
Abstract
A case of colchicine overdose of 27 mg, or 0.27 mg/kg (weight 99.8 kg), is reported to assess the potential symptoms seen with this type of toxicity and analyze a prospective treatment for successful outcomes. A 74-year-old man unintentionally ingested approximately 45 tablets of colchicine 0.6 mg, and he then presented to the hospital and received gastric lavage, activated charcoal, and whole bowel irrigation. The patient’s platelets rapidly dropped within 48 h, and he was continuously managed with supportive care and hematopoietic agents until stabilization. The patient experienced no further decline and was discharged from the hospital 15 days after ingestion. A 74-year-old male who presented with acute colchicine toxicity was successfully treated with gastric lavage, activated charcoal, and whole bowel irrigation. There have been no recorded cases of whole bowel irrigation used to treat colchicine overdose in the past 30 years.
Introduction
Colchicine is a commonly prescribed anti-gout agent. The recommended maximum dose is 1.8 mg/day for the treatment of an acute gout flare. 1 However, ingestion of high-dose colchicine can cause gastrointestinal (GI) dysfunction, severe pancytopenia, arrhythmias, and cardiac failure. 2 Accordingly, we report a case of a patient having accidentally taken up to 45 tablets of colchicine 0.6 mg in a single sitting (0.27 mg/kg). He ultimately required unremitting intensive care unit monitoring for leukopenia and thrombocytopenia consistent with marrow suppression, along with continuous cardiovascular monitoring.
Colchicine is derived from two medicinal alkaloidal plants, Colchicum autumnale and Gloriosa superba. 3 It has been used for many years for rheumatic immune diseases due to its anti-inflammatory properties. It is currently approved for gout flares and familial Mediterranean fever (FMF). 4 Colchicine interrupts cytoskeletal functions by inhibiting tubulin polymerization into microtubules, ultimately causing activation aversion, degranulation, and migration of neutrophils, correlating with resolving selected gout symptoms. 5 At larger than usual doses, it can cause disruption of protein assembly, cellular morphology, and motility, arresting mitosis and preventing cell division. 6 Colchicine is readily absorbed to a maximum serum concentration in 1–2 h after ingestion in fasting conditions. It has a low binding affinity for serum protein and a high bioavailability of 5–8 L/kg. The breakdown of colchicine is one that extensively undergoes first-pass metabolism. Colchicine undergoes demethylation via the hepatic P450 cytochrome CYP3A4 in enterocytes and hepatocytes, after which it is rapidly distributed to body tissues, including the kidney, spleen, liver, and leukocytes. Colchicine is known to undergo enterohepatic recirculation via the bile, but the exact significance of this process is not well understood. Commonly reported adverse events associated with colchicine include diarrhea, nausea, and vomiting, which are likely to occur in more than 20% of patients who take colchicine. However, GI symptoms are notably dependent on dosage and can be avoided by using the lowest dose possible and slowly titrating as necessary. 7 Colchicine’s half-life is 20–40 h at repeated therapeutic doses, and its anti-inflammatory effects continue for days after discontinuation. 8 Colchicine cannot be removed via hemodialysis, is removed 10%–20% through renal excretion, and the remainder as the parent drug in stool.
