
Abstract
Background
Chronic diseases present a significant health risk, and global medication adherence for these conditions remains insufficient. Understanding the factors that affect adherence is essential.
Purpose
This study aims to better understand medication adherence and the factors influencing non-adherence in Saudi Arabia.
Materials and Methods
A questionnaire-based survey was carried out among patients with chronic diseases in the Makkah region of Saudi Arabia from May 1 to August 31, 2024. Participants included individuals aged 18 and older using either prescribed or over-the-counter (OTC) medications. Descriptive statistics were employed to outline the participants’ characteristics, with categorical variables presented as frequencies and percentages. A chi-square test was utilized to examine the relationships between variables.
Results
In total, 292 participants were included in this study. Their ages ranged from 18 to more than 50 years, with a mean age of 38.4 ± 12.5 years old and most of them (72.6%) were female. For chronic diseases, the most reported were hypertension (HTN) (28.8%), diabetes (22.6%), and dyslipidemia (22.3%). The majority of patients (77.7%) were taking 1–3 medications daily, 13.5% were taking 4–6 drugs, and 3.8% were taking 7–9 medications. Medication adherence was significantly associated with informed medical instruction (p < .01), family and friend support (p < .01), and the number of drugs received daily (p < .004).
Conclusion
Focusing on factors such as clear medical instructions, social support, and the number of medications prescribed could boost medication adherence and lead to better health outcomes for patients with chronic diseases in Saudi Arabia.
Introduction
Medication adherence plays a vital role in managing chronic diseases, significantly influencing health outcomes, quality of life, and overall healthcare expenses. 1 In Saudi Arabia, the increasing prevalence of chronic conditions such as diabetes, hypertension (HTN), and cardiovascular diseases underscores the necessity of understanding and improving medication adherence. Research reveals that many patients do not follow their prescribed medication regimens, resulting in adverse health effects and escalating healthcare costs.2, 3
Chronic diseases pose a significant challenge in Saudi Arabia, particularly diabetes, which is a leading health concern. 4 The International Diabetes Federation estimates that around 4 million adults in the country are affected by diabetes, with projections indicating a further increase. HTN and cardiovascular diseases also contribute to high morbidity and mortality rates. 5 Managing these conditions typically requires long-term adherence to medication, which can be difficult for many patients to maintain. 6 Multiple factors influence medication adherence in Saudi Arabia. Among the patient-related factors, psychological issues such as depression and anxiety were prevalent and could impede motivation and the ability to adhere to complex treatment plans. Furthermore, health literacy is critical; many patients may not fully understand their conditions or the significance of following their prescribed treatments.4, 6
Cultural beliefs and attitudes toward medications also played a role in adherence. Patients may express concerns about potential side effects or harbor doubts about the necessity of certain treatments. 5 Additionally, the social environment, particularly familial support, can either promote or hinder adherence. In Saudi culture, strong family ties can be beneficial, but they may also create dependence on family members for medication management, which can occasionally be counterproductive. 7
Healthcare system factors further complicate adherence challenges. Access to healthcare services can be limited, especially for those in rural areas, where obtaining medications and securing follow-up care may be difficult. 8 Effective communication between healthcare providers and patients fosters understanding and cooperation regarding treatment plans. 9 Therefore, addressing these barriers is essential for improving medication adherence. Non-adherence to medication regimens can lead to serious health repercussions in Saudi Arabia. 10 Patients may suffer from uncontrolled diseases, resulting in increased complications and higher hospitalization rates. 11 This affects the individuals and places a significant financial strain on the healthcare system, with estimates indicating that non-adherence costs millions annually due to avoidable hospitalizations and additional treatments.10, 12
To enhance medication adherence among patients with chronic diseases in Saudi Arabia, a comprehensive approach is necessary. 13 Patient education is essential; providing clear and accessible information about chronic conditions and the importance of adherence empowers patients to take charge of their health. 8 Additionally, leveraging technology, such as mobile reminders and medication tracking applications, can significantly improve adherence rates. Improving communication between healthcare providers and patients is also critical.10, 14 Training healthcare professionals to involve patients in shared decision-making can enhance understanding and commitment to treatment plans. 15 Moreover, addressing financial obstacles through patient assistance programs and advocating for the use of generic medications can help mitigate some of the challenges patients face. 16
Ultimately, improving medication adherence among patients with chronic diseases in Saudi Arabia involves a thorough understanding of the factors affecting adherence and the implementation of targeted interventions. 17 By prioritizing education, enhancing communication, and providing robust support, healthcare providers can boost adherence rates, leading to better health outcomes and reduced healthcare costs. 18 Therefore, this study aims to understand medication adherence better and the factors influencing non-adherence in Saudi Arabia.
