
Abstract
Background
Autoimmune and inflammatory diseases, such as rheumatoid arthritis, multiple sclerosis, inflammatory bowel disease, and psoriasis, are typified by immune dysregulation resulting in chronic inflammation and progressive tissue injury. Standard treatments, including corticosteroids, non-steroidal anti-inflammatory drugs, and disease-modifying anti-rheumatic drugs, are often of limited efficacy, have significant side effects, and are challenged by drug resistance.
Purpose
This narrative review discusses new pharmacotherapeutic approaches to autoimmune and inflammatory diseases with a focus on biologic drugs, small-molecule inhibitors, gene therapy, and nanotechnology drug delivery systems.
Materials and Methods
A systematic literature search was performed using PubMed, Scopus, and Web of Science, covering clinical trials, pharmacological advances, and expert reviews of the past decade. The review highlights trends in immunotherapy, biomarker-stratified treatment selection, and new therapies for autoimmune diseases.
Results
Biologic drugs, including tumor necrosis factor-alpha inhibitors, interleukin-17 inhibitors, and Janus kinase-signal transducer and activator of transcription inhibitors, have shown pertinent increases in disease remission rates and lowered systemic toxicity. However, constraints include high cost, resistance, and restricted access. Small-molecule inhibitors and precision immunotherapies enable patient-specific treatments with enhanced efficacy, but resistance and accessibility are significant hurdles. Breakthroughs in nanomedicine, clustered regularly interspaced short palindromic repeats-CRISPR associated protein 9 (CRISPR-Cas9) gene-editing, and artificial intelligence-assisted drug discovery hold much promise for overcoming these issues and providing more efficient and targeted treatments.
Conclusion
Precision pharmacotherapy has transformed autoimmune disease treatment by providing mechanism-based, patient-specific approaches. Future studies should aim to improve biomarker-guided therapies, enhance drug accessibility, and incorporate AI-based innovations to maximize clinical outcomes.
Introduction
Autoimmune and inflammatory disorders, including rheumatoid arthritis (RA), multiple sclerosis (MS), inflammatory bowel disease (IBD), psoriasis, and systemic lupus erythematosus (SLE), are a growing global burden, with millions of people suffering worldwide. 1 These diseases are expressions of immune dysregulation, wherein the body’s immune apparatus would attack its tissues and lead to chronic inflammation and irreversible organ damage. 2 The pathogenesis of these diseases is multifactorial, with interplays between genetic, environmental, and immune factors, necessitating treatment modalities that are multidisciplinary in approach. Though overuse of traditional modalities such as corticosteroids, non-steroidal anti-inflammatory drugs (NSAIDs), and disease-modifying anti-rheumatic drugs (DMARDs) is a widespread practice, their long-term effectiveness is often suboptimal, necessitating more targeted and individualized therapeutic modalities. 3
Traditionally, autoimmune diseases have been treated with non-selective immunosuppressives that, despite their efficacy in managing acute inflammation, yield side effects like osteoporosis, cardiovascular disease, and susceptibility to infections. 4 They also yield unpredictable patient drug responses, and therefore biomarker-guided precision pharmacotherapy for more effective and targeted treatment. 5
The advances in molecular pharmacology, immunology, and bioinformatics in the recent past have profoundly altered the model of treatment. Biologic therapy, such as tumor necrosis factor-alpha (TNF-α) inhibitors, interleukin-17 (IL-17) inhibitors, and Janus kinase (JAK) inhibitors, has transformed the treatment of disease and achieved targeted immune modulation with reduced systemic toxicity. 6 These therapies have improved remission of such diseases as RA, Crohn’s disease, psoriasis, and ankylosing spondylitis. Oral therapy, such as JAK inhibitors and sphingosine-1-phosphate (S1P) receptor modulators, also provides convenient alternatives to biologics. 7
Among the most exciting new developments in treating autoimmunity are integrating biomarker-directed treatment choice and precision medicine. Genomic, transcriptomic, and proteomic profiling have rendered predictive biomarkers accessible, which makes it possible to treat patients earlier and more precisely. Pharmacogenomic screening has even been utilized to tailor therapy based on genetic polymorphisms that affect drug metabolism and immune function. 8
However, challenges are present in translating these advances into routine clinical practice. Treatment resistance, frequently due to developing anti-drug antibodies (ADAs) or modulation of immune pathways, is a major challenge. 9 Furthermore, the cost of biologics and gene therapies limits their accessibility, especially in low- and middle-income countries. New therapies like nanomedicine, gene-editing technologies like clustered regularly interspaced short palindromic repeats-CRISPR associated protein 9 (CRISPR-Cas9), and RNA therapeutics are being investigated 10 to overcome these challenges.