At high doses, colchicine can cause irreversible myelosuppression, leukopenia, and thrombocytopenia, as well as multiple organ failure that can occur over the course of several days. 9 It usually mimics gastroenteritis during the initial phase, 10–24 h post-ingestion. The subsequent multi-organ dysfunction phase is characterized by cardiovascular collapse, respiratory failure, renal impairment, and hepatic dysfunction. 6 Given the lack of availability, there is no known threshold for toxicity based on serum colchicine levels, and these labs are not routinely collected even in the event of an overdose due to the need to outsource blood processing, which can take several days and would hence not be useful in guiding emergent clinical decisions. Cozza et al. reported on a 32-year-old male who presented approximately 44 h after ingesting between 32.4 and 54 mg of colchicine. Pancytopenia and concomitant multi-organ failure developed rapidly during this post-ingestion stage. 10 Acute cardiac collapse has been documented in many instances of colchicine overdose. 11 Given limited data and variability of presentation, there is a lack of consensus on toxic doses; however, doses >0.5 mg/kg are most frequently (but not exclusively) reported with signs of toxicity. Ingestion of doses of 0.80 mg/kg or above has been known to be fatal and cause nearly 100% mortality. 12 Fu et al. reported the case of a 56-year-old male who seemingly consumed 12 mg (0.17 mg/kg) of colchicine and presented 40 h after ingestion with multiple organ failure, metabolic acidosis, and respiratory alkalosis. At 60 h post-ingestion, the patient required tracheal intubation for progressive decline of respiratory function. His condition rapidly deteriorated, and the patient died after developing additional hepatic dysfunction, rhabdomyolysis, and systemic inflammatory response syndrome approximately 132 h after being admitted. 9 Similarly, Little et al. reported a case of a 39-year-old who presented 2 h after co-ingestion of 0.28 mg/kg of colchicine along with high (but reported tolerable) doses of indomethacin and zopiclone. Despite early presentation and decontamination with multiple doses of activated charcoal, the patient developed metabolic acidosis, elevated INR, significant shortness of breath, leukopenia, thrombocytopenia, shock, and acute kidney injury within 36 h and eventually succumbed to multi-organ failure approximately 52 h post-ingestion.12, 13
Case Presentation
A 74-year-old man with a past medical history of hypertension, hyperlipidemia, bilateral total knee replacements, type II diabetes mellitus (T2DM), obstructive sleep apnea, and gout presented via emergency medical services (EMS) as a transfer from an outside hospital (OSH) after unintentionally ingesting approximately 45 tablets of colchicine 0.6 mg, as confirmed by patient report. Upon arrival at the OSH, the patient was alert and oriented, and he underwent gastric lavage within approximately 1 h from the patient-reported time of ingestion. Documentation of pill-fragment removal was noted at this time in the OSH reports. The patient was subsequently transferred to us as a quaternary referral center for further treatment. By the start of the post-ingestion hour three, the patient had arrived at our emergency department, where his initial vital signs included a blood pressure of 163/84 mmHg, a heart rate of 93 beats per minute (bpm), a respiratory rate of 20 breaths per minute, an SpO2 of 94%, and a temperature of 97.8℉. The patient reported no symptoms of chest pain or shortness of breath. He was alert, oriented, and appeared to be in no acute distress. Initial lab tests were notable for a white blood cell count of 2,300/µL, an absolute neutrophil count (ANC) of 770/µL, troponin <0.01 ng/mL, and platelets of 138,000/µL (Table 1). At this time, the labs also demonstrated a lactate level of 3.0 mmol/L and liver enzyme markers of alanine aminotransferase (ALT) and aspartate aminotransferase (AST) at 28 and 22 units/L, respectively. Obtaining serum colchicine levels differed by the emergency medicine and toxicology teams, given no available equipment for rapid evaluation of serum colchicine levels, and a send-out lab was anticipated to take several days. A lactated Ringer’s infusion was started at 125 mL per hour to facilitate hydration and resuscitation. Given that the patient had presented in the early stage of an overdose, undergone gastric lavage, and not yet demonstrated signs of toxicity, the decision was made to insert a nasogastric (NG) tube and initiate whole bowel irrigation (WBI) using polyethylene glycol (Golytely) solution, given at 4,000 mL per hour for 2 h for two rounds. During the first round of WBI, the patient reported symptoms of nausea and was given intravenous ondansetron 4 mg. Filgrastim-sndz 480 µg was administered subcutaneously for anticipated neutropenia that has been reported in severe cases of colchicine overdose. After the completion of the second round of polyethylene glycol WBI, 50 g of activated charcoal solution are administered for acute drug toxicity. He was then admitted to the medical intensive care unit (MICU) for ongoing treatment and care.
Post-ingestion Timeline of Patient Symptoms, Lab Trends, and Treatments.
