
Abstract
Background
Patients with acute promyelocytic leukemia (APML) undergoing induction therapy are severely immunocompromised and prone to opportunistic infections. Tuberculosis (TB), though less commonly considered, can complicate the clinical course, particularly in endemic regions.
Purpose
To emphasize the need to consider extrapulmonary TB in APML patients with persistent fever and non-resolving pleuro-pulmonary abnormalities.
Materials and Methods
An APML patient receiving arsenic trioxide (ATO) and all-trans retinoic acid (ATRA) developed persistent high-grade fever. High-resolution computed tomography (HRCT) and microbiological evaluation were performed. TB DNA was detected from mediastinal lymph nodes. Due to hepatic and renal dysfunction, a modified anti-tubercular treatment (ATT) regimen was initiated. Serial HRCT scans from February 17 to February 25, 2025 were used for follow-up.
Results
Initial HRCT revealed right pleural effusion, adjacent lung collapse, bilateral centrilobular nodules, and mediastinal lymphadenopathy. Follow-up imaging showed marked reduction in pleural effusion with persistent pleural thickening and minimal residual air near the drain site, suggesting an ongoing infectious process. The patient demonstrated clinical improvement with continued modified ATT and APML-directed therapy.
Conclusion
Persistent pleural thickening despite decreasing effusion in immunocompromised APML patients should raise suspicion of tuberculosis. Early microbiological confirmation, serial imaging, and multidisciplinary management are crucial for timely diagnosis and favorable outcomes, particularly in TB-endemic settings.
Keywords
Introduction
Acute promyelocytic leukemia (APML) is a well-characterized subtype of acute myeloid leukemia (AML) with defined treatment protocols involving all-trans retinoic acid (ATRA) and arsenic trioxide (ATO). However, the management of APML complicated by concomitant infectious diseases such as tuberculosis (TB), especially with extrapulmonary involvement and pleural effusions, remains poorly described. Limited reports highlight the challenges in diagnosis, tailored treatment adjustment due to organ dysfunction, and the interpretation of evolving radiological findings in such cases. 1 This case emphasizes the need for increased awareness and integrated, multidisciplinary approaches to optimize outcomes in APML patients with systemic infectious complications, addressing a gap in existing literature. 2 Clinically, patients with disseminated intravascular coagulation (DIC), a hallmark characteristic of APML, present with bleeding tendencies; this calls for the quick commencement of treatment.3, 4 Patients are still susceptible to problems notwithstanding these therapeutic benefits, especially pulmonary problems brought on by leukemic infiltration, secondary infections, or differentiation treatment-related capillary leak syndromes like retinoic acid syndrome.5–7 Notable causes of pleural effusion in AML include direct leukemic infiltration, overlapping infections like TB, or therapy-induced vascular permeability changes.8, 9 The patient also developed differentiation syndrome, and distinguishing the cause of pleural effusions depends critically on high-resolution computed tomography (HRCT) and serial radiographic monitoring, which helps to identify accompanying radiologic features, including pleural thickening, ground glass opacities, and lymphadenopathy. 10 The case highlights the need for serial imaging in directing therapy, especially when complications result from both the disease process and opportunistic infections.11, 12
Methodology
Patient data are derived from medical records at Believers Church Medical College Hospital (November 2024–February 2025), along with written informed consent. Institutional ethical approval is obtained. The literature search was conducted using PubMed, Scopus, and Web of Science. On follow-up imaging, compared to the previous measurement of 6.5 × 9.5 × 16.6 cm, the most recent scan showed a significant interval reduction in the right-sided pleural effusion to 2.8 × 6.8 × 14.1 cm, with persistent parietal pleural thickening. The patient’s identity is protected as per the guidelines.
