
Abstract
Background
Medical students experience a heightened risk of depression and necessitate effective, low-side-effect interventions.
Purpose
This study evaluates the efficacy of saffron in decreasing salivary cortisol levels and alleviating mild depressive symptoms in medical students.
Materials and Methods
A randomized controlled trial (RCT) was conducted with eligible undergraduate medical students. Participants were assigned to either the intervention group, which received saffron tablets, or the placebo group for an 8-week duration. Depressive symptoms were assessed using the Hamilton Depression Rating Scale (HDRS), while salivary cortisol levels were measured via enzyme-linked immunosorbent assay (ELISA). Measurements were taken at baseline, week 4, and week 8.
Results
Among 56 participants (28 in each group), the saffron group exhibited significantly lower HDRS scores compared to the placebo group at week 8 (10.5 vs. 18; p < .001), alongside a notable downward trend (p < .001). No significant differences in HDRS were observed at week 4 (p = .302). Salivary cortisol levels did not show significant differences between groups (p > .05), although the saffron group exhibited a decreasing trend while the placebo group showed an increasing trend.
Conclusion
Saffron demonstrates efficacy in reducing mild to moderate depressive symptoms among medical students, although it does not lead to significant changes in salivary cortisol levels.
Introduction
Mental disorders, particularly depression, are garnering increasing global attention due to their adverse effects on individual capabilities and performance. Healthcare professionals, who constitute the backbone of health systems worldwide, often grapple with depression stemming from challenging work environments, excessive workloads, fatigue, and substantial work-related pressures. Similarly, medical students, as the future cohort of healthcare providers, exhibit notably higher rates of depression compared to their peers in other fields. The rigors of medical education contribute to this elevated prevalence. 1 Indeed, it is estimated that approximately 28% of medical students globally suffer from depression, with rates of suicidal ideation reported at 11.1%.2–4 Notably, a recent meta-analysis highlighted that 27.2% of medical students across 47 countries display depressive symptoms, with findings indicating that nearly one in four medical students in Jakarta also experience such symptoms. While the prevalence of depression varies across different countries and regions, several studies indicate that the contributing factors appear to be remarkably consistent.1, 5, 6
Depression is a multifaceted syndrome with various clinical manifestations that can differ among individuals. It is characterized by sustained feelings of sadness, a diminished interest in activities once enjoyed, and a significant impairment in daily functioning that lasts for at least 2 weeks. The ramifications of depressive episodes can be severe, contributing to approximately 800,000 suicides worldwide each year. Without appropriate intervention, this may result in a considerable loss of future healthcare practitioners.3, 7
Pharmacotherapy, primarily using anti-depressants, remains the standard approach for treating depression. However, the effectiveness of these medications in addressing mild to moderate depression is subject to ongoing debate. Research indicates that while anti-depressants offer significant benefits for individuals with severe depression, their impact on those with mild to moderate forms appears limited.8, 9 Additionally, the side effects associated with synthetic anti-depressants can hinder their overall efficacy, often preventing patients from achieving complete remission.8, 9
Herbal medicine is increasingly recognized as a viable alternative for treating depression, primarily due to its lower cost and reduced side effects compared to synthetic options.8, 9 Current clinical evidence suggests that herbal remedies can exert effective anti-depressant effects, particularly in patients with mild to moderate depression. Over recent decades, herbal medicines have been widely prescribed globally as complementary and alternative therapies for depression. Saffron, derived from the Crocus sativus flower, has emerged as a promising candidate for depression treatment. Its bioactive components, including safranal, crocin, and crocetin, exhibit significant anti-oxidant properties by elevating superoxide dismutase (SOD) levels and enhancing glutathione availability while simultaneously reducing markers of lipid peroxidation. These mechanisms are anticipated to alleviate depressive symptoms, which have been associated with oxidative stress and reductions in anti-oxidant enzymes such as glutathione peroxidase (GSH-Px), catalase, and SOD.9–11 Additionally, preclinical studies suggest that crocin affects the serotonergic system and may alleviate obsessive-compulsive behaviors in mice by antagonizing the 5-HT2C receptor. 12
Clinical trials investigating the efficacy of saffron in treating depression have emerged over the past few decades. Findings indicate that patients administered 30 mg/day of saffron for 6 weeks exhibited significant improvements in depression symptoms, as measured by the Hamilton Depression Rating Scale (HDRS), in comparison to those receiving a placebo. 13 A meta-analysis of randomized controlled trials (RCTs) further supports the effectiveness of saffron for unipolar depression, demonstrating an efficacy comparable to that of synthetic anti-depressants while also presenting a favorable safety profile. Variability in study outcomes is largely attributed to differences in dosage (ranging from 30 to 100 mg/day), treatment duration (6–12 weeks), the type of comparator anti-depressant used, and the specific depression assessment tools employed (such as the Beck and Hamilton scales). Nonetheless, despite these methodological variations, the collective evidence consistently demonstrates saffron’s superiority over placebo and its comparable effects to conventional anti-depressants. 14
Saffron has demonstrated efficacy in alleviating mild to moderate depression among young adults, including those in college, as evidenced by multiple clinical trials.15, 16 However, research specifically examining the effectiveness of saffron in treating depression within the medical student demographic remains absent. This study seeks to assess the impact of saffron administration on salivary cortisol levels and the clinical symptoms associated with mild to moderate depression in medical students. The findings are anticipated to enhance the body of evidence supporting saffron’s potential as a viable option for medical students, who often experience heightened stress and may be reluctant to use conventional anti-depressants due to concerns about side effects, such as cognitive impairment or drowsiness, and the associated stigma.