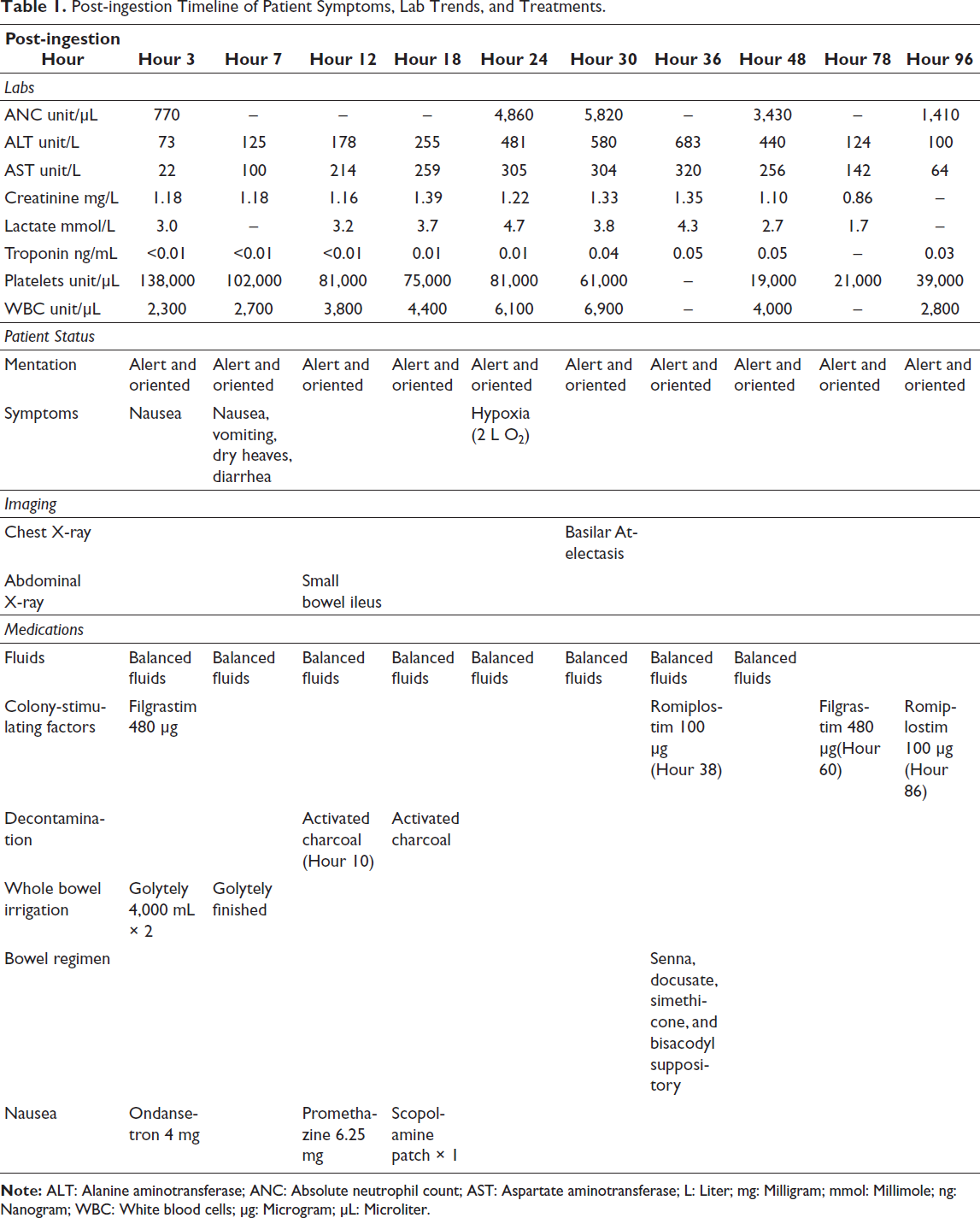
Shortly after his admission to the MICU, the patient was given promethazine 6.25 mg intravenously for nausea and a second round of 50 g of activated charcoal solution. At this time, the patient had a slight elevation in serum lactate (3.2 mmol/L) but was still asymptomatic otherwise. The decision was made to start an infusion of sodium bicarbonate despite low-quality evidence in helping with his mild, stable lactic acidosis. 14 Lactate continued to be monitored every few hours due to concern for the likelihood of an upsurge. Over the next several hours after the irrigation process, the patient had many bouts of diarrhea and vomiting but maintained normal mental status. By 18 h after ingestion, most of the vomiting had turned to dry heaving. He was reportedly fatigued and tired but remained afebrile. A chest X-ray was performed to look for signs of aspiration after vomiting in the setting of activated charcoal use, which showed bibasilar atelectasis. A complete blood count (CBC) and troponin were checked every 6–8 h. Creatinine kinase (CK) was checked every 12 h to look for signs of rhabdomyolysis. After 36 h post-ingestion, the patient was still experiencing diarrhea, dry heaves, and abdominal bloating but reported no chest pain or shortness of breath. His liver function tests (LFTs), lactate, and troponin were all trending upward. A transthoracic echocardiogram (TTE) was performed, with the results showing a normal left ventricular size, and no significant valvular disease was noted. At 48 h, his platelets dropped to critical levels (19,000/µL), and romiplostim 100 µg was administered subcutaneously. By 60 h, his lab markers were all normalizing, and a repeated dose of romiplostim 100 µg was given at 72 h. Throughout the course of the next few days under ICU monitoring, blood pressure ranged from 109/66 to 172/92 mmHg, and his heart rate ranged from 64 to 96 bpm. The patient remained stable throughout his admission and was transferred out of the ICU 8 days after the overdose and discharged home 15 days after the incident.