Materials and Methods
Ethical Approval
The research received approval from the Biomedical Research Ethics Committee at the Faculty of Medicine, Umm Al-Qura University in Makkah, Saudi Arabia. The approval number is HAPO-02-K-012-2021-04-672 in accordance with the Declaration of Helsinki.
Study Design
A cross-sectional study involving patients with chronic diseases in Saudi Arabia was carried out. Participants were randomly contacted and invited to complete an electronic questionnaire over 4 months from May 1 to August 31, 2024. The questionnaire detailed the purpose of the study, and participants were informed that their involvement was voluntary.
Questionnaire Tool
The questionnaire was adapted from a previous study by Algarni et al. 19 Experts provided their feedback and opinions for improving the questionnaire, and their suggestions were incorporated into the final questionnaire, which contained 20 questions and was designed using online cloud-based questionnaire development software (Google Forms). The questionnaire was developed in English, translated into Arabic, the local spoken language, by proficient speakers of both languages, and revised to suit the general population. It was divided into three main parts: the first part included sociodemographic information. The second part was about the participants’ medication adherence and their reasons for non-adherence. The third part was about over-the-counter (OTC) medications, herbs, and supplements. The survey has been checked and validated to ensure its questions accurately and consistently measure what they intend to. This process involves methods like expert review (face and content validity) and testing on a smaller, representative sample of the population (pilot testing) to filter out confusing, biased, or irrelevant questions, ensuring the final data are trustworthy and actionable.
Study Populations (Inclusion/Exclusion Criteria)
The selection criteria included adults (men and non-pregnant women) above 18 years of age with chronic diseases, who took prescription and OTC drugs, and visited primary care facilities in the Makkah region of Saudi Arabia met the selection criteria. Exclusion criteria include pregnancy, incapacity to give informed permission, and concurrent major medical or surgical conditions needing hospitalization.
Sample Size and Data Collection
The sample size was determined using Slovin’s formula, based on a population of 385 patients with chronic diseases in Saudi Arabia, as reported in a recent study by Alosaimi et al. 20 The calculations were made with a confidence interval (CI) of 95% and a margin of error of 5%. Measures of effect size in analysis of variance (ANOVA) are measures of the degree of association between an effect (e.g., a main effect, an interaction, a linear contrast) and the dependent variable. They can be thought of as the correlations between an effect and the dependent variable. The questionnaire was disseminated via social media platforms. After being downloaded from the Google Forms website, every questionnaire response was saved on a secure server. Those who answered all 20 questions in the three-part survey were given a comprehensive case study of their responses. Individuals who did not complete the questionnaire were not allowed to participate. The information was gathered from the Google Forms spreadsheets and imported into Microsoft Excel.
Data Analysis and Statistics
The data were collected, reviewed, and then fed into the Statistical Package for Social Sciences version 26 (Released 2019; Armonk, NY: IBM Corp). All statistical methods used were two-tailed with an alpha level of 0.05, considering significance if the p value was less than or equal to .05. We used the Pearson chi-square and exact probability tests for small frequency distributions to measure any differences. Descriptive analysis for categorical data was done using frequencies and percentages, whereas numerical data were presented as the mean with standard deviation.