Case Presentation
A 43-year-old male patient diagnosed with APML was admitted for induction phase chemotherapy and later developed high-grade fever spikes. His blood cultures were negative. Even on high-end antibiotics, he persistently developed fever spikes. The patient’s abnormal liver function tests (LFTs) most likely included elevated bilirubin, which caused hyperbilirubinemia and suggested acute hepatitis and liver inflammation, and elevated transaminases (alanine aminotransferase (ALT) and aspartate aminotransferase (AST)), which indicated transaminitis. Imaging revealed periportal and gallbladder wall edema, which supported liver dysfunction. Acute kidney injury (AKI) stage Kidney Disease: Improving Global Outcomes (KDIGO) 3 due to contrast-induced nephropathy was indicated by elevated serum creatinine and decreased urine output in the renal function tests (RFTs), which required dialysis. Drug dosages were adjusted based on creatinine clearance. Bronchoscopy was done, which was negative for any infectious status. A multidisciplinary team initiated a modified anti-tubercular treatment (ATT) regimen, adjusted for liver and renal dysfunction. The patient developed bilateral pleural effusion with bacterial sepsis, managed successfully with intravenous antibiotics and intercostal drain (ICD) insertion. He improved clinically and was discharged. On follow-up, the patient had no respiratory symptoms, and physical examination was mostly normal, except for reduced air entry in the right lower lung. Laboratory tests showed no ongoing infection, and he was clinically stable. Sequential chest CT scans showed obvious changes in pleural pathology. Compared to the prior 6.5 × 9.5 × 16.6 cm, the most recent scan revealed a noteworthy interval reduction in right-sided pleural effusion, currently measuring 2.8 × 6.8 × 14.1 cm, together with constant parietal pleural thickening. Moreover, tiny non-dependent air bubbles were noticed surrounding the previously installed drain tube. The septal thickening at the bilateral apices had completely vanished once it came out; ground glass opacities in the left lower lobe showed some resolution. There was neither new lymphadenopathy nor skeletal abnormalities noted. Considering the persistent pleural thickening despite radiological improvement and a stable clinical state, a more in-depth multidisciplinary assessment was begun. Subsequent microbiological examinations confirmed the presence of Mycobacterium tuberculosis, indicating that the patient had acquired TB after his initial APML diagnosis. This underscores the susceptibility of immunocompromised people to secondary illnesses and the need for ongoing monitoring even in clinically stable individuals.
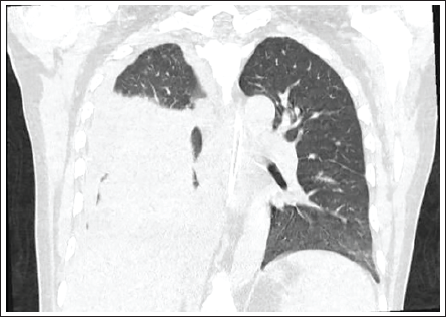
A 43-year-old man with a known APML case and bilateral pleural effusion, mainly on the right, shows a moderate right pleural effusion with neighboring on his HRCT chest scan dated November 4, 2024, which appears steady, with lung collapsed consolidation. The hyperdense areas inside the effusion have shrunk in both density and size relative to the earlier October 21, 2024, scan. There is a nearly complete collapse of the right lower lobe that remains stable, in addition to subsegmental atelectasis impacting the left lower lobe lateral and posterior basal segments. Though there are a few scattered centrilobular nodules in the bilateral lung parenchyma, they have reduced dramatically from the prior scan. Not seen proof of mass, honeycombing, interstitial thickening, fibrosis, bronchiectasis, or pleural thickening. The trachea and main bronchi appear to be normal in caliber and lumen; the heart appears normal, with no pericardial effusion. Stable markers of mediastinal lymphadenopathy are a dilated primary pulmonary artery (31 mm) and several paraaortic and right paratracheal nodes, with the biggest 13–15 mm short axis diameter (SAD). Normal chest wall and bony thorax; preservation of mediastinal fat planes; no esophageal dilation; a splenunculus was also found.
The CT scan findings before treatment are shown in Figure 1.
Patient Clinical Events Timeline. 8
Follow-up CT scan findings after treatment are shown in Figure 2.