A Brief Review of Decontamination Strategies
Methods
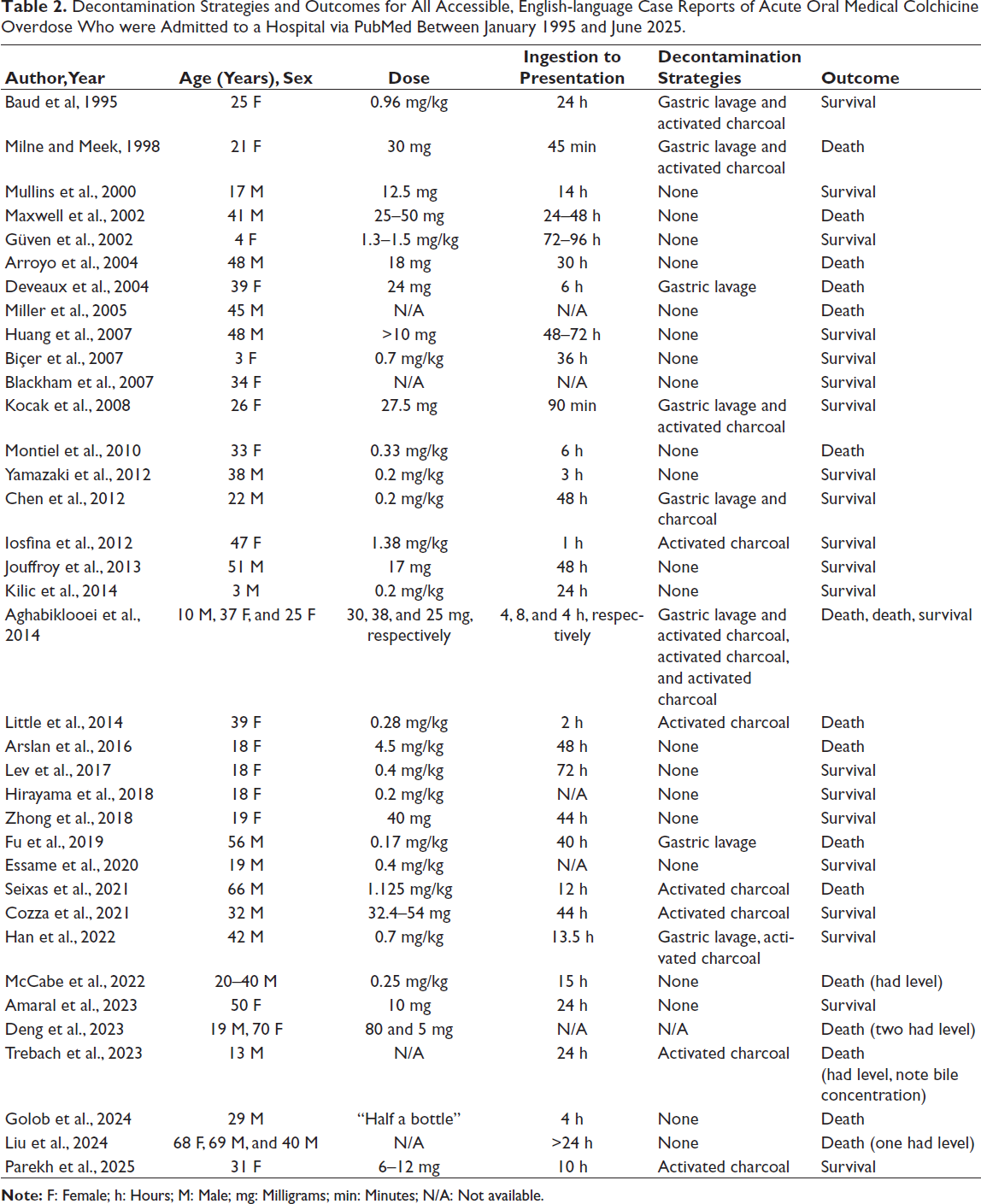
We performed a review of all accessible, English language-reported cases of colchicine overdoses between January 1995 and June 2025 via PubMed. We only considered cases where the overdose was due to oral, medicinal colchicine, given that there are reports of intravenous, intranasal, and plant-based colchicine overdoses. We also only considered scenarios where the patient survived until presentation to the hospital, to account for cases where overdose was suspected in the case of out-of-hospital death. Attention was given to the patient’s age and sex, the probable dose of colchicine taken, the estimated time from ingestion to healthcare presentation, types of decontamination strategies employed, and the outcome of survival or death from that hospital encounter (Table 2).
Decontamination Strategies and Outcomes for All Accessible, English-language Case Reports of Acute Oral Medical Colchicine Overdose Who were Admitted to a Hospital via PubMed Between January 1995 and June 2025.
Results
We present the results of 41 patients from 36 case reports over the past 30 years.10–12, 15–46 In total, 21 of these patients (≈51%) were male. Of the 40 patients with a known age, the median age was 32.5 years with a range of 3–70 years. Doses of colchicine and patient body weight were not consistently reported in these studies, with suspected flat doses ranging from 6 to 80 mg and weight-based doses ranging from 0.2 to 1.5 mg/kg. Only five of these patients had serum colchicine levels reported (and one bile colchicine level); however, this information never impacted the management of their clinical course. The time from known or suspected ingestion to presentation varied greatly, ranging from 45 min to 96 h. Mortality was high, with 19 patients (≈46%) not surviving their hospital admission. Death occurred with doses lower and equivalent to our patient (e.g., 0.17, 0.25, and 0.28 mg/kg).