Nanomedicine has been promising in enhancing drug bioavailability, tissue targeting, and safety profiles, enhancing therapeutic response with reduced toxicity. Similarly, CRISPR-Cas9 and other gene-editing platforms are promising to correct immune dysregulation at the genetic level, with curative treatment in certain autoimmune diseases being a possibility. 11
In the coming years, artificial intelligence (AI) and computational drug design will significantly accelerate the identification of new immunomodulatory drugs. AI can predict drug response from big patient data and optimize treatment protocols, clearing the pipeline between preclinical research and clinical practice. 12 Moreover, research on multi-target combination therapies that simultaneously target multiple pathways of inflammation is an encouraging aspect to improve the durability of treatment and reduce relapse rates. 13
In conclusion, the art of autoimmune pharmacotherapy is undergoing a paradigm shift, powered by precision medicine, molecular pharmacology, and innovative drug delivery systems. The transition from non-specific immunosuppression to biomarker-driven, targeted therapy promises improved patient outcomes with reduced side effects. Future research will address pharmacogenomic applications, optimizing combination therapy, and integrating AI-based models. Interdisciplinary partnerships between academia, the drug industry, and healthcare professionals will be indispensable in translating these advances into daily clinical practice, ultimately optimizing patient quality of life and long-term cure.
Review of Literature
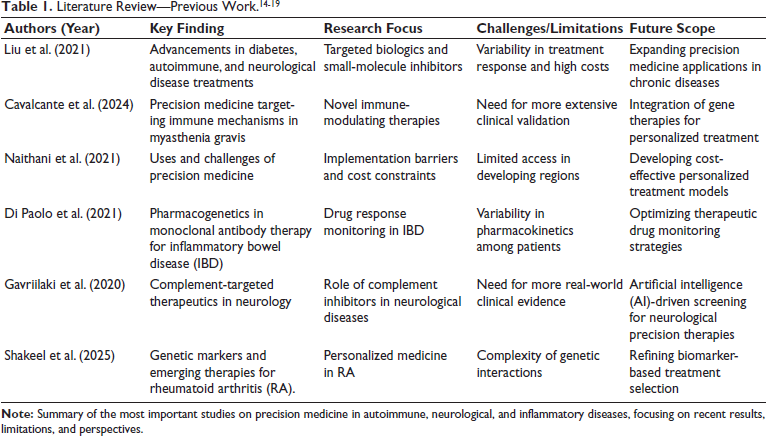
Precision medicine is revolutionizing the treatment of autoimmune, inflammatory, and neurological disorders by personalizing therapy based on genetic and molecular information. Liu et al. emphasized therapeutic advancements in diabetes and autoimmune diseases through targeted biologics and small-molecule inhibitors. 14 Cavalcante et al. wrote on precision medicine in myasthenia gravis, emphasizing novel immune-modulating treatments. 15 Naithani et al. spoke of limitations to personalized medicine, including cost and availability being high. 16 Di Paolo et al. wrote about monoclonal antibody pharmacogenetics in IBD, 17 while Gavriilaki et al. presented complement therapeutics in neurology, 18 Shakeel et al. wrote about new therapies and genetic markers in RA, 19 as shown in Table 1.
Methodology
Locating Data
We conducted a literature search in PubMed, Scopus, Web of Science, and Google Scholar from 2010 to 2024. We searched clinical trials, systematic reviews, and peer-reviewed publications on precision medicine in autoimmune and inflammatory disorders. We also searched clinical guidelines that were relevant to the topic, pharmacovigilance reports, and regulatory guidelines to support the findings.
Inclusion/Exclusion Criteria
The following study types were included: targeted therapy studies, biologics, small-molecule inhibitors, gene therapy, or nanomedicine studies used for autoimmune or inflammatory diseases. Studies published between 2010 and 2024, including clinical trials and preclinical studies, were chosen. Outdated studies, studies with suboptimal clinical data, or studies irrelevant to the therapeutic purpose in this review were excluded.
