
Abstract
Background
Epilepsy affects around 70 million people worldwide, with a higher prevalence in developing countries like Malaysia. Antiepileptic drugs (AEDs) such as carbamazepine, phenobarbitone, valproic acid, and phenytoin are essential for managing epilepsy, but their pharmacokinetic variability requires precise monitoring. Limited local data underscore the need to optimize therapeutic drug monitoring (TDM) practices in Malaysia to improve therapeutic outcomes.
Purpose
This study evaluates the associations between TDM indications (breakthrough seizure, dosing adequacy, compliance, and suspected toxicity) and plasma concentrations of four commonly used AEDs to guide drug therapy in epilepsy management.
Materials and Methods
A retrospective, case-control study was conducted over 1 year in a tertiary care hospital, including patients on AEDs requiring TDM. Plasma drug levels were analyzed in relation to breakthrough seizures, dosing adequacy, compliance, and suspected toxicity. Statistical analysis was performed using SPSS, focusing on descriptive statistics and odds ratios with 95% confidence intervals.
Results
A total of 780 samples were analyzed, revealing significant variations in plasma concentrations of AEDs relative to TDM indications. Carbamazepine had the highest proportion within the therapeutic range (78.9%), followed by phenobarbitone (61.3%). Valproic acid and phenytoin had lower therapeutic range proportions (40.6% and 18.1%, respectively). Non-compliance with carbamazepine impacted outcomes, while phenytoin and valproic acid were strongly linked to toxicity.
Conclusion
The study emphasizes the importance of TDM in epilepsy management, particularly for optimizing dosages and monitoring compliance and toxicity. It suggests that Malaysian TDM guidelines should focus on more frequent monitoring of AEDs like phenytoin and valproic acid, which show higher rates of sub-therapeutic and toxic levels. These insights could improve AED therapy and patient care in Malaysia.
Introduction
Epilepsy is a chronic brain disorder marked by recurrent seizures. Idiopathic epilepsy has no identifiable cause, while secondary epilepsy results from factors such as brain injury, stroke, prenatal damage, brain tumors, infections, genetic disorders, high fever, dementia, or substance abuse. Epilepsy triggers include lack of sleep, illness, stress, bright lights, caffeine, alcohol, medications, irregular meals, and certain food ingredients.1–4 Around 70 million people worldwide have epilepsy, with a higher prevalence in developing countries like Malaysia.5, 6 In Malaysia, the lifetime epilepsy prevalence is 7.8 per 1,000. 7 Seizures vary in severity, and pharmacotherapy controls seizures in about 70% of patients. First-generation antiepileptic drugs (AEDs) such as carbamazepine, phenobarbitone, valproic acid, and phenytoin require therapeutic drug monitoring (TDM) due to their narrow therapeutic windows and complex pharmacokinetics. These drugs manage seizures, bipolar disorder and status epilepticus.3, 8
Carbamazepine has significant inter-individual plasma half-life variation due to autoinduction. Phenytoin undergoes saturable elimination, requiring careful dosage to avoid neurotoxicity.9–12 Phenobarbitone is effective but often second-line due to sedative effects. Valproic acid has an unpredictable dose-plasma concentration relationship and a short half-life while inhibiting enzymes.9, 13, 14 Most AEDs are ineffective for specific seizure types, making accurate diagnosis crucial. Treatment starts with monotherapy, gradually increasing the dose, followed by the potential substitution or addition of a second AED. Long-term therapy may involve two or three AEDs.8, 15 Pharmacokinetic parameters for these drugs are in Table 1.
Pharmacokinetics Parameters of Carbamazepine, Phenobarbitone, Phenytoin, and Valproic acid.
