
Abstract
Chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) is a rare yet debilitating neuropathy characterized by chronic inflammation, demyelination, and axonal degeneration. Current treatments, including corticosteroids, intravenous immunoglobulins, subcutaneous immunoglobulins, and plasma exchange, often result in inadequate responses and relapse. Efgartigimod, a novel Fc receptor (FcRn) blocker, has emerged as a promising therapy by reducing pathogenic autoantibodies. Recent clinical trials, particularly the ADHERE and ADVANCE-CIDP studies, demonstrate its efficacy in prolonging clinical response and reducing relapse rates. This review explores CIDP’s pathogenesis, current treatments, and the potential of efgartigimod to revolutionize the management of this challenging condition.
Keywords
Introduction
Chronic inflammatory demyelinating polyradiculoneuropathy (CIDP), the chronic counterpart of Guillain–Barré syndrome (GBS), is a rare and complex neuropathy with an estimated annual incidence ranging from 0.15 to 1.6 cases per 100,000 population. This disorder presents heterogeneously, in a variegated course.1, 2 Despite its rarity, CIDP impacts a substantial proportion of the population, with a reported worldwide prevalence of 0.67–10.3 per 100,000 and a unique male-predominant profile having a 2:1 male-to-female ratio.3–5 The disease accounts for an appreciable proportion of all chronic polyneuropathies, resulting in its marked contribution to neuropathic morbidity.
Evolving over a minimum of 8 weeks, CIDP typically presents with progressive muscular weakness of limbs, more pronounced in the distal extremities.1, 2 Patients initially experience hand muscle weakness, foot drop, and difficulty with motor tasks, progressing to involve the shoulder and hip girdle.1–3 Sensory symptoms include paresthesia and compromised vibration detection; motor symptoms are more dominant, affecting motor fibers, particularly the larger and proximal fibers.1, 5 Interstitial abnormalities include endoneurial edema and inflammatory cell infiltrates.
The complex pathogenesis of CIDP can be attributed to two distinct mechanisms.6, 7 One of these is the impaired myelin sheath reconstitution due to recurrent demyelination and remyelination. This can be explained by the disease’s tendency to demyelinate the nerves at the paranodal region, prompting remyelination by Schwann cells. However, the remyelinated segments are short with thinner myelin sheaths, leading to the hallmark pathological manifestation of onion bulbs.6, 7
Recent studies have validated the 2021 European Academy of Neurology/Peripheral Nerve Society (EAN/PNS) updated guidelines as the standardized diagnostic criteria to verify CIDP. 8 The approach involves clinical evaluation, electrodiagnosis, and lab testing with exclusion criteria. Electrodiagnosis relies on specific indications in at least two nerves. Additional investigations can be supportive. Moreover, an objective response to treatment, cerebrospinal fluid (CSF) analysis, and nerve biopsy findings can hold confirmatory status. 9
Despite the availability of numerous conventional therapeutic regimes (i.e., corticosteroids, intravenous immunoglobulins (IVIg), and plasma exchange), inadequate response to treatment and symptomatic relapse of the disease have been common complaints of a significant number of CIDP patients. 10 This prompts the scientific community to dive deeper into the exploratory realm of novel therapeutic strategies. Efgartigimod is a promising new agent in the treatment landscape for CIDP. It is a recombinant human immunoglobulin G (IgG1) fragment crystallizable (Fc) fragment that targets and inhibits the neonatal Fc receptor (FcRn)—playing a critical role in recycling IgG antibodies. By reducing the levels of pathogenic autoantibodies, efgartigimod aims to mitigate the autoimmune component underlying CIDP and improve patient outcomes. 11
This short communication explores the emerging evidence supporting the efficacy of efgartigimod in managing CIDP, highlighting recent clinical trial results and discussing its potential impact on future treatment paradigms for this challenging condition.