Data Collection
We ranked research that examined the efficacy of biologics, small-molecule inhibitors, gene therapy, and nanomedicine. Real-world application-based clinical trials, long-term outcomes, and more recent therapeutic advances were particularly highlighted. Regulatory documents, scientific guidelines, and pharmacovigilance reports were also analyzed to present a comprehensive field picture.
Data Extraction
Major information from the selected articles was the mechanisms of action, clinical information, limitations, and future research areas. The strongest preclinical and clinical studies were emphasized, and the duplicate, outdated, and irrelevant studies were excluded from the review.
Integrating Data
Data were qualitatively compared and collated to identify trends in pharmacotherapy, biomarker-guided therapy, and precision medicine challenges. Important findings were tabulated to make it easy to comprehend and signal future research direction.
Results
Advancements in Targeted Biologic Therapies in Autoimmune Diseases
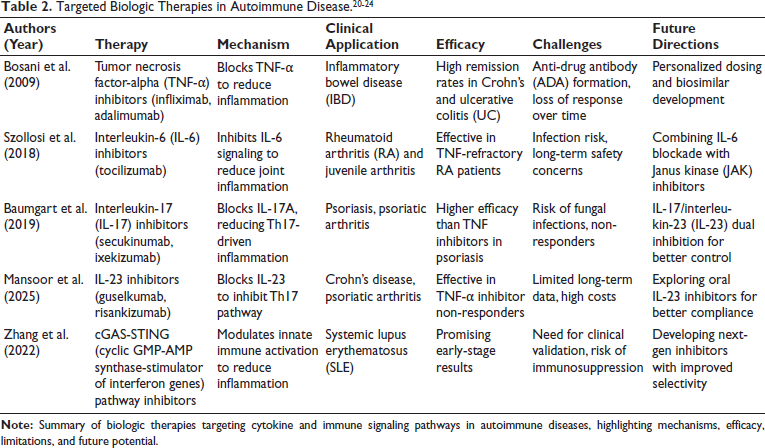
Biologic drugs have revolutionized the treatment of autoimmune diseases through targeted modulation of inflammatory pathways. Monoclonal antibodies (mAbs) that inhibit specific cytokines have been highly effective in RA, MS, IBD, and psoriasis, with better disease control and long-term outcomes than traditional immunosuppressants. 20 TNF-α blockers, such as infliximab and adalimumab, have been extensively used in RA, Crohn’s disease, and ulcerative colitis (UC), with remarkable suppression of inflammation and induction of remission. 21 Their long-term administration is, however, limited by secondary resistance through the generation of ADAs. Interleukin-6 (IL-6) inhibitors, such as tocilizumab, have been effective in RA by inhibiting synovial inflammation and reducing joint damage as a second-line therapy in TNF-refractory patients. 22
IL-17 inhibitors (secukinumab, ixekizumab) are increasingly becoming a cornerstone of treating psoriasis and ankylosing spondylitis since they target Th17-mediated inflammation. Interleukin-23 (IL-23) inhibitors (guselkumab, risankizumab) have extended treatment benefits in psoriatic arthritis (PsA) and Crohn’s disease with increased specificity and duration of action over IL-17 inhibition. 23
Although beneficial, long-term safety risks involve enhanced infection risk, malignancy risk, and cardiovascular disease. Furthermore, resistance to therapy is still a problem, and combination therapy strategies and stratified drug selection based on biomarker stratification are necessary. Next-generation biologics with reduced immunogenicity, improved therapeutic drug monitoring (TDM), and the integration of AI-based precision medicine need to be developed in future research to improve treatment selection, as shown in Table 2. 24
The Place of Small-Molecule Inhibitors in Precision Pharmacotherapy
Small-molecule inhibitors are emerging as potent alternatives to biologics, with the advantage of oral administration and targeted immune modulation. JAK inhibitors, tofacitinib, baricitinib, and upadacitinib, have revolutionized the treatment of RA, PsA, and UC by inhibiting intracellular cytokine signaling pathways. Unlike the extracellular action of biologics on cytokines, intracellular JAK inhibitors inhibit the JAK-signal transducer and activator of transcription (STAT) pathway, inhibiting systemic inflammation and disease progression. 25 Their oral bioavailability and quick action increase comfort and convenience, with better patient compliance than biologic injections. A second category of small molecules, the S1P receptor modulators, such as fingolimod and ozanimod, have revolutionized MS therapy. 26 The drugs inhibit lymphocyte egress from lymphoid tissue, preventing neuroinflammation and rates of disease relapse. Their action, specific for MS, has yielded long-term clinical benefits with an excellent safety profile, with the only caveat being the requirement for monitoring for potential side effects on the cardiovascular system. 27
Oral small-molecule inhibitors are more readily used with biologics because of enhanced patient compliance, dosing flexibility, and lower immunogenicity. However, long-term safety issues, thromboembolic risk, and hepatotoxicity necessitate judicious patient selection and monitoring. Although biologics are the initial treatment of choice for most autoimmune diseases, JAK inhibitors and S1P modulators provide practical alternatives for patients needing non-injectable, target-specific therapy. Future advances to the pinnacle of precision pharmacotherapy will be in next-generation small molecules with enhanced specificity and lower toxicity. 28