Materials and Methods
Study Design and Participants
This research employs an analytical experimental design utilizing the RCT methodology with random sampling. The study involved two groups: one group received saffron tablets as treatment, while the control group administered placebo tablets. Recruitment took place between August 2024 and the enrollment of a sufficient number of participants from the Medical Education Study Program at our medical faculty. All study protocols obtained ethical approval from the local research ethics commission (reference number: 644/UN4.6.4.5.31/PP36/2024). Additionally, the study is registered with the Research Registry under the number
The study sample comprised undergraduate students with mild to moderate depression, as indicated by Patient Health Questionnaire-9 (PHQ-9) self-report scores ranging from 5 to 19. Initially, all samples were examined for their mental status to ensure they met the inclusion and exclusion criteria. Inclusion criteria required participants to be registered as active students in semesters 2 through 7. Exclusion criteria included a diagnosis of severe mental disorders (i.e., manic bipolar disorder, organic mental disorders, and mental disorders caused by the use of psychoactive substances), current use of anti-depressant or corticosteroid medications within the past month, the presence of chronic physical illnesses requiring treatment, or being pregnant or enrolled in a pregnancy program. Participants were classified as dropouts if they exhibited severe depression during the study, transitioned from a depressive to a manic or hypomanic phase for those with bipolar disorder, were inconsistent in saffron consumption, were uncooperative in clinical symptom assessments, experienced severe physical illness necessitating alternative medications, or suffered significant side effects from saffron.
The sample size was calculated using a formula for experimental design, specifically for an unpaired numerical comparison between two groups across multiple measurements. The parameters used in the formula included an alpha of 0.05, a beta of 0.20, a minimum significant difference of 0.10, a standard deviation (SD) of 15.81, an intraclass correlation of 0.30, and an estimated dropout rate of 10%. Consequently, the minimum sample size required for each group in this study was determined to be 12. Participants were randomly assigned to either the treatment or placebo group in a 1:1 ratio.
Randomization and Masking Procedure
Participants will be provided with sealed envelopes containing randomly assigned numbers from 1 to 60. Participants numbered 1–30 will be allocated to the Safranin group, while those numbered 31–60 will be assigned to the placebo group. Both the placebo and saffron tablets will be indistinguishable in appearance, with congruent coating colors, shapes, and sizes.
Procedures
Both study groups received oral treatment in tablet form. The active tablets, supplied by Pharmactive Biotech Products SLU, contained 15 mg of standardized saffron extract (affron®) derived from the stigmas of C. sativus L. These extracts were standardized to contain over 3.5% Lepticrosalides, which include key bioactive compounds such as safranal and crocin. The saffron was cultivated in Alborea (Albacete, Spain) and processed at Pharmactive Biotech Products SLU’s facility in Madrid to produce affron® 3.5% Lepticrosalides®. The placebo tablets were formulated with the same excipients as the active tablets (microcrystalline cellulose and calcium hydrogen phosphate) and were also manufactured and packaged in Spain.
The Safranin group received a daily oral dose of 30 mg of saffron tablets once a day, either before or after meals, for 8 weeks. The control group received placebo tablets on the same schedule. To maintain uniformity, participants were provided with a diary to document their daily intake of either the Safranin or placebo tablets.