Results
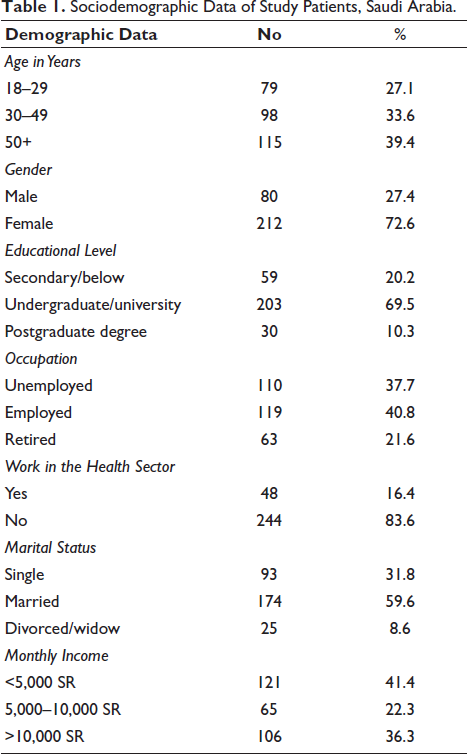
A total of 300 questionnaires were collected, of which eight were excluded because of incomplete responses, giving a response rate of 97%. In total, 292 participants were included in this study. Participants’ ages ranged from 18 to more than 50 years, with a mean age of 38.4 ± 12.5 years old. Exact of 212 (72.6%) were females, 203 (69.5%) were university graduates, and 30 (10.3%) had a postgraduate degree. As for occupation, 119 (40.8%) were employed, 110 (37.7%) were not employed, and 63 (21.6%) were retired. Only 48 (16.4%) worked or were students in the health care field. Considering marital status, 174 (59.6%) were married, 93 (31.8%) were single, and 25 (8.6%) were divorced/widowed. 121 (41.4%) participants reported a monthly income less than 5,000 SR, while 106 (36.3%) had a monthly income exceeding 10,000 SR (Table 1).
Sociodemographic Data of Study Patients, Saudi Arabia.
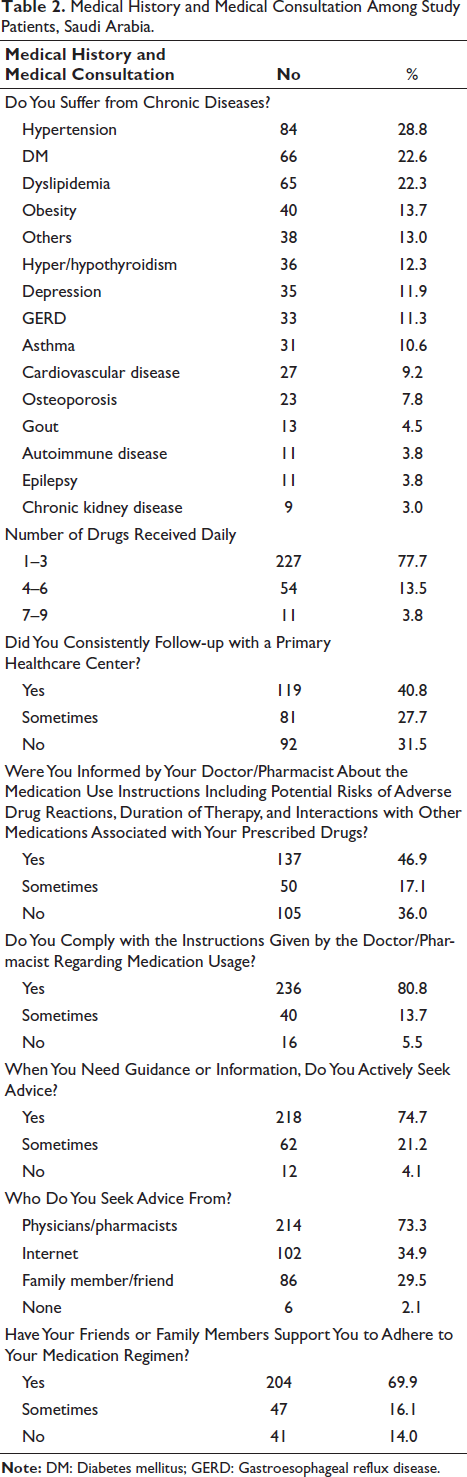
As shown in Table 2, for chronic diseases, the most reported were HTN 84 (28.8%), diabetes mellitus (DM) 66 (22.6%), dyslipidemia 65 (22.3%), and obesity 40 (13.7%). The majority of patients, 227 (77.7%), were taking 1–3 medications daily, 54 (13.5%) were taking 4–6 medications, and 11 (3.8%) were taking 7–9 medications. Only 119 (40.8%) consistently follow up with a primary healthcare center, but 81 (27.7%) did sometimes. Nearly half of the respondents, 137 (46.9%), reported being informed by their healthcare providers about the medication use instructions, potential risks of adverse drug reactions, duration of therapy, and interactions, while 50 (17.1%) were sometimes informed. As for complying with the instructions given by the doctor/pharmacist regarding medication usage, it was usually done by 236 (80.8%), and 218 (74.7%) actively seek advice when need guidance or information, mainly from physicians or pharmacists 214 (73.3%), and internet 102 (34.9%), and family members/friends 86 (29.5%). Furthermore, a majority of respondents, 204 (69.9%), reported that their friends or family members support them to adhere to their medication regimen.