Treatment Resistance and Loss of Response Challenges
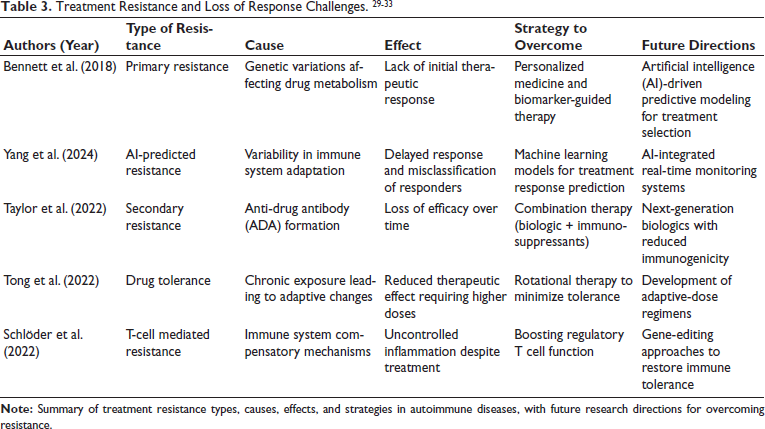
Despite the introduction of biologics and small-molecule inhibitors, therapy resistance is a significant issue in treating autoimmune and inflammatory diseases. The resistance is primary (lack of response from the start) or secondary (loss of response over time). 29 Primary resistance is typically caused by intrinsic disease processes, where the patient is not responsive to initial therapy. Biologics best characterize secondary resistance, where the therapeutic effect is reduced due to immune alterations or drug-neutralizing processes. 30
One of the major causes of secondary resistance to biologics is the formation of ADAs, where the immune system generates neutralizing antibodies against mAbs such as TNF-α inhibitors (infliximab, adalimumab) or IL-6 inhibitors (tocilizumab). This results in reduced drug levels and therapeutic response. In such situations, combination therapy approaches (e.g., immunosuppressants such as methotrexate with biologics) have been reported to reduce ADA formation and extend drug action. 31 In the case of small-molecule inhibitors such as JAK inhibitors (tofacitinib, baricitinib), resistance arises due to intracellular signal modifications that can resist the drug’s mechanism of action. To overcome these challenges, TDM has become an important strategy for maximally individualized treatment. 32 By monitoring trough levels of the drug and ADA levels, physicians can adjust dosing regimens, alter therapy accordingly, and enhance long-term treatment efficacy. The discovery of predictive biomarkers and machine learning (ML)-based response modeling should be the target of future research to obtain maximum precision-based treatment modulation and overcome resistance effectively, as shown in Table 3. 33
New Gene-based Therapies and RNA-based Treatments
The emergence of gene therapies is transforming the management of autoimmune disorders with very targeted, long-term treatments by modulating genetic and molecular pathways of immune dysregulation. CRISPR-Cas9 gene editing is beneficial in manipulating immune cell function to facilitate the correction of genetic mutations leading to autoimmune diseases such as type 1 diabetes, RA, and MS. With the direct manipulation of disease genes, CRISPR technology provides a curative treatment rather than symptomatic relief. 34
Along with gene editing, RNA therapeutics such as small interfering RNA (siRNA) and microRNA (miRNA) therapies are investigated to modulate immune signaling pathways. siRNA therapeutics modulate this by downregulating pro-inflammatory cytokine genes, thus reducing the hyperactive immune response in diseases such as SLE and IBD. Similarly, miRNA therapies regulate T-cell differentiation and inflammatory cytokine expression and, thus, have the potential to treat psoriasis and RA. 35 Gene therapies are also being investigated to re-engineer immune tolerance by controlling regulatory T-cells (Tregs) and dendritic cells to suppress autoimmune attacks. Although gene-based therapies are still experimental, clinical trials evaluate their safety, efficacy, and long-term immunological effects. Future advances should focus on minimizing off-target effects, improving delivery mechanisms, and integrating AI-driven predictive modeling to create personalized gene-editing regimens for treating autoimmune disease. 36
Nanomedicine and Modern Drug Delivery Systems
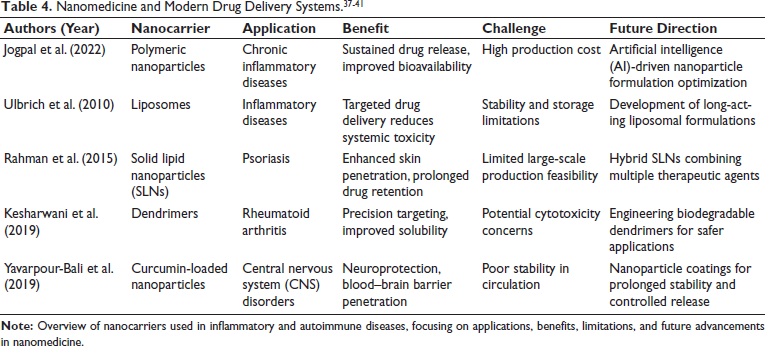
Nanomedicine is revolutionizing the therapy of autoimmune disorders by enhancing drug bioavailability, targeting specificity, and reducing systemic toxicity. Nanoparticles, liposomes, and polymeric micelles are efficient drug carriers, showing sustained release of the drug, increased stability, and improved tissue penetration. 37 For instance, liposomal formulations of immunosuppressants like cyclosporine have demonstrated higher therapeutic efficacy in RA and lupus by offering sustained release of the drug with lower toxicity. Polymeric micelles are involved in solubilizing hydrophobic drugs and delivering poorly soluble immunomodulators. 38