Chronology of Clinical Events. 8

Bronchoscopy was done, which was negative for any infective status. Bone marrow aspiration showing aberrant promyelocytes, and cytogenetic verification of the distinctive t (15;17) (q24;q21) translocation creating the promyelocytic leukemia/retinoic acid receptor alpha (PML-RARA) fusion gene, established his diagnosis. Standard treatment using ATO in addition to ATRA was started; he reacted with a good hematologic remission. Nevertheless, parietal pleural thickening persisted, therefore increasing the chance of arranging pleuritis or chronic fibrotic alterations caused by previous inflammation. Other than modest age-related degenerative changes, the mediastinal vessels, trachea, bronchial tree, and bones of the chest wall and spine were unremarkable. Clinically, the patient maintained afebrile and said that they had no respiratory symptoms, including coughing, dyspnea, or chest pain. Though otherwise within acceptable bounds, the physical examination found reduced breath sounds over the right lower lung area, possibly matching the residual pleural thickening. Specific microbiological and molecular tests—including sputum analysis and pleural revealed M. tuberculosis thereafter, fluid GeneXpert confirmed that the patient had acquired pulmonary TB as a second result during the leukemia treatment.
Given his immunocompromised state brought on by both the disease and its treatment, which increases vulnerability to opportunistic infections like TB, this diagnosis was particularly pertinent. Not only to evaluate disease remission and therapy response, but also to identify secondary effects such as TB, serial imaging in APML is highlighted in this case.
Baseline demographic characteristics of the patient are presented in Table 1.
Therapeutic Agents Used in the Management of Polycythaemia Vera.51
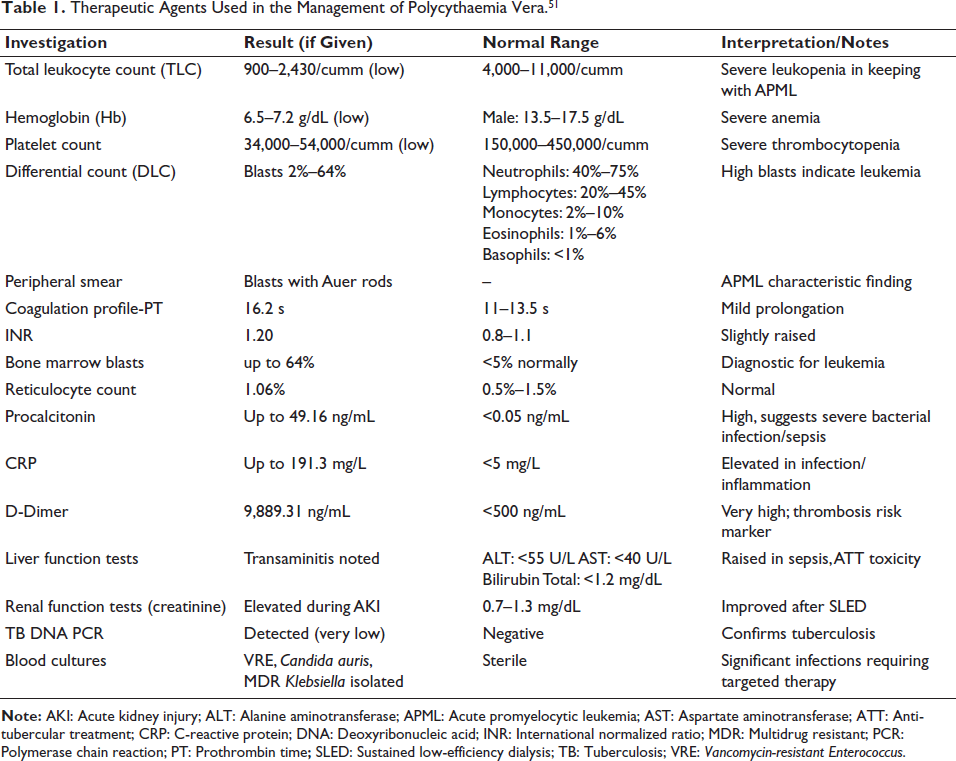
The patient presented with severe pancytopenia, with total leukocyte counts ranging from 900 to 2,430/cumm (severe leukopenia), hemoglobin 6.5–7.2 g/dL (severe anemia), and platelet counts of 34,000–54,000/cumm (severe thrombocytopenia). Peripheral smear showed 20%–64% blasts with Auer rods, consistent with APML. Prothrombin time of 16.2 s and INR of 1.20 suggested early coagulopathy. Bone marrow biopsy showed leukemia with 64% blasts. Elevated procalcitonin up to 49.16 ng/mL and C-reactive protein (CRP) up to 191.3 mg/L suggested a severe bacterial infection or sepsis. A highly elevated D-dimer up to 9,889.31 ng/mL suggested a risk for thrombosis or DIC. Transaminitis in LFTs suggested possible sepsis-related liver injury or anti-tubercular drug toxicity. AKI was corrected with sustained low-efficiency dialysis (SLED). TB deoxyribonucleic acid (DNA) polymerase chain reaction (PCR) was positive. Blood cultures revealed the presence of Vancomycin-resistant Enterococcus, Candida auris, and multidrug-resistant Klebsiella. This is all indicative of severe sepsis, coagulopathy, organ failure, multidrug-resistant infections, and critical illness in the setting of APML, requiring urgent multidisciplinary intervention.