Outcomes
In this study, we assessed two primary parameters: clinical symptoms of depression and cortisol levels. Clinical symptoms of depression were evaluated using the HDRS, with classifications as follows: no depression (scores 0–7), mild depression (scores 8–16), moderate depression (scores 17–24), and severe depression (scores >25). Cortisol levels were determined via an enzyme-linked immunosorbent assay (ELISA) method using morning saliva samples. Both parameters were measured at three time points: baseline, week 4, and week 8.
Statistical Analysis
Categorical data in this study, including gender, study cohort, and PHQ-9 screening results, are expressed as percentages for each category. Numerical data, comprising age, HDRS scores, and salivary cortisol levels, are reported as mean ± SD for normally distributed data or as median (range) when not normally distributed. Initially, the Mann–Whitney U test or chi-square test was employed to assess differences in median values or the distribution of categorical proportions between the two groups. Subsequently, an independent t-test or Mann–Whitney U test was utilized to differentiate HDRS scores and salivary cortisol levels between the two groups at each measurement time point. Additionally, a repeated measures analysis of variance (ANOVA) or the Friedman test was conducted to analyze differences in HDRS scores and salivary cortisol levels over time within the same group. Finally, the correlation between HDRS scores and salivary cortisol levels was evaluated using either Pearson or Spearman correlation coefficients. Furthermore, sensitivity analysis was performed using the intention-to-treat analysis method. Missing data were handled using the estimation maximization method, a single imputation approach. The test results were declared robust or not. Statistical significance was defined as a p value ≤ .05, and all analyzes were performed using Statistical Package for the Social Sciences (SPSS) for Windows version 24.0 (IBM, USA).
Results
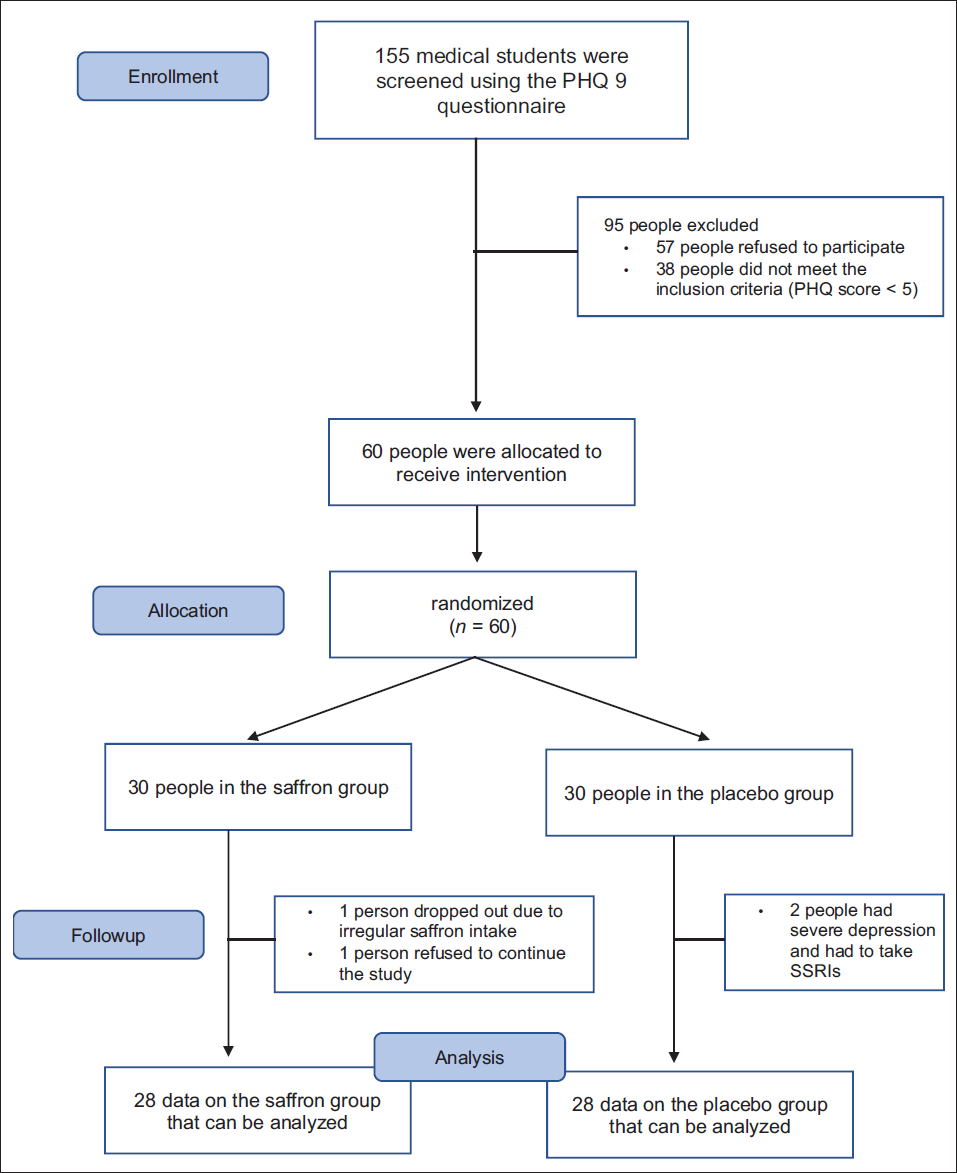
Following the screening with the PHQ-9, 60 research participants were allocated into two groups: one consisting of 30 individuals who received a placebo, and the other comprising 30 individuals who received saffron. During the follow-up phase of the study, two participants from the placebo group withdrew due to non-compliance with the study protocol regarding saffron consumption. Conversely, two individuals in the saffron group exited the study as they experienced significant depressive symptoms that necessitated pharmacological intervention. The Consolidated Standards of Reporting Trials (CONSORT) flow diagram illustrating participant progression is presented in Figure 1.