Medical History and Medical Consultation Among Study Patients, Saudi Arabia.
Regarding adherence to prescribed medications, 253 (86.7%) experienced instances where they forgot to take their medications, 228 (78.1%) missed doses of medication while on vacation or traveling, 184 (63.0%) sometimes discontinue taking medications without informing their doctor/pharmacist, 175 (59.9%) sometimes stop taking their medication when they start feeling better, and 181 (62.0%) have difficulty taking medications on a hectic day, as shown in Table 3. Only 83 (28.4%) believe that they are taking an excessive number of medications, and 61 (20.9%) accidentally take one medication instead of another due to the similar color or shape of the pill or package. About OTC practice, 226 (77.4%) participants seek advice from a doctor or pharmacist before taking any OTC medications, supplements, or herbal medicines, and 186 (63.7%) believe that taking OTC medications is safe and that they do not need to consult their doctor or pharmacist about them.
Study Participants Medication Adherence Among Patients with Chronic Diseases in Saudi Arabia.
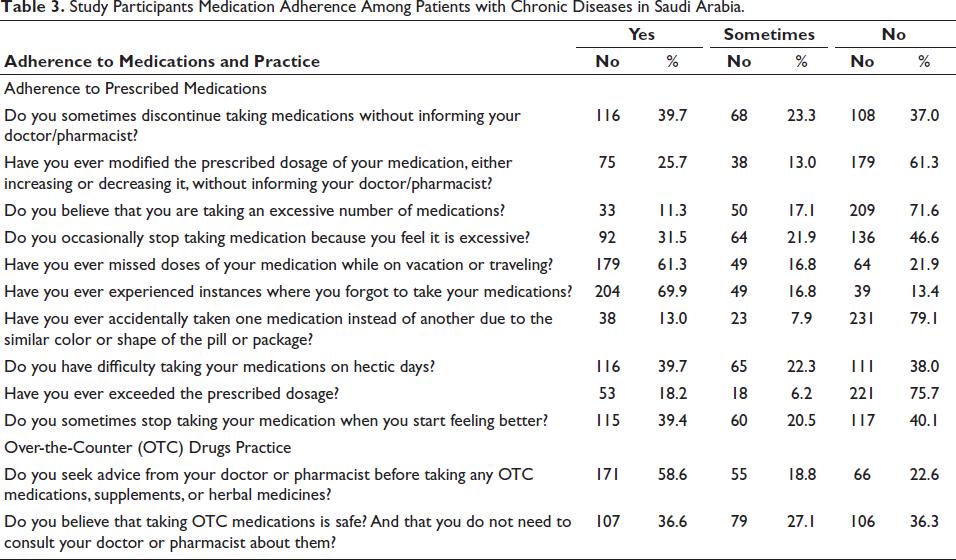
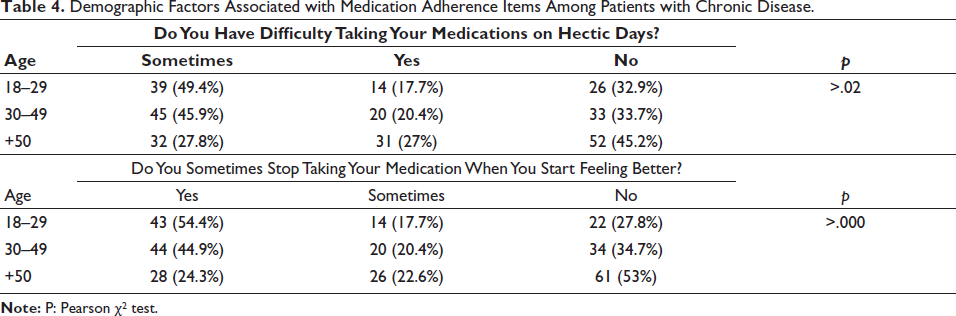
Table 4 shows demographic factors associated with medication adherence items among patients with chronic diseases in Saudi Arabia. 39 (49.4%) of participants aged 18–29 experienced difficulty taking their medications on hectic days compared to 45 (45.9%) of those aged 30–49, and 32 (27.8%) of those aged 50 and above (p = .02). Additionally, 43 (54.4%) of participants aged 18–29 stopped taking their medication when they felt better, compared to 44 (44.9%) of those aged 30–49, and 28 (24.3%) of those aged 50 and above (p = .000).