It is important to note that clinical presentation, suspicion of overdose, co-ingestion, and time since ingestion likely contributed to the choice of decontamination and outcomes for these patients, given that several reports acknowledged the utility of early gastric lavage and activated charcoal, even if the patient was not treated with either method. The narrative of several reports also focused primarily on a specific aspect of the treatment course, such as the use of colony-stimulating agents, extracorporeal membrane oxygenation, serum troponin markers, dialysis or plasma exchange, acute kidney injury, serum colchicine trends, and so on. When looking at the reported decontamination strategies, only 8 patients (19.5%) were treated with a gastric lavage, and 14 patients (34.1%) were treated with activated charcoal. In total, 23 patients (56%) had no reported decontamination strategies, and two patients’ reports were unclear on the supportive therapies they received. To our knowledge, WBI has never been reported for the treatment of colchicine overdose.
Discussion
Although many other medications and substances have a chemical antidote available that can be used in clinical settings of acute toxicity, colchicine does not have a reversal agent that clinicians can use. Thus, management of colchicine toxicity is mainly supportive. Knowing what is likely to occur in a situation of colchicine overdose helps medical staff be able to treat a patient more efficiently. Multiple other reports of acute colchicine toxicities include a frontload of GI symptoms, such as abdominal discomfort, nausea, vomiting, and diarrhea, within 24 h after ingestion. Over the period of 24 h to 7 days, patients may experience a large array of symptoms, including hypovolemia, pancytopenia, renal failure, liver failure, cardiac arrhythmias, encephalopathy, hemolysis, convulsions, sepsis, and acute respiratory distress syndrome (ARDS). Hemodynamic instability, cardiac arrhythmias, along with infectious and hemorrhagic complications, remain at the top of the list of concerns for death from acute colchicine poisoning. 6 The recovery phase is sometimes accompanied by transient alopecia. Throughout this process of potential multi-organ failure, providing decontamination measures and high-quality supportive care remains key to patient outcomes in this setting. There have been no reported cases of the management of a colchicine overdose with early decontamination strategies with WBI.