Consolidated Standards of Reporting Trials (CONSORT) Study Participant Flow Diagram.
Baseline Participant Characteristics
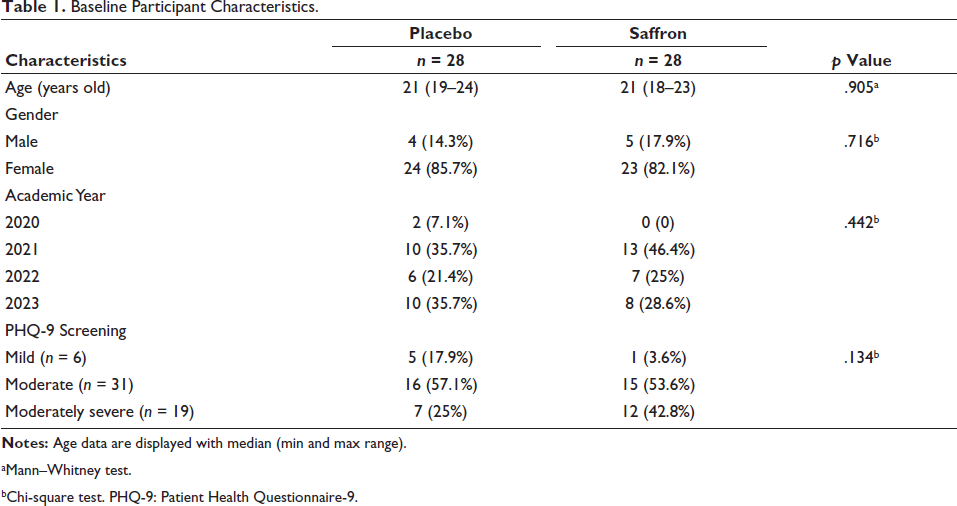
Table 1 presents a comparison of the characteristics of research subjects across the two groups. The median age of participants in both groups was 21 years. The study predominantly involved female subjects, with 24 (85.7%) in the placebo group and 23 (82.1%) in the saffron group. Male participants comprised 4 (14.3%) in the placebo group and 5 (17.9%) in the saffron group. Regarding the academic year, the largest cohort was from the class of 2021, with 13 (46.4%) in the saffron group, while the placebo group included equal numbers from the classes of 2021 and 2023, each comprising 10 (35.7%). The most frequently observed PHQ-9 screening outcome for both groups was mild depression, affecting 16 (57.1%) participants in the placebo group and 15 (53.6%) in the saffron group. Statistical analysis revealed no significant differences between the two groups in terms of age, gender, academic year, or PHQ-9 depression category (p > .05), indicating a homogeneous distribution of characteristics among the study groups.
Baseline Participant Characteristics.
aMann–Whitney test.
bChi-square test. PHQ-9: Patient Health Questionnaire-9.