Demographic Factors Associated with Medication Adherence Items Among Patients with Chronic Disease.
As shown in Table 5, among those who seek advice from a physician or pharmacist, 67 (35.5%) discontinued medications without informing their physician/pharmacist, compared to 40 (51.3%) of those who did not seek advice (p = .02). Furthermore, 50 (23.4%) of individuals informed about medication use instructions, duration of therapy, adverse drug reactions, or drug–drug interactions modified their prescribed dosage without informing their doctor/pharmacist, compared to 44 (31.4%) of those not informed (p = .01). When supported by friends or family, 50 (24.5%) modified their dosage without informing their doctor, compared to 12 (29.3%) of those without support (p = .01). Finally, 6 (54.5%) of those receiving 7–9 drugs daily stopped taking their medication because they felt it was excessive, compared to 22 (40.7%) of those receiving 4–6 drugs daily, and 64 (28.3%) of those receiving 1–3 drugs daily (p = .004).
Medical History and Medical Consultation Factors Associated with Medication Adherence Items Among Patients with Chronic Diseases.

Discussion
This study aimed to gain insight into the factors influencing non-adherence to chronic disease medications in Saudi Arabia. Medication non-adherence is a significant issue, negatively impacting healthcare, especially for patients with chronic conditions. The findings revealed that younger patients, particularly those aged 18–29, faced more challenges in sticking to their medication routines during busy times compared to older individuals. The increased difficulty among younger adults may be attributed to lifestyle factors, such as more demanding schedules or a lower emphasis on health management than older age groups. 21
Additionally, the data indicated that (54.4%) of younger patients aged 18–29 were more likely to discontinue their medication when they started feeling better and once their symptoms improved, compared to 44.9% in the 30–49 age group and only 24.3% of those aged 50 and above (p = .000). This trend suggests that younger patients may have a less comprehensive understanding of the importance of long-term medication adherence, particularly in managing chronic conditions where stopping medication can lead to a relapse or exacerbation of the disease. 22 Our results were similar to those of multiple studies, which showed that younger adults were significantly associated with decreased adherence. Interestingly, the adherence patterns improved with age, as demonstrated by the fact that the oldest participants (aged 50 and above) were less likely to report difficulties in taking medication on hectic days (27.8%) and had the lowest rates of discontinuation when feeling better (24.3%).23, 24 This could be attributed to the likelihood that older adults are more familiar with the consequences of inconsistent medication usage, possibly due to more frequent interactions with healthcare systems or longer experience managing chronic diseases. 25
These findings highlight the necessity for targeted strategies to enhance medication adherence, particularly among younger individuals. 1 Educational campaigns that stress the importance of maintaining medication routines, even when symptoms are absent, could help improve adherence rates. 26 Additionally, introducing reminder systems or mobile health applications may help younger adults manage their medications more effectively during hectic periods. 27 Our data also revealed a connection between medical history, consultation behaviors, and medication adherence among chronic disease patients in Saudi Arabia. A key takeaway is the notable influence of seeking guidance from healthcare professionals, such as doctors or pharmacists, on adherence patterns. 28
Patients who consulted healthcare providers were less likely to stop their medications without notifying their physician or pharmacist. Specifically, 35.5% of those who sought advice discontinued their medicines without informing their provider, compared to 51.3% of those who did not seek advice (p = .02). This emphasizes the vital role healthcare providers play in educating patients about adherence and non-compliance risks. Regular communication with healthcare professionals can enhance medication adherence and lower the chances of patients discontinuing their treatments on their own. 29 Another critical factor affecting adherence was the provision of medication use instructions. Only 23.4% of informed individuals altered their prescribed dosages without consulting their provider, in contrast to 31.4% of those who were not informed (p = .01). This underscores the need for thorough patient education on medication management. Teaching patients about potential side effects and proper usage can help prevent them from making independent dosage adjustments, which may lead to negative health outcomes. 30
