels were significantly correlated to maximum diameter of the lesion (rho = 0.73, p = 0.006 and rho = 0.25, p = 0.02, respectively).

VEGF-A levels at IHC predict multiple adenoma and correlate with polyp size. (a) VEGF-A in multiple and single colonic lesions and its accuracy (ROC curve) in predicting multiple polipoid colonic lesions. (b) VEGF-A correlation with polipoid colonic lesions main diameter.
Discussion
CRC represents the second cause of death in Western countries and its incidence is rising all over the world. 1 Screening programs have reduced the mortality rates for CRC in Italy by finding lesions at initial stages or by directly treating precancerous lesions during colonoscopy.1,22 Although NCCN guidelines state that clinical follow-up is recommended in case of endoscopic removal of polyps with adenocarcinoma at histology with favorable prognostic factors, in the other cases, a proper oncological resection with adequate margins and lymphadenectomy remain mandatory. 14 However, the preoperative diagnosis is still difficult in case of polyps that cannot be removed endoscopically and in which biopsies can potentially miss possible sites of invasion and malignancy. In fact, in a recent review of series of patients undergoing surgical resection for colorectal polyps that were not amenable to endoscopic removal, the malignancy rate varied from 0% to 60%.22–26 Indeed, endoscopy with histological examination of biopsies that do not include the entire lesion is limited in the distinction between benign and malignant polyps. For this reason, in recent years, some more sophisticated endoscopic techniques, such as confocal laser endomicroscopy, have been proposed to improve diagnostic accuracy. Therefore, the aim of this study was to assess the VEGF expression in the different steps of colorectal carcinogenesis to explore its potential role as a marker of malignancy in polypoid lesions.
In our series, VEGF-A mRNA and VEGF-A protein expression resulted to be higher in invasive carcinoma. VEGF-A is one of the principal cytokines involved in tumoral progression because of its antiapoptotic role on neoplastic cells and its regulation of tumoral neoangiogenesis by stimulating the vessels growth. The tumor is initially an avascular mass that draws from the surrounding microenvironment of the maintenance and blood supply; however, when the dimensions reach approximately 4 mm, the development of its own blood supply becomes necessary. 27 This critical point is called angiogenic switch, which is a characteristic of the malignant lesion and allows its progression. 28 Our data clearly showed the switch of the VEGF-A expression in the passage from high-grade dysplasia (HGD) to invasive cancer. And this switch might be translated into a clinical application. In fact, in polypoid lesions, both VEGF-A mRNA and protein expression at IHC were significantly higher in CRC than in adenomas. The specificity of the VEGF-A protein for the diagnosis of adenocarcinoma in colonic polypoid lesions was 100% (CI = 87.9–100) and sensibility was 66.67% (CI = 34.9–89.9) with an overall accuracy of 91.7 (CI = 78.7–97.9). Moreover, these data are supported by those obtained from the external validation on the GSE36374 dataset. 19 In this dataset, VEGF-A mRNA levels predicted the malignancy in polypoid lesions with an overall accuracy of 85%. Taken into consideration together, these data confirm what observed by Staton et al. 29 who demonstrated the angiogenic switch in the passage from adenoma to CRC, and they can lay the basis for the use of VEGF-A as to stratify colorectal polyps in different risks of progression classes.
Several studies have evaluated the prognostic value of the VEGF-A expression in CRC,30–34 and a recent meta-analysis concluded that the VEGF-A expression is a negative prognostic factor in CRC. 35 In our series, in patients with CRC, VEGF-A levels at IHC were significantly correlated to T stage. Similarly, Hanrahan et al. 36 observed that VEGF-A mRNA correlated with the grade and dimensions of the tumor and in a Finnish series it correlated with T stage. 37 In fact, the VEGF expression was described to be increased in the center of the neoplastic mass and progressively reduced approaching the borders with an intensity that finds its apex in the first 5–10 cm around the tumor. 38 However, Hanrahan et al. 36 observed that VEGF-A mRNA did not correlate with vascular and lymphatic invasion, while in our series VEGF-A levels at immunoassay were significantly higher in adenocarcinoma with lymphovascular invasion compared with those without it, and low levels of VEGF-C predicted the presence of lymphovascular invasion. The discrepancy between the two observations may be due to the different transcriptional stages of the two observations (our mRNA VEGF-A data also did not correlate with lymphovascular invasion). Nevertheless, since lymphovascular invasion is a well-known negative prognostic factor, as stated by the NCCN guidelines, 14 VEGF-A levels at immunoassay might be potentially useful to stage the disease.
In our series of patients with adenoma, VEGF-A at IHC was significantly lower in patients with multiple adenoma compared to those with single adenoma. These data might be useful when observing an unexpectedly low VEGF-A level at IHC (i.e. in a large polypoid lesion). The suspect that should arise is that there is more than one polypoid lesion. However, this could only be an interesting observation and larger series should be observed to draw definitive conclusions.
In conclusion, this study demonstrated that the VEGF-A expression changes along the colorectal carcinogenesis pathway showing a neat step up at the passage from HGD to invasive cancer. This feature might potentially be useful to stratify colorectal polyps in different risks of progression classes. Moreover, high levels of the VEGF-A expression predicted the presence of lymphovascular invasion with good accuracy.
Footnotes
Acknowledgements
The authors are grateful to Dr Ida Ruffolo, PhD, for her assistance in editing the final version of this manuscript. This article was accepted for oral presentation at the UEG Week 2015 in Barcelona, Spain.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by current research funds from the University of Padova to Prof. Nicolò Bassi and from the Italian Ministry of Health to Dr. Carlo Castoro.