Comparison of Changes in Clinical Symptom Scores of Depression Between the Placebo and Saffron Groups
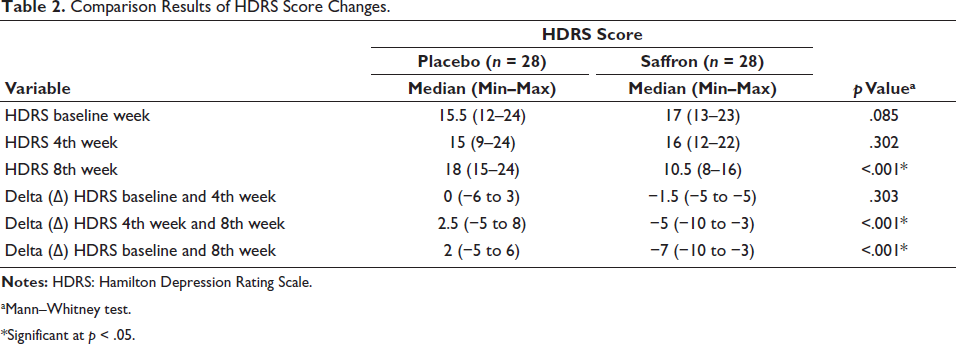
A comparison of HDRS scores between the placebo and saffron groups is outlined in Table 2. At baseline (week 0), the median HDRS score for the placebo group was 15.5, categorized as mild depression, while the saffron group had a median score of 17, indicating moderate depression. Statistical analysis revealed a p value of .085, indicating a marginally significant difference between the groups at this time point. Further analysis using analysis of covariance (ANCOVA) testing with age as a numerical covariate confirmed that there was no significant difference in baseline HDRS scores between the two groups (p value of corrected model .454). By week 4, the median HDRS score for the placebo group had decreased to 15 (mild depression), while the saffron group’s score had dropped slightly to 16 (still mild depression). However, no significant difference was observed in HDRS scores between the two groups at week 4. In contrast, by week 8, the median score for the placebo group rose to 18, reflecting a transition to moderate depression, while the saffron group demonstrated a significant reduction in score to 10.5, corresponding to mild depression. Notably, statistical comparisons indicated a significant difference in HDRS scores between the placebo and saffron groups at week 8.
Comparison Results of HDRS Score Changes.
aMann–Whitney test.
*Significant at p < .05.
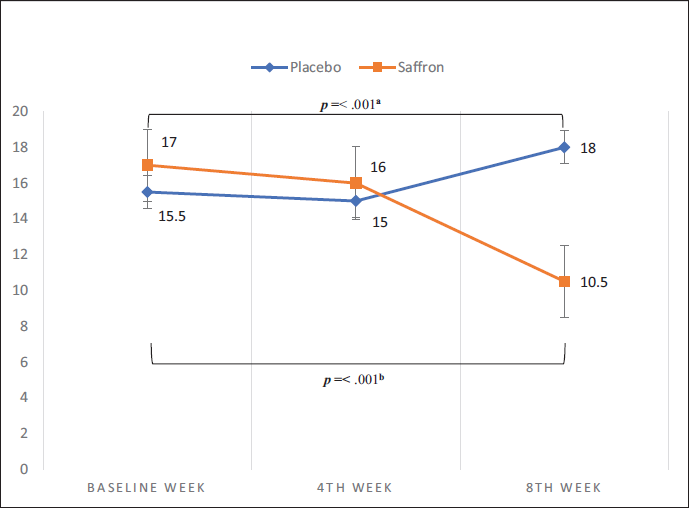
A comparison of HDRS scores across observation time points for each group is illustrated in Figure 2. Between weeks 0 and 4, no significant differences in HDRS scores were observed between the placebo and saffron groups. However, from week 4 to week 8, notable changes in HDRS scores were identified; the placebo group exhibited an increase in scores, while the saffron group demonstrated a decrease. Statistical analyzes confirmed a significant difference in the changes in HDRS scores during this period. Additionally, when comparing HDRS scores from week 0 to week 8, an increase in scores was observed in the placebo group, while a decrease was noted in the saffron group, with statistical tests indicating a significant difference in these changes between the two time points. Sensitivity analysis indicates a robust conclusion for the statistical test interpretation regarding the HDRS score changes in both groups.
Comparison of Changes in Salivary Cortisol Levels Between the Placebo and Saffron Groups
A comparative analysis of salivary cortisol levels between the placebo and saffron groups is summarized in Table 3. At baseline (week 0), the placebo group exhibited an average salivary cortisol level of 6.939, while the saffron group had a level of 10.332. Statistical analysis indicated no significant differences between groups at this time point. By week 4, salivary cortisol levels had risen to 8.329 in the placebo group and 11.679 in the saffron group, with no significant differences observed between the groups. At week 8, the average salivary cortisol levels decreased to 8.225 in the placebo group and 7.582 in the saffron group, again showing no significant differences between the two groups.