Support from family and friends significantly impacts medication adherence. Patients with social support were less likely to adjust their medication dosages without consulting a healthcare professional, with only 24.5% of those receiving support doing so, compared to 29.3% of those without support (p = .01). This indicates that a strong support system can encourage adherence by reinforcing medication routines and discouraging unauthorized dosage changes. Additionally, the number of medications prescribed daily was linked to adherence challenges; 54.5% of patients taking 7–9 medications reported discontinuing treatment due to feeling overwhelmed, compared to 28.3% of those on 1–3 medications (p = .004).31, 32 This suggests that polypharmacy can lead to frustration and confusion, necessitating strategies like medication reviews and simplified regimens to improve adherence among chronic disease patients. 33
While nearly 47% reported being informed about medication use, 36% indicated that they received no information, highlighting a communication gap that could lead to misunderstandings and non-adherence. Improving communication between healthcare providers and patients about medication importance and its usage is crucial for better health outcomes.34, 35 The study found that 80.8% of participants generally adhere to the medication guidelines provided by healthcare professionals, indicating a strong engagement with treatment plans. However, 19.2% of patients who sometimes or never comply highlight a need for further support and intervention. When seeking information about their medications, 73.3% of patients consult healthcare providers like physicians or pharmacists, reflecting a traditional reliance on professional advice. However, a significant number also turn to non-professional sources, with 34.9% using the Internet and 29.5% seeking input from family or friends. This reliance on varied sources could lead to inconsistent adherence and potential misconceptions about treatment. Additionally, 69.9% of participants reported receiving support from friends or family, which positively impacts adherence; however, the 14.0% without such support may face a higher risk of non-adherence. This suggests that healthcare providers should consider patients’ social environments when creating treatment plans and provide extra resources for those lacking support.36, 37
A few limitations should be noted when interpreting the results of this study. First, using an online survey may affect the sample’s representativeness, as it might exclude responses from patients who do not engage with social media; moreover, there was a potential information bias, as we used self-reported surveys. Second, the study did not analyze specific classes or subclasses of medications related to non-adherence. Third, the generalizability of the study’s findings is limited to the Makkah region due to specific local factors and potential non-probability sampling methods. This means the results may not be applicable to other regions, such as different cities or countries, because of unique local conditions like culture, demographics confined to the Makkah region. Despite these limitations, this research, involving patients with chronic diseases in Saudi Arabia, contributes valuable insights, especially given the scarcity of studies on medication non-adherence in chronic illness populations. Additionally, our study included participants taking both prescribed and OTC medications, whereas previous research has often concentrated on specific drug classes or conditions.
Conclusion
Our findings emphasize the importance of regular follow-ups with healthcare providers, effective communication about medication usage, and the need for trustworthy information sources and robust support systems.
Footnotes
Abbreviations
Acknowledgments
All authors acknowledge all the participants who helped in this survey.
Authors’ Contributions
Authors contributed equally to this work in terms of concept, methodology, analysis, writing, and revising the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the Ethics Committee for the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was taken from all participants.
Summary
In summary, focusing on factors such as clear medical instructions, social support, and the number of medications prescribed could boost medication adherence and lead to better health outcomes for patients with chronic diseases in Saudi Arabia.