Prospective Complications
Diagnosed with APML, the patient, who next acquired TB with resolving pleural effusion, is in danger of a number of severe repercussions. One of the most frightening outcomes is ongoing pleural thickening and fibrosis, which could impair pulmonary mechanics and cause restrictive lung disease. This structural change can cause chronic breathlessness and limit exercise ability, especially when pleural adhesions induce trapped lung and thereby inhibit full re-expansion of the injured hemithorax. 13 Pharmacological interactions present yet another major hazard under these circumstances. Being a potent inducer of cytochrome P450 enzymes, rifampicin accelerates the metabolism of ATRA, therefore becoming a key component of ATT. Hence, ATRA and ATO reduce their therapeutic efficacy in APML therapy.14, 15 Subtherapeutic levels could also increase the risk of partial remission or disease reappearance. Furthermore, the likelihood of hepatotoxicity and liver damage is enhanced by overlapping toxicities between TB drugs and APML therapy, particularly with isoniazid, pyrazinamide, and arsenic compounds. The dual load of leukemia and TB greatly lowers immunological capability, hence making the patient more susceptible to secondary illnesses, including invasive fungal infections, like viral reactivations, as well as candidiasis or aspergillosis.16–18 These opportunistic infections might influence the clinical path and demand prolonged or thorough antibiotic treatment. Another possible issue is TB reactivation, especially in the setting of chronic immunosuppression.19–22 Even after a clear microbiological cure, residual bacilli can stay latent and be reactivated, therefore leading to recurrent sickness or disseminated forms like miliary TB or TB meningitis.23, 24 From a diagnostic angle, differentiating radiologic features of TB from leukemic infiltrates or drug-induced inflammatory responses presents an inherent challenge. Wrong interpretation of imaging data may cause delays in the appropriate therapeutic treatment or, in some situations, needless changes to the leukemia treatment plan.25–29 Moreover, the prolonged course of the disease and the load of treatment can worsen severe nutritional deficits, especially when combined with the metabolic requirements of both TB and cancer. The catabolic state that follows could compromise the patient’s functional status and tolerance to intensive treatment.30–33 At last, should anti-leukemic treatment be delayed or dose reduced as a result of TB control or toxicity problems, there is an actual chance of APML return. Given that APML is curable with proper adherence to therapy, any deviation in protocol caused by drug interactions, toxicity, or coinfections may jeopardize long-term outcomes.34, 35
Future Direction
Continuous multidisciplinary care is essential for managing APML complicated by pleural effusion and TB. Between November 2024 and February 2025, serial CT scans showed partial right lung re-expansion and near-complete resolution of the effusion. The patient remained in remission with normal blood counts, an afebrile status, and undetectable TB DNA, indicating microbiological cure. Despite residual pleural thickening, pulmonary function and quality of life were stable, highlighting the value of early, integrated follow-up. Predictive biomarkers are also needed to distinguish APML relapse from inflammatory lung changes, with minimal residual disease best detected through PML-RARA transcript monitoring. 36 Further research on TB-leukemia immune interactions could inform new immunotherapies or vaccine strategies for immunocompromised patients. 37 Comprehensive care should also include nutritional, psychological, and fatigue management, as sarcopenia and cachexia remain overlooked yet significant factors in poor outcomes.38–40
Review of Literature
Although they are still uncommon and difficult to treat, similar cases of APML complicated by TB have been documented. According to Yang et al., carrimycin and dose-modified ATT administered concurrently with chemotherapy were used to successfully treat APML and pulmonary TB, leading to complete remission of both conditions. 41 A variant of APML coexisting with TB was reported by Palta et al., bringing to light the difficulties in diagnosis and treatment that call for specialized care. 42 Effective treatment of disseminated pulmonary TB complicating leukemia during induction chemotherapy without chemotherapy interruption was demonstrated in a pediatric case. 43 Wang et al. described a rare case of AML with a leukemic pleural effusion and elevated pleural adenosine deaminase levels, highlighting the diagnostic difficulties in differentiating between effusions related to leukemia and TB. 44