In the case of our patient, GI decontamination processes of functionally removing the contents of the GI tract took place prior to his arrival at our hospital. While many overdose or poisoning scenarios do not provide the best circumstances for performing gastric lavage in patients, it was considered the best initial resolution in our patient due to the excessive amount of ingested colchicine and given his quick arrival to the emergency department (within 1 h of ingestion). Evidence from clinical studies, including human volunteer trials, suggests that decontamination may reduce the absorption of toxins in the GI tract and may be helpful in select circumstances, particularly for those who present within 60 min of ingestion. 47 In one case of colchicine overdose, gastric lavage was performed 40 h post-ingestion with no improvement seen, likely due to the extended timeframe from consumption. 9
Activated charcoal has been a primary agent used in toxicity situations dating back to the 1800s. 13 It works by surface adsorption of the toxic substance, thereby inhibiting the absorption in the GI tract and preventing systemic toxicity. It is also continued to remain a debatable subject among clinical decision makers due to its unclear magnitude of effectiveness. Hoegberg et al. reported a benefit of activated charcoal beyond 1 h in many clinical circumstances. 48 Many other reports on the use of activated charcoal have concluded that its use is significantly dependent on the type of substance ingested and the amount of toxin consumed. Case examples include scenarios in which activated charcoal has been used even hours into the digestion of the substance, but with varying outcomes of survival and death. 11 In our case, the attempt to lower GI absorption remained one of the top priorities and, in turn, was administered at hours 10 and 17 post-ingestion.
WBI is a form of detoxification in acutely poisoned patients where osmotically balanced polyethylene glycol electrolyte solution (PEG-ES) is administered at large rates to induce liquid bowel movements and flush out the toxins in a timely manner. In cases of severe toxicity, 1.5–2 L is suggested to be given per NG tube every hour until the rectal discharge is clear (a timeframe of about 6 h). WBI can come with several adverse effects, such as nausea, vomiting, diarrhea, abdominal cramps, abdominal distention, and vomiting with aspiration. 49 Deguigne et al. reported that treatment with WBI was performed with successful induction of diarrhea in 47% of cases versus those given a placebo and was associated with a relatively low risk of complications. 50 To our knowledge, no other cases of colchicine toxicity have reported the use of WBI as a form of treatment, likely due to the challenge of patient tolerability and concerns for the potential to develop intestinal ileus. Balancing the high likelihood of adverse effects, including aspiration risk, nausea, and vomiting, requires close monitoring with the need to aggressively treat symptoms, which likely makes WBI an unfavorable option in this setting.
Conclusion
Colchicine overdose may not always be quickly recognized upon a patient’s arrival at a medical facility. However, if reported or suspected, medical providers’ early recognition of this toxicity is crucial to patient outcomes. We report our case to highlight the effects of preventing poison absorption promptly and providing fundamental supportive care throughout the post-ingestion phase. Furthermore, we report the addition of WBI as part of our treatment plan to be unique in the case of a colchicine overdose and conceivably correlate to the positive outcome in our patient. Overall, we took a general approach to drug poisoning with the use of historically well-known methodologies along with close monitoring and supportive measures due to the high likelihood of non-survival without exhaustive interventions.
Footnotes
Abbreviations
Acknowledgments
The authors would like to acknowledge the efforts of Shelby Lanham, PharmD, Candidate at Belmont University College of Pharmacy, Nashville, TN, USA, for her efforts in composing this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study/work was approved by the Vanderbilt University Medical Center Institutional Review Board.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Casey reported receiving travel support from Fisher & Paykel outside the submitted work.
Informed Consent
Not applicable.