Current Treatment Landscape
Several therapeutic modalities, each with a unique mechanism of action (MOA), and challenges have shown varying degrees of efficacy while treating CIDP. IVIg functions through a variety of mechanisms. 12 IVIg data from several randomized controlled trials (RCTs) demonstrate variable results and short-term efficacy compared to corticosteroids. Utilizing a similar MOA to IVIg, subcutaneous immunoglobulins (SCIg) proved their practical superiority with fewer adverse effects and their ability to be administered at home, being on par with IVIg for patients new to therapy.13, 14 SCIg was approved by the Food and Drug Administration (FDA) in 2018 for use as maintenance therapy in adult patients with CIDP, based on the findings of the polyneuropathy and treatment with Hizentra (PATH) study. 15 Global studies confirm SCIg’s effectiveness in avoiding relapse, with a 12-week RCT particularly highlighting gains in strength of handicap due to this innovative therapy. 16 In addition to this, studies provide strong support for the use of SCIg as an effective maintenance therapy for CIDP, demonstrating comparable efficacy to IVIg with respect to relapse rates and clinical outcomes. SCIg offers notable benefits, including a reduced incidence of adverse events, improved quality of life, and a higher patient preference, attributed to factors such as the ability to self-administer at home, greater convenience, and fewer treatment-related fluctuations. While both SCIg and IVIg contribute to the maintenance or improvement of neuromuscular function, SCIg is associated with a lower risk of adverse events and presents potential cost-saving advantages. 17 Moreover, plasma exchange, another treatment option where plasma detoxification occurs, has shown short-term effectiveness, often necessitating the use of corticosteroids or IVIg as concurrent therapy, especially in refractory instances.18–20
While there is a scarcity of literature favoring immunosuppressants in CIDP, drugs like azathioprine, methotrexate, cyclosporine, and mycophenolate mofetil continue to be widely used for immune response suppression; for refractory instances, rituximab and cyclophosphamide are reported to work well.21, 22 A more drastic therapeutic methodology is stem cell transplantation to reset the immune system. This invasive technique, called “autologous stem cell transplantation,” is considered risky due to the morbidity and death associated with it. However, studies found high rates of treatment-free remission following this surgical approach. 23
Drug classes like FcRn blockers are effective against CIDP as they reduce the serum lifespan of pathogenic antibodies. 12 The intent of neonatal Fc receptor-targeted therapeutics is to precisely target FcRn employing a variety of strategies, including monoclonal anti-FcRn antibodies or Fc fragments. 24 By inhibiting the IgG recycling pathway, these methods expedite the breakdown of autoantibodies. 24 It suppresses the amounts of pathogenic autoantibodies along with total plasma immunoglobulin levels without altering the levels of immunoglobulins A, E, M, or D, the other immunoglobulin subclasses. 24 Efgartigimod, rozanolixizumab, batoclimab, and nipocalimab are medications that block FcRn. These drugs can be given subcutaneously or intravenously. 24 Adverse effects that have been reported include diarrhea, pyrexia, nausea, upper respiratory tract infections, urinary tract infections, and headaches (more frequently reported with efgartigimod and rozanolixizumab). Notably, batoclimab and nipocalimab have been related to transient hypoalbuminemia and hypercholesterolemia. 24 Rozanolixizumab was observed to be safe and well-tolerated in a clinical trial (NCT03861481); however, because of its high rate of placebo stability, it was not effective in treating CIDP patients. 25 Efgartigimod is considered more potent in lowering the chance of disease recurrence. 12