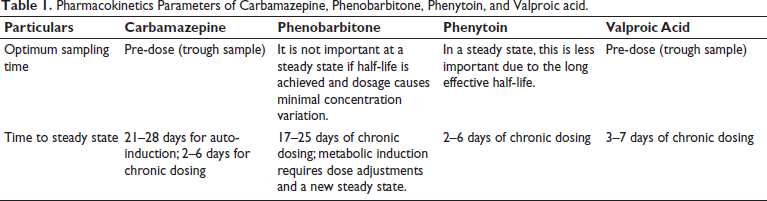
Carbamazepine is used for seizures, bipolar disorder, and trigeminal neuralgia, with a range of 4–12 mg/L. It induces its metabolism, and side effects include rash, hyponatremia, and dizziness. Phenobarbitone treats epilepsy and status epilepticus, with a range of 15–40 mg/L. 16 Its clearance is affected by other AEDs, and side effects include sedation and nystagmus. Phenytoin is used for all epilepsy types except absence seizures, with a range of 10–20 mg/L. Its dose-response is variable, and side effects include neurotoxicity and gingival hyperplasia. Valproic acid is used for epilepsy, bipolar disorder, and migraine prevention, with a range of 50–100 mg/L for seizures. Its clearance is affected by other AEDs, and side effects include hepatotoxicity, pancreatitis, weight gain, and teratogenicity.8, 13, 16
TDM measures drug concentrations in body fluids to guide therapy and prevent toxicity. Drugs with narrow therapeutic ranges are at high risk for toxicity. Pharmacokinetics and drug interactions should be considered when adjusting dosages to achieve optimal therapeutic outcomes.8, 13 In Malaysia, the TDM service managed by pharmacists started in the 1980s.17–19 Pharmacists are involved in managing TDM services and ensuring the optimum use of TDM services. 17
AEDs like carbamazepine, phenytoin, phenobarbitone, and valproic acid have narrow therapeutic indexes, making them prone to toxicity or loss of efficacy.9–12 TDM is essential to study the relationship between dosage, plasma concentration, and pharmacological effects.10, 12 Proper monitoring ensures optimal dosage adjustments for effective seizure control.11, 20 Due to individual variations in pharmacokinetics and pharmacodynamics, AED concentrations may fall outside the therapeutic range without causing harm. TDM is also crucial for monitoring drug interactions in combination therapy.21, 22
Studies in India, Mexico, Switzerland, Iraq, Thailand, and Sabah (in Malaysia) have focused on carbamazepine, phenytoin, phenobarbitone, and valproic acid. They evaluated pharmacist-managed TDM services to achieve optimal seizure control with minimal adverse effects and ensure proper patient care. In India, TDM is used for dosage adjustments, breakthrough seizures, toxicity, poisoning, and non-compliance. 23 In Thailand, it is for compliance, sub-therapeutic concentrations, toxicity, and routine monitoring. 24 In Switzerland, TDM is requested for new therapy, insufficient effect, pharmacokinetic changes, toxicity, drug interactions, and post-seizure checks. 25 In Oman, it is used for side effects, increased seizures, routine checks, and dose titration. 22
The association between plasma concentrations and TDM requests in Malaysia is underreported. While global TDM services improve seizure control and reduce adverse effects, they are underutilized in Malaysia, leading to suboptimal seizure control. Addressing this gap can enhance epilepsy management. Given the diverse demographics and varying healthcare access, TDM is essential for AEDs like carbamazepine, phenytoin, phenobarbitone, and valproic acid. This study aims to identify TDM utilization patterns to improve clinical decision-making and outcomes for Malaysian patients.
Methodology
This 1-year retrospective case-control study in a tertiary care hospital examines the relationship between plasma drug concentrations and TDM indications in AED patients. No therapeutic interventions were made. TDM indications include breakthrough seizures, dosing adequacy, compliance, and suspected toxicity. The study compares patients with and without outcomes, analyzing the correlation between plasma levels and risk factors like sub-therapeutic or toxic concentrations.
Inclusion criteria were patients on phenytoin, valproic acid, carbamazepine, or phenobarbitone, regardless of age or sex, who underwent TDM. Patients on combination therapy were included. Exclusion criteria included incorrect sampling times, samples from other hospitals with inadequate information, and incomplete requests. Sampling times were verified for steady-state levels. 19
TDM request data were collected from the Pharmacy Department, including patient details, medication, dosage, sample timing, drug levels, and pharmacist recommendations. The study tracked the correlation between TDM indications and drug levels (sub-therapeutic, therapeutic, toxic). Extreme plasma levels were verified, and unreliable samples were excluded after reviewing clinical records for errors, such as incorrect timing or drug administration mistakes. Suspect samples were flagged and excluded to ensure valid results and accurate clinical correlations.
Results
A total of 780 samples were studied, with indications for TDM request listed in Table 2. The study revealed significant variations in plasma concentrations of AEDs based on TDM indications, highlighting the complex relationship between drug levels, TDM requests, and clinical outcomes.
Therapeutic Drug Monitoring (TDM) Request Indications and Number of Total Number of Samples.
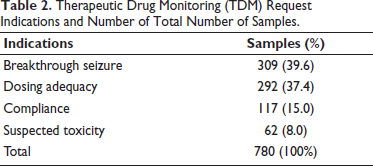
Table 3 shows the association between TDM indications and drug levels for carbamazepine, phenytoin, valproic acid, and phenobarbitone. Carbamazepine had 78.9% within the therapeutic range, and 21.1% sub-therapeutic. Phenytoin showed 18.1% therapeutic, 56% sub-therapeutic, and 25.9% toxic. Valproic acid had 40.6% therapeutic, 52.4% sub-therapeutic, and 7% toxic. Phenobarbitone had 61.3% therapeutic and no toxic levels. These results highlight the need for better monitoring, especially for phenytoin and valproic acid, to optimize seizure control.