One of the most recent advances in nanomedicine is drug delivery using exosomes, which leverages naturally occurring extracellular vesicles to deliver immunomodulatory drugs. Exosomes can deliver siRNA, miRNA, and therapeutic proteins, allowing targeted immune modulation with low immunogenicity. 39 Investigations show that exosome-based therapies hold promise in treating diseases such as MS, IBD, and type 1 diabetes, offering a cell-targeting, biocompatible solution. Relative to traditional drug formulations, nanomedicine has advantages like longer drug half-life, reduced systemic toxicity, and enhanced penetration into inflamed tissue. 40 Nano-formulated delivery systems also reduce the risk of immune clearance, with longer circulation times and enhanced drug activity. Manufacturing complexities, scale-up issues, and regulatory issues are ongoing limitations to widespread clinical application. The development of low-cost, biocompatible nanocarriers and the integration of AI-based nanotechnology are important research directions required in the future to optimize drug formulation and individualized therapy in autoimmune diseases, as shown in Table 4. 41
Comparative Advances in Autoimmune Pharmacotherapy: From Well-Established Biologic Agents to Emerging Gene and Nanomedicine Technologies
Autoimmune disorders are increasingly being managed with more accurate, precision-guided immune dysregulation-targeting therapy with less systemic toxicity. mAbs have revolutionized therapy by attaining cytokine blockade, specifically by TNF-α, IL-6, IL-17, and IL-23 blockers. 42 Therapeutic agents exhibit better clinical remission, with TNF-α inhibitors attaining up to 39% remission at week 30 in Crohn’s disease and IL-17 inhibitors attaining 82% PASI75 (Psoriasis Area and Severity Index 75% improvement) response in psoriasis, a milestone in cytokine-targeted therapy. 43
In tandem, oral immunomodulators like JAK inhibitors and S1P modulators augmented treatment options with targeted intracellular signal blockade. JAK inhibitors have shown a 59% ACR20 (American College of Rheumatology 20% improvement) response in RA at week 24, offering an injectable biologic substitute with improved adherence and dosing flexibility. 44 However, resistance mechanisms, specifically ADAs, are problematic, limiting long-term efficacy. TDM and combination therapies with immunosuppressants are pivotal in the resistance and regimen tailoring. 45 Novel gene-editing platforms like CRISPR-Cas9 and RNA therapeutics (siRNA/miRNA) open new possibilities by directly editing immune regulatory networks. These preclinical interventions promise durable, mechanism-specific treatments, though clinical integration remains nascent. 46 Finally, nanocarrier-based delivery of drugs by liposomes, polymeric micelles, or exosomes offers promising improvements in tissue-specific targeting, bioavailability, and safety. Nanomedicine enables prolonged drug half-life and localized delivery, which is of great potential in overcoming systemic toxicity and resistance to treatment. These pharmacotherapeutic advances herald a transition to individualized, high-precision autoimmune disease management. 47
Emerging Technologies
Nanomedicine and AI are revolutionizing autoimmune disease therapy. Nanomedicine, with nanocarriers like liposomes and polymeric micelles, is under experimental investigation, with preclinical trials showing good efficacy in enhancing drug bioavailability and targeting. 48 However, manufacturing complexity and regulatory hurdles still hamper wide clinical application. AI, especially drug discovery and biomarker-directed therapy, is advancing rapidly, with various ML models used to forecast drug response and individualize treatment regimens. Although AI-assisted clinical applications are still in the pipeline, it is very promising for personalized medicine. 49
Limitations and Challenges of Therapies for Autoimmune Diseases
While significant improvements have been made in treating autoimmune disorders, some limitations exist. Primary and secondary drug resistance is significant, typically due to developing ADAs or genetic variability among the patients. Cost is another significant limitation because the biologic drugs and gene-based therapies are not inexpensive. Therefore, the accessibility is limited among patients, particularly from low- and middle-income nations. Logistical, regulatory, and healthcare infrastructure limitations also hinder access to these newer therapies; hence, timely treatment and prolonged care are challenging for most patients globally. These limitations need to be overcome by innovation in affordable therapy and enhanced healthcare access.