Classical complement inhibition drugs like SAR445088 reduce downstream complement activation by primarily inhibiting the C1-complex, which may stop inflammatory processes linked to CIDP. 12 Since 2021, an open-label, non-randomized phase 2 study (NCT04658472) has been ongoing to assess the safety, efficacy, and tolerability of SAR445088 in 90 patients with CIDP. 12
Bruton tyrosine kinase (BTK) inhibitors prevent B-cell maturation, which could decrease the generation of harmful autoantibodies. 12 BTK is a non-receptor protein-tyrosine kinase relating to the TEC family of kinases. When the B-cell receptor (BCR) is activated, the SRC-family kinase LYN phosphorylates BTK, subsequently phosphorylating its substrate, the downstream molecule phospholipase C-γ2. It builds intracellular calcium levels and activates transcription factors that are vital for B-cell survival, differentiation, and proliferation. 26 In cases of immune-mediated disease, it may have therapeutic benefits. Waldenström’s macroglobulinemia and chronic lymphocytic leukemia are now treated with BTK inhibitors. 12 Only one case series highlights the successful use of the BTK inhibitor ibrutinib to treat patients with anti-myelin-associated glycoprotein (MAG) neuropathy, emphasizing the current lack of information and expertise in the field of autoimmune neuropathy. In the Netherlands, zanubrutinib and rituximab are presently being used in a phase II single-arm open-label trial for anti-MAG associated polyneuropathy (MAGNAZ) (NCT05939037). No trials are underway in CIDP. 12
ADVANCE-CIDP 1 (NCT02549170) was a multicenter, phase 3, prospective, randomized, double-blind, placebo-controlled study that assessed the safety, effectiveness, and tolerability of facilitated subcutaneous immunoglobulin (fSCIG) 10% as a maintenance treatment to prevent disease recurrence that would cause neuromuscular impairment in CIDP individuals. It was shown that fSCIG 10% was more effective than placebo at preventing relapse of neuromuscular impairment when used as a maintenance therapy in a patient group with stable CIDP receiving intravenous immunoglobulin treatment. Most patients preferred the subcutaneous infusions of fSCIG 10% and placebo over their prior intravenous treatment, and both were well tolerated. 27 The ADVANCE-CIDP 1 study demonstrated that fSCIG 10% significantly reduced the absolute risk of CIDP relapse by 22% compared to placebo, with a lower relapse rate (9.7%) than previously reported for IVIg (13%) and conventional SCIg (19%–33%). Patients receiving fSCIG 10% experienced improved quality of life, high satisfaction with treatment, and preferred subcutaneous infusions over intravenous treatments. The treatment also showed favorable results in functional worsening, motor function, and safety profile, with less frequent systemic reactions and low treatment-induced adverse effects. The study concluded that fSCIG 10% is a promising treatment option for CIDP patients, justifying further evaluation in clinical settings. 27
An open-label, long-term continuation of the phase 3 double-blind, randomized, placebo-controlled ADVANCE-CIDP 1 research, ADVANCE-CIDP 3 (NCT02955355), attempted to evaluate the long-term safety, tolerability, and effectiveness of fSCIG 10%. ADVANCE-CIDP 3 was accessible to patients who had completed 6 months of fSCIG 10% or placebo treatment in ADVANCE-CIDP 1 without encountering a recurrence. The utility of fSCIG 10% as a maintenance treatment for CIDP was further supported by its low recurrence rate and acceptable long-term safety and tolerability. 28
While there are many therapies available, the treatment of choice is selected based on the unique characteristics of the patients as well as their reaction to earlier treatments. Further investigation and clinical studies are essential to improve and extend the existing treatment regime.
Table 1 shows different types of treatment methods for CIDP, which work by targeting different immune mechanisms.
Different Therapeutic Modalities Show Varying Degrees of Efficacy in Treating CIDP.
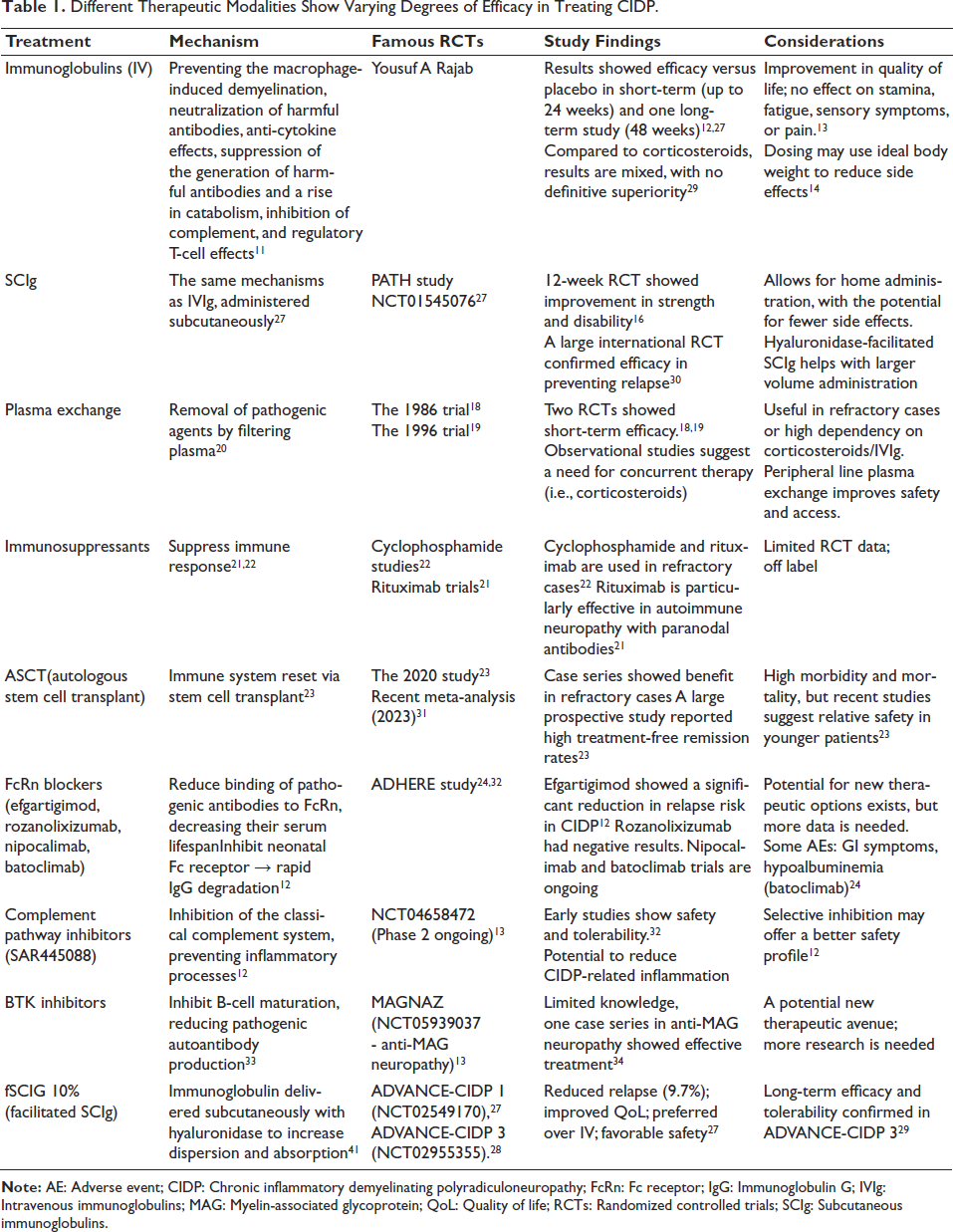