Comparison Results of Changes in Salivary Cortisol Levels.
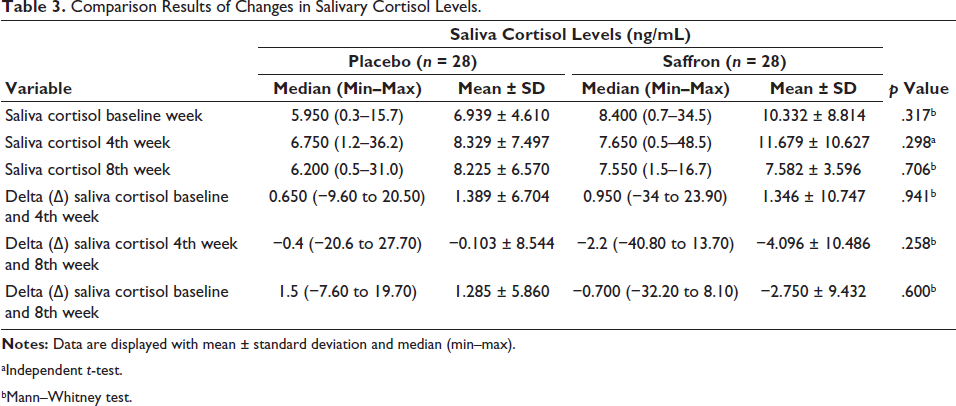
aIndependent t-test.
bMann–Whitney test.
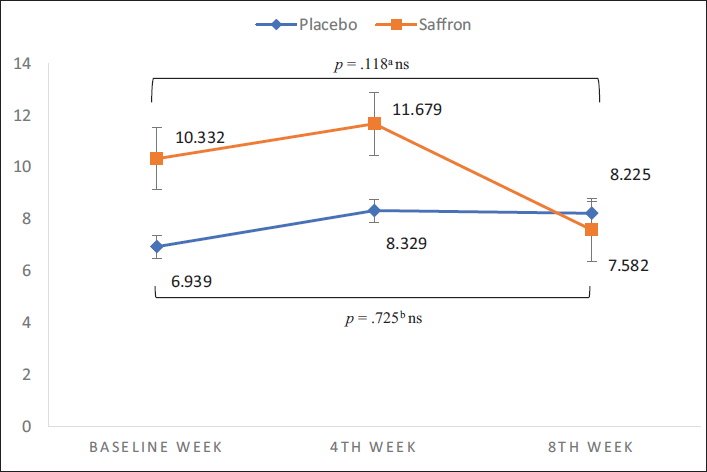
A comparison of salivary cortisol levels at various observation periods within each group is illustrated in Figure 3. Between weeks 0 and 4, cortisol levels increased in both the placebo group (1.389) and the saffron group (1.346), although the analysis did not reveal a significant difference between the two groups. When comparing cortisol levels from week 4 to week 8, both groups exhibited a decline, with the placebo group showing a change of −0.103 and the saffron group showing a change of −4.096. Moreover, no significant difference was found between the two groups. Additionally, the difference in cortisol levels from week 0 to week 8 increased 1.285 ng/mL in the placebo group, but decreased 2.570 ng/mL in the saffron group. No significant changes were detected in either group through statistical analysis. Sensitivity analysis indicates a robust conclusion of the statistical test interpretation regarding the salivary cortisol level changes in both groups.
Correlation of HDRS Scores and Salivary Cortisol Levels in the Placebo and Saffron Groups
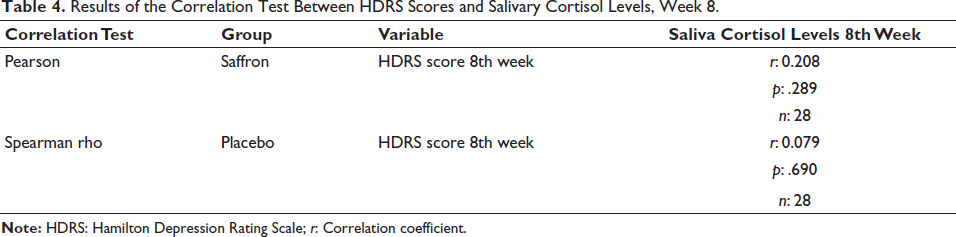
Table 4 presents the results of the correlation analysis between HDRS scores and salivary cortisol levels within the saffron and placebo groups. No significant correlations were observed at week 8. In the saffron group, the significance value was 0.289, indicating an insignificant relationship, as supported by a Pearson correlation coefficient of 0.208, which reflects a very weak correlation. Similarly, the placebo group exhibited a significance value of 0.690, suggesting a lack of significant correlation, with a Spearman correlation coefficient of 0.079, also indicating a very weak association. Sensitivity analysis confirms a robust conclusion regarding the statistical test interpretation of the correlation between HDRS scores and salivary cortisol levels in both groups.