Directions of the Future in AI-Based Drug Discovery and Personalized Medicine
ML and AI are revolutionizing drug discovery and precision medicine with new ways of discovering drug targets, rationalizing therapeutic regimens, and patient stratification. AI platforms analyze large-scale biological data to predict drug–target interactions, molecular binding affinities, and off-target effects to discover new drug candidates. This has accelerated new immunomodulator discovery for autoimmune diseases with enhanced drug development efficiency. 50 The most substantial use of AI in precision medicine is biomarker-directed therapy choice. Computer-based AI-powered algorithms consider genomic, proteomic, and metabolomic information to determine which treatment to use in each patient. An example is where ML processes cytokine profile data in RA or MS and chooses treatment using TNF-α inhibitors, IL-6 inhibitors, or JAK inhibitors based on personalized patient immune reaction. This cuts down on trial-and-error, improves efficacy, and minimizes side effects. 51
AI also plays an active role in designing combination therapies for multiple targets by simulating drug interactions and synergies. Network-based AI models also determine the optimal drug pair for autoimmune diseases, including coupling JAK inhibitors with biologics to avoid drug resistance. 52 Deep learning approaches also optimize drug repurposing strategies, enabling accelerated discovery of known drugs with novel immunomodulatory activity. With further development of AI technologies, it will be essential to integrate AI into clinical decision-making, reinforce regulatory environments, and streamline data standardization to maximize its potential in precision pharmacotherapy. AI-aided diagnostics, drug development, and real-time treatment optimization are areas where future research needs to be focused on personalizing further and optimizing autoimmune disease management. 53
Discussion
The field of autoimmune and inflammatory diseases has been revolutionized by the arrival of precision medicine and targeted pharmacotherapy. Traditional therapy, in the form of corticosteroids, NSAIDs, and non-specific immunosuppressants, has remained the backbone of therapy for many decades. 54 Their non-specific mechanism of immunosuppression has, however, led to untoward effects of severe nature, such as infections, metabolic derangement, and cardiovascular risk, prompting the creation of newer, more targeted, mechanism-based therapies. Biologic agents, small-molecule inhibitors, gene therapy, nanomedicine, and AI-guided drug discovery are transforming the scene of autoimmune pharmacotherapy with higher efficacy, safety, and individualization of the choice of therapy. 55
One of the most successful advancements in treating autoimmune diseases has been creating biological agents, particularly mAbs directed against inflammatory cytokines. The TNF-α inhibitors (infliximab, adalimumab) have revolutionized the management of RA, Crohn’s disease, and UC, but the development of ADA has resulted in loss of effect and failure of treatment over time. 56 More recently, IL-6 inhibitors (tocilizumab), IL-17 inhibitors (secukinumab), and IL-23 inhibitors (guselkumab) have shown greater efficacy in PsA and ankylosing spondylitis with greater specificity and durability. Nonetheless, despite their benefits, biologics are expensive, restricting access in low- and middle-income countries, and long-term immunosuppression carries the risk of increased risk of infection and development of malignancy. 57
In contrast, small-molecule inhibitors, particularly JAK inhibitors (tofacitinib, baricitinib, upadacitinib), have emerged as adequate oral substitutes for biologics by directly suppressing intracellular immune dysregulation signaling pathways. In contrast to biologics, which block extracellular cytokines, JAK inhibitors block intracellularly, with greater dosing flexibility and a broader immunomodulatory window. 58 Another important class, S1P receptor modulators (fingolimod, ozanimod), has shown outstanding efficacy in MS by blocking autoreactive lymphocytes from entering the central nervous system (CNS). Although small-molecule inhibitors offer greater patient compliance and lower immunogenicity than biologics, long-term safety concerns, including thromboembolism, hepatotoxicity, and cardiovascular risk, need constant monitoring and patient-individualized risk stratification. 59