First-line treatments include IVIg and SCIg, which perform their action by modulating harmful antibodies and regulating the immune response. A study conducted by Yousuf A. Rajab, comparing IVIg versus placebo for the treatment of CIDP, demonstrated better quality of life. The PATH study concluded that SCIg has fewer side effects and can be administered at home.
Plasma exchange, a treatment method in which pathogenic factors are removed by plasma, has shown promising results in refractory and high dependency cases. Immunosuppressants like Cyclophosphamide and Rituximab are used off-label in severe or resistant cases. Additionally, autologous stem cell transplant carries a high risk; however, new data suggest that it is safer for younger patients and may induce long-term remission.
Novel therapies include FcRn blockers like efgartigimod, which perform their action by lowering the IgG levels, showing efficacy in relapse prevention. Complement inhibitors and BTK inhibitors represent new approaches; however, the data are limited. ADVANCE-CIDP studies demonstrated that, using hyaluronidase for better absorption, facilitated SCIg has also shown promising results by improving quality of life and reducing relapse; moreover, they provide long-term safety.
Role of Efgartigimod
Efgartigimod, a human IgG1 antibody fragment, decreases circulating immunoglobulins by binding to the neonatal FcRn. Lowering the pathogenic IgG autoantibody levels and recycling, this drug combats CIDP on a pathophysiological level.35–37 A co-formulation of efgartigimod alfa and recombinant human hyaluronidase, going by Vyvgart Hytrulo, has been licensed by the US Food and Drug Administration to treat adults with CIDP. 37 Hyaluronidase, in this combination therapy, works by depolymerizing hyaluronan, increasing the permeability of the subcutaneous tissue. 38
A multicenter study (Study 3; NCT04281472) assessed the efficacy of Vyvgart Hytrulo in treating adults with CIDP. In the open-label phase, 322 patients received subcutaneous injections of Vyvgart Hytrulo (1,008 mg/11,200 units) up to 12 times weekly until two consecutive visits showed significant clinical improvement. Of these, 69% (221 patients) demonstrated improvement and proceeded to the randomized, double-blind, placebo-controlled phase. In this phase, participants received either Vyvgart Hytrulo or a placebo once weekly. Efgartigimod significantly reduced the risk of relapse compared with placebo, with relapses occurring in 27.9% of the Efgartigimod group versus 53.6% of the placebo group. 35
The ADHERE+ trial (NCT04280718) is an open-label extension of the ADHERE trial that endeavors to evaluate the efficacy, safety, and long-term tolerability of efgartigimod PH20 SC in patients with CIDP. About 226 men and women, ages 18 and above, who ended the 48-week ADHERE (NCT04281472) trial’s stage B were recruited for this study and received subcutaneous efgartigimod PH20 treatment. 39 The trial’s results are anticipated because it is scheduled to conclude in 2027.
Side Effects and Safety Profile
According to clinical studies, efgartigimod is a well-tolerated drug with minimal adverse consequences. 40 Most adverse events were mild or moderate in extent. However, consuming Vyvgart Hytrulo could increase the risk of infections, particularly respiratory and urinary tract infections. Blood abnormalities, including low white blood cells, lymphocytes, and neutrophils, were also more common but typically mild to moderate. During trials, patients receiving this therapy experienced hypersensitivity responses such as rash, angioedema (swelling), dyspnea (difficulty breathing), urticaria (itchy welts), and injection site reactions (≥15%). Bruising and erythema at the injection site were the most frequent of these reactions.35, 38
The effect of immunization, particularly with live vaccines, is unclear, so vaccinations should be considered before starting treatment. Hypersensitivity reactions (i.e., rash and anaphylaxis) and infusion-related reactions (i.e., hypertension and chills) have been recorded, prompting close monitoring during use.41, 42 Treatment should be delayed in the presence of an active infection.