Results of the Correlation Test Between HDRS Scores and Salivary Cortisol Levels, Week 8.
Discussion
The study demonstrated that saffron administration significantly reduced depressive symptoms, with a marked improvement from moderate to mild depression by week 8, as measured by the HDRS. Additionally, the length of saffron treatment was correlated with lower HDRS scores in participants with mild to moderate depression.
The findings of this study are reinforced by a meta-analysis conducted by Yang et al., which reported that saffron led to more significant reductions in depressive symptoms compared to a placebo. Furthermore, saffron demonstrated efficacy comparable to synthetic anti-depressants, including tricyclic anti-depressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs). Secondary analyzes from this meta-analysis indicate that saffron’s effectiveness in achieving remission for unipolar depressive disorder parallels that of synthetic anti-depressants. 14 Additionally, a supporting meta-analysis by Dai et al. found saffron to be more effective than a placebo in alleviating mild to moderate depression. Upon re-evaluating the sources of heterogeneity in saffron treatment, the analysis revealed that neither the treatment duration nor the saffron dosage contributed to the observed variability in outcomes. 17 Notably, a clinical trial by Midaoui et al. found significant benefits from saffron treatment within just one week, as evidenced by reductions in depression scale scores and an overall improvement in treatment outcomes. 10
The findings of this study indicate no statistically significant differences in salivary cortisol levels between the placebo and saffron groups at weeks 0, 4, or 8, nor in the changes observed from week 0 to week 4, week 4 to week 8, or week 0 to week 8. Despite the lack of significant findings, a trend toward decreased salivary cortisol levels was noted in the saffron group compared to the placebo group. A comprehensive analysis revealed that at baseline (week 0), the average salivary cortisol levels among the 56 participants fell within normal ranges, with only four subjects demonstrating cortisol levels exceeding the expected range of the ELISA kit (5–21.6 ng/mL). Notably, these four subjects were part of the saffron group, and their salivary cortisol levels returned to normal by weeks 4 and 8. These results underscore the potential therapeutic effects of saffron in modulating salivary cortisol levels. Furthermore, this suggests a valuable direction for future research to investigate saffron’s efficacy in populations with elevated baseline cortisol levels, particularly in individuals with depressive disorders.
Another factor that may explain the generally normal cortisol levels in the subjects of this study may also be related to the subtype of depression experienced. The subjects of this study were predominantly those with mild to moderate depression, representing a less severe subgroup of depression that is not melancholic and is not accompanied by psychotic symptoms, so that cortisol levels in the subjects of this study tended to be normal. This study is supported by previous research from Herane-Vives et al., which has found no increase in daily salivary cortisol levels in subjects with depression. 18 This condition shows that, in addition to the subtype, the severity of depression plays an important role in explaining the variation in cortisol levels in depression, especially in cases of depression treated on an outpatient basis. This may differ if the depressed subjects are a group of patients with severe depression who are hospitalized. Additionally, the heterogeneity of symptom profiles, symptom severity, and cortisol specimens may explain these varying results.
Dysregulation of the hypothalamic–pituitary–adrenal (HPA) axis has been well-established as a contributing factor to the onset of major depressive disorder in adulthood. A recent meta-analysis conducted by Zajkowska et al., which reviewed 26 studies and included 14 in the quantitative analysis, specifically examined the role of the HPA axis in adolescent and young adult depression on a global scale. The findings indicate elevated morning cortisol levels in individuals with depression; however, no significant differences were observed in evening cortisol levels. Notably, in cross-sectional studies, morning cortisol levels did not significantly differentiate between healthy controls and those with unipolar depressive disorders. Additionally, the meta-analysis suggested that both increased morning and evening cortisol levels serve as risk factors for depression rather than indicators of unipolar depression, particularly in adolescents. 19
Additionally, the diversity of salivary cortisol levels in both groups is another factor that needs consideration. In this study, the values for salivary cortisol levels in both groups were very diverse and had an extensive range between each subject, namely, the mean value and SD for the saffron group at weeks 0, 4, and 8 were (10.332 SD ± 8.8140; 11.679 SD ± 10.6271; 7.582 SD ± 3.5967), while for the placebo group the mean value and SD at weeks 0, 4, and 8 were (6.939 SD ± 4.6101; 8.329 SD ± 7.4978; 8.225 ± 6.5707), so that this also played a role and contributed to the results of the statistical test analysis.