A long-standing problem in autoimmune pharmacotherapy is resistance to treatment, which can be classified as primary (lack of response from the start) or secondary (worsening response over time due to immune adaptation). Secondary resistance in biological therapy is typically associated with ADA formation, which eliminates the therapeutic activity of mAbs. Combination therapy strategies, including methotrexate co-administration with TNF inhibitors, have been investigated to reduce ADA formation and extend therapeutic duration. Resistance mechanisms in small-molecule therapies include intracellular pathway modifications, reducing drug sensitivity. 60 One of the most significant developments in overcoming resistance is TDM, which allows personalized dose adjustment based on drug levels and immune response markers. TDM has helped optimize biologic and small-molecule therapy, allowing dose optimization, early intervention on response loss, and personalized treatment regimens. 61
In addition to conventional therapies, gene-based and RNA-based medicines are revolutionizing the treatment of autoimmune diseases. CRISPR-Cas9 gene editing has been explored as a potentially therapeutic strategy in autoimmune disease, with the potential to modulate immune dysregulation at the gene level precisely. With gene editing in genes linked to immune hyperactivation, CRISPR holds promise in autoimmune diseases such as type 1 diabetes, SLE, and IBD. Further, RNA-based therapy, including siRNA and miRNA therapy, has been shown to modulate cytokine signaling, regulate immune pathways, and suppress autoimmunity. Therapeutically beneficial, gene-based treatments are not without problems regarding off-target effects, delivery efficiency, and regulatory approval and consequently require further study before widespread clinical use. 62
Another breakthrough in precision medicine technology is nanomedicine, which utilizes nanoparticles, liposomes, and polymeric micelles to enhance drug bioavailability and targeting specificity. Traditional immunosuppressive therapies are marred by compromised pharmacokinetics, systemic toxicity, and ineffective drug penetration into inflamed tissues. Liposomal formulations of drugs, for example, liposomal cyclosporine, have improved drug stability, controlled release, and reduced toxicity in autoimmune diseases. 63 Polymeric micelles and nanocarriers are being developed to offer site-specific drug delivery, particularly in neuroinflammatory conditions like MS. Breakthrough technology in nanomedicine is exosome-based drug delivery, which utilizes extracellular vesicles for therapeutic payload delivery and immune evasion. Exosome-based therapies are being explored for precision-targeted immune modulation, a potential alternative to traditional drug formulations. 64
AI and ML are game-changers for autoimmune drug discovery. AI-driven algorithms accelerate drug target identification, biomarker discovery, and therapeutic optimization. AI models can utilize large-scale patient data to predict individual treatment responses, optimize biomarker-based stratification, and enhance combination therapy strategies. 65 Deep learning models are being applied to predict synergistic drug combinations, enabling the design of multi-targeted therapies to bypass resistance mechanisms. AI-driven virtual screening also accelerates the discovery of new immunomodulators, with significant time and cost reductions in drug development. 66
Despite these advances, several challenges must be overcome before precision pharmacotherapy is implemented in clinical practice. High cost is the most significant access hurdle for biologics, gene therapies, and nanomedicine-based products. In addition, the lack of long-term safety data on new treatments, such as RNA-based drugs and CRISPR gene editing, raises regulatory and ethical issues. 67 With the evolution of precision medicine, future research must tackle the generation of cost-efficient, scalable treatments, refinement of biomarker-driven treatment algorithms, and implementation of AI-based precision medicine models in daily clinical practice. 68