Future Direction and Conclusions
This article provides an in-depth analysis of CIDP, focusing on its intricate immune-mediated mechanisms, clinical manifestations, and the challenges in managing the condition. Managing CIDP is challenging due to its varied presentation, complex diagnostic process, and inconsistent response to conventional therapies. Many patients experience relapses despite treatment, and more aggressive approaches, such as stem cell transplantation, carry significant risks, further complicating the management of the disease. The findings highlight the importance of tailored healthcare strategies, acknowledging that a universal therapeutic regimen may not be effectively optimized for all patients.
Among the treatments discussed, efgartigimod stands out, particularly as evidenced by the ADHERE study. This therapy has shown considerable promise in reducing relapse rates and extending clinical response in CIDP patients, which could significantly lessen the disease burden. By focusing on the underlying immune processes, efgartigimod offers a more targeted treatment approach, potentially leading to improved long-term outcomes. Expanding the treatment options available to clinicians, this medical prodigy is a hope for effective and personalized CIDP management.
With this article, we hope to present new insights and potential treatment avenues for this challenging neurological condition. While there remains a need to dive deeper into this uncharted realm, we hope our work helps the broader medical research community to improve patient care and quality of life.
The clinical and therapeutic challenges of CIDP are complex because of its variable response to standard therapies, diagnostic complexity, and heterogeneity in presentation. Although many patients find symptom relief from treatments like IVIg, corticosteroids, and plasma exchange, a small percentage of patients continue to relapse or show insufficient improvement, highlighting the need for more focused and long-lasting solutions.
With early data indicating positive results in lowering relapse rates and extending response, efgartigimod, an FcRn blocker, represents a novel approach in CIDP therapy. Its function must be viewed in the context of a more comprehensive therapeutic approach, which includes newer alternatives such as BTK inhibitors and complement pathway inhibitors (e.g., SAR445088), which may provide different ways to influence the immune response.
Although efgartigimod exhibits enormous potential, complement pathway inhibitors, such as SAR445088, present a viable substitute by blocking C1-complex activation and so reducing inflammatory cascades. By stopping B-cell maturation, BTK inhibitors might additionally reduce the formation of autoantibodies. Early trials in comparable autoimmune neuropathies suggest potential cross-applicability, notwithstanding the scarcity of data on their usage in CIDP. To identify the best order or mix of these treatments, comparative research will be required.
According to the study, transthyretin (TTR) was elevated in CIDP patients’ CSF, which raises the possibility that it could be used as a diagnostic biomarker. TTR was noticeably elevated in CIDP, even though it has also been changed, often downregulated, in other disorders such as GBS and neurodegenerative pathologies. TTR serves as a carrier for thyroxine and vitamin A, is mostly made in the choroid plexus, and may be involved in nerve regeneration. However, TTR lacks disease specificity because it is present in various disorders. 43
Other proteins, such as pro-apolipoprotein, transferrin, and haptoglobin, were also found; however, these are also frequently seen in a variety of neurological conditions. Their existence could be an indication of similar disease processes or sensitivity limitations in detection.
Cost-effectiveness studies are also essential as biologics and advanced treatments proliferate. Clinical decisions will be more sustainable and well-informed if the economic impact of each treatment is assessed in addition to its clinical effectiveness. Healthcare policy and reimbursement strategies can be guided by tools like budget impact models and quality-adjusted life years (QALYs).
In conclusion, mechanistic understanding, innovative therapeutic approaches, and the move toward individualized care are driving CIDP management into a transformative era. In order to improve treatment paradigms and outcomes for all patients with CIDP, future research should concentrate on integrating these components.
Footnotes
Abbreviations
AE: Adverse event; ASCT: Autologous stem cell transplantation; BCR: B-cell receptor; BTK: Bruton tyrosine kinase; CIDP: Chronic inflammatory demyelinating polyradiculoneuropathy; CSF: Cerebrospinal fluid; FcRn: Fc receptor; fSCIG: Facilitated subcutaneous immunoglobulin; GBS: Guillain–Barré syndrome; Ig: Immunoglobulin; IVIg: Intravenous immunoglobulin; PH20: Recombinant human hyaluronidase; QALY: Quality-adjusted life year; QoL: Quality of life; SCIg: Subcutaneous immunoglobulin; TTR: Transthyretin.
Author Contributions
All authors contributed equally.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.