Recommendations for Therapy
Management for this patient has to stay risk-adapted, balancing remission maintenance for APML with complete microbiological and radiological clearance of TB. Low-to intermediate-risk APML therapy still centers on ATRA and ATO; nonetheless, monitoring for hepatotoxicity and QT interval (QT) prolongation becomes vital in the existence of concurrent ATT. 1
Discussion
Emerging data support the use of liposomal ATO in relapsed or refractory APML cases, which may offer a more favorable safety profile and pharmacokinetics, though its role in coinfection scenarios remains under investigation. 45 Extended ATT for the pulmonary features may be justified if follow-up imaging reveals evidence of chronicity or partial resolution of pleural illness. Though their use must be balanced against immunosuppressive risks in a leukemic context, adding corticosteroids may be thought of in cases of organizing pleuritis with major functional impairment. 46 Anti-fibrotic agents like pirfenidone or nintedanib have shown efficacy in idiopathic pulmonary fibrosis and are currently under investigation in post-TB fibrotic lung disease; their compassionate use in severe pleural fibrosis following TB in oncology patients could be a future consideration pending supportive trial results. 47 If pleural thickening advances to symptomatic fibrothorax, interventional pulmonology advice can be necessary; treatments such as decortication or chemical pleurodesis may give symptomatic relief and functional improvement.
Preserving lung function also demands close thought of incentive spirometry and structured pulmonary rehabilitation. Especially drug–drug interactions between rifampicin and ATRA or azoles used for anti-fungal prevention need careful attention. 48 Regular molecular remission monitoring, psychological therapy, dietary changes, and reentry into daily life, at last, should guide planning for long-term survival. A collaborative approach between hematologists, pulmonologists, infectious disease experts, and rehabilitation therapists ensured comprehensive care and a lower risk of fragmented treatment in difficult circumstances like this. 49
Conclusion
The management of APML in the presence of pleural effusion and TB is complicated, as this case illustrates. Combining ATO and ATRA therapy resulted in complete hematologic and molecular remission for the patient, while a modified anti-tubercular regimen controlled TB without causing significant hepatic or renal toxicity. A follow-up from November 2024 to February 2025 revealed stable remission, undetectable TB DNA, and a noticeable radiologic resolution of the pleural effusion. Continuous monitoring and pulmonary physical therapy were necessary due to persistent pleural thickening. Patients with APML and concurrent TB can achieve good functional recovery and long-lasting remission when multidisciplinary collaboration is used to manage their condition, balancing anti-leukemic therapy, infection control, and functional rehabilitation. According to new research, this case emphasizes the need for careful follow-up, molecular monitoring, and customized treatment planning in order to maintain remission and quality of life in intricate coinfection situations. 50
Footnotes
Abbreviations
AKI
Acknowledgments
The authors express their gratitude to the patients and their family members and to the Believers Church Medical College Hospital for granting consent to utilize their valuable medical records for case reporting.
Authors Contribution
Chepsy C. Philip, Bobby Abraham, Sreehari, and Aakash Chozakade contributed to data collection, literature review, and drafting of the manuscript. Paul Mathi Vathana Karunagaran assisted in pharmacotherapy analysis, manuscript editing, and preparation of clinical summaries. Edlin Domini Thakkekara conceptualized the case report, supervised the work, and critically revised the final manuscript.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval was obtained from the Institutional Ethics Committee, and informed consent was taken from the patient prior to inclusion in the study and publication of clinical details.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.