Morning cortisol testing is considered representative because it is known that peak cortisol levels are reached approximately 30 min after waking up. This initial peak is known as the cortisol awakening response (CAR). 20 Additionally, findings from a meta-analysis by Zajkowska et al. suggest that morning cortisol levels increase in individuals with depression, but not in the evening. 19 Furthermore, the study also showed that morning cortisol levels were not significantly different between healthy controls and individuals with unipolar depressive disorder in a cross-sectional study. Thus, the study explains that increased cortisol in the morning is a risk factor for depression, not a marker or biomarker for unipolar depression, especially in the adolescent age group.
The findings from the study at weeks 4 and 8 indicated no significant differences in salivary cortisol levels between the placebo and saffron groups. It is well recognized that prolonged exposure to stressors can lead to overstimulation of the HPA axis, resulting in varying cortisol levels. The study participants, who were medical students, faced considerable challenges in mitigating stressors due to their demanding academic responsibilities. Throughout the study duration, they encountered psychosocial stressors that were known to provoke cortisol fluctuations. Our hypothesis suggests that chronic stress may provoke the HPA axis activation, potentially leading to hypercortisolemia or a blunted diurnal cortisol rhythm. Extended periods of elevated cortisol are neurotoxic, particularly affecting the hippocampus, and disrupt the feedback mechanisms regulating the HPA axis. Such dysregulation can result in emotional instability, cognitive impairments, and an increased vulnerability to depressive symptoms. The relationship between chronic stress and HPA axis overstimulation is crucial, leading to significant fluctuations in cortisol levels. 20
Several clinical trials have investigated the efficacy of saffron in regulating cortisol levels during acute stress events. Previous research has indicated a statistically significant difference in the time to reach maximum salivary cortisol concentration (Tmax), as evidenced by a p value of .04 from the Friedman test. Participants who received acute saffron extract supplementation demonstrated an increased Tmax for salivary cortisol compared to those in the placebo group when faced with acute stress. These findings warrant consideration in future studies that assess salivary cortisol levels in response to acute stressors, such as examinations or quizzes. 21
Saffron had demonstrated potential for alleviating symptoms of moderate depression, as assessed by the HDRS questionnaire, but this had only recently been explored among medical students. Generalizing the results of this study to populations with different characteristics should be done with caution. The recent study had a limited 8-week duration and did not account for the psychosocial stressors that affected the participants. However, in this study, in week 4, an unmeasured psychosocial stressor was present, namely, the final exam for the course, which had the potential to bias the research results. The condition of the research population, which had a busy lecture and exam schedule, made it challenging to ensure that students did not experience psychosocial stress during the study. Future research should include serial cortisol measurements in the morning and evening for comparative analysis. Additionally, more extended observation periods and more comprehensive documentation of side effects are necessary. Selecting participants with mild to moderate depression who also exhibit elevated baseline cortisol levels could help standardize the subject population in subsequent studies.
Conclusion
Administration of saffron has been shown to enhance clinical outcomes in individuals with mild to moderate depression, as evidenced by a reduction in depression scores from moderate to mild levels. Nonetheless, further investigation is necessary to fully understand saffron’s effect on salivary cortisol levels, particularly in individuals presenting with elevated baseline salivary cortisol.
Footnotes
Abbreviations
CAR: Cortisol awakening response; ELISA: Enzyme-linked immunosorbent assay; GSH-Px: Glutathione peroxidase; HDRS: Hamilton Depression Rating Scale; HPA: Hypothalamic–pituitary–adrenal; PHQ-9: Patient Health Questionnaire-9; RCT: Randomized controlled trial; SOD: Superoxide dismutase; SSRIs: Selective serotonin reuptake inhibitors; TCAs: Tricyclic anti-depressants; Tmax: Time to reach maximum salivary cortisol concentration.
Acknowledgments
The authors acknowledge Farhamna Academic for assisting in the preparation of this manuscript. The authors also acknowledge the staff at our institution who assisted in data collection and acquisition.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
The Institutional Ethics Committee approved all procedures (reference number: 644/UN4.6.4.5.31/PP36/2024). Written informed consent was obtained from all the participants before enrollment. All data of the participants were strictly maintained and kept confidential and anonymous.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Trial Registry
The study is registered with the Research Registry under the number