In short, the pharmacotherapy of autoimmune disorders is now being redefined, shifting away from immunosuppressive, broad-spectrum therapy to very specific, highly individualized treatment approaches. Biologics, small-molecule inhibitors, gene therapy, nanomedicine, and AI-assisted drug discovery are rewriting the treatment plan with increased efficacy, safety, and personalized selection of therapy. 69 Overcoming resistance to treatment, maximizing combination regimens, and increasing access worldwide will be critical in driving equitable patient outcomes. As science advances, the convergence of AI and precision medicine technologies will bring a new age of personalized autoimmune disease treatment, ultimately leading to improved long-term disease control and patient quality of life. 70
Conclusion
Biomarker-directed precision pharmacotherapy transforms autoimmune disease treatment by enabling targeted, patient-specific treatment strategies. Genomic, proteomic, and transcriptomic data integration enables biomarkers to guide therapy choice, ensuring greater efficacy and fewer adverse effects. Despite the unprecedented advances, challenges remain to overcome drug resistance, particularly secondary resistance due to ADAs and immune system modulation. In addition, the exorbitant cost of biologics and gene-based therapies limits their widespread access, especially in low- and middle-income countries. With new therapies such as nanomedicine and gene editing tools on the horizon, future research must focus on biomarker optimization, making treatments less expensive and more accessible. Furthermore, incorporating AI-driven predictive models for real-time treatment optimization and exploring combination therapy will provide more personalized, effective management strategies. Closing the gap between new therapies and practical clinical use will be essential to optimizing long-term patient outcomes and global healthcare parity.
Key Takeaways
Precision medicine is revolutionizing autoimmune disease therapy with biologics, small-molecule inhibitors, and gene-based therapies to offer targeted immune modulation with enhanced efficacy and safety. Nanomedicine is improving drug bioavailability, and AI-facilitated drug discovery is streamlining the process of developing treatments and biomarker identification. Treatment resistance, ADA production, and high cost remain some challenges, necessitating TDM and combination therapy. Future development must address cost-effective individualized therapy, optimal utilization of gene editing, and AI-aided clinical decision-making to reduce the cost of treatments and long-term benefits to the patients.
Footnotes
Abbreviations
ACR20, American College of Rheumatology 20% improvement; ADA, anti-drug antibodies; AI, artificial intelligence; cGAS-STING, cyclic GMP-AMP synthase-stimulator of interferon genes; CNS, central nervous system; CRISPR-Cas9, clustered regularly interspaced short palindromic repeats-CRISPR associated protein 9; DMARDs, disease-modifying anti-rheumatic drugs; IBD, inflammatory bowel disease; IL-6, interleukin-6; IL-17, interleukin-17; IL-23, interleukin-23; JAK, Janus kinase; mAbs, monoclonal antibodies; miRNA, microRNA; ML, machine learning; MS, multiple sclerosis; NSAIDs, non-steroidal anti-inflammatory drugs; PASI75, Psoriasis Area and Severity Index 75% improvement; PsA, psoriatic arthritis; RA, rheumatoid arthritis; S1P, sphingosine-1-phosphate; siRNA, small interfering RNA; SLE, systemic lupus erythematosus; SLNs, solid lipid nanoparticles; STAT, signal transducer and activator of transcription; TDM, therapeutic drug monitoring; TNF-α, tumor necrosis factor-alpha; Tregs, regulatory T-cells; UC, ulcerative colitis.
Acknowledgments
The authors appreciate the work of researchers whose studies have shed light on precision pharmacotherapy. They further thank their respective institutions for their facilitation of this review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This peer-reviewed established literature-based narrative review did not involve human or animal subjects. No collection or analysis of new clinical data was conducted; therefore, no ethical approval was necessitated. The research complies with the ethical guidelines for scientific integrity and responsible reporting of biomedical research.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.