Association Between Indication and Measured Drug Levels for Carbamazepine, Phenytoin, Valproic Acid, and Phenobarbitone.
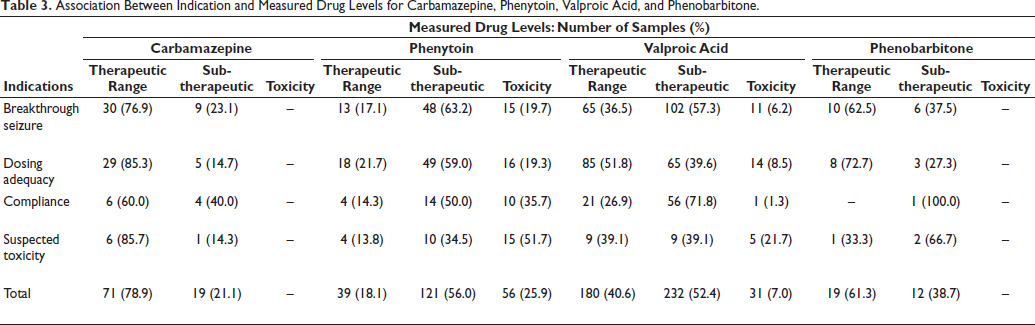
Table 4 shows that of 780 TDM samples, 39.6% were therapeutic, 49.2% sub-therapeutic, and 11.2% toxic. For breakthrough seizures, 38.2% were therapeutic, 53.4% sub-therapeutic, and 8.4% toxic. Dosing adequacy showed 47.9% therapeutic, 41.8% sub-therapeutic, and 10.3% toxic. Compliance was 26.5% therapeutic, 64.1% sub-therapeutic, and 9.4% toxic. Suspected toxicity showed 32.3% therapeutic and 32.3% toxic, indicating a need for better monitoring.
Association Between Indication and Measured Plasma Concentrations Among Four Antiepileptic Drugs (AEDs).
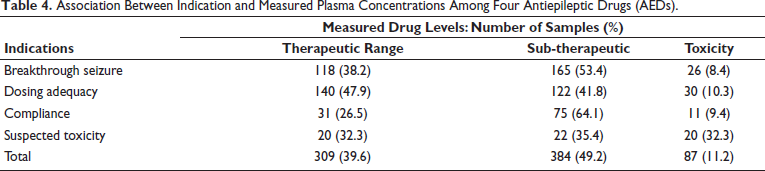
Table 4 shows odds ratios (95% confidence interval (CI)) for drug levels and indications. Carbamazepine’s compliance issues have an odds ratio of 2.889. Phenytoin’s suspected toxicity has an odds ratio of 3.815, while valproic acid shows higher odds for suspected toxicity (4.209), dosing adequacy (2.084), and compliance (2.733). No data for phenobarbitone’s toxicity. These findings highlight the importance of monitoring, dosing, and compliance, particularly for phenytoin and valproic acid.
Table 4 shows odds ratios (95% CI) for the association between indications and drug levels. Carbamazepine’s compliance issues have an odds ratio of 2.889, while phenytoin’s suspected toxicity has an odds ratio of 3.815, highlighting the need for careful monitoring. For valproic acid, odds ratios for suspected toxicity (4.209), dosing adequacy (2.084), and compliance (2.733) emphasize the importance of accurate dosing and adherence. No data is available for phenobarbitone’s suspected toxicity. These findings underscore the importance of monitoring, precise dosing, and patient compliance, especially for phenytoin and valproic acid.
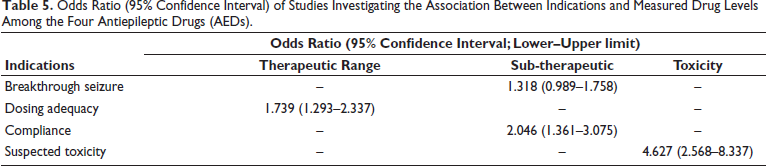
Table 5 shows the odds ratios (95% CI) for the four AEDs. For breakthrough seizures, the odds ratio is 1.318 (95% CI: 0.989–1.758). Dosing adequacy has an odds ratio of 1.739 (95% CI: 1.293–2.337). Compliance issues have an odds ratio of 2.046 (95% CI: 1.361–3.075). The odds ratio for suspected toxicity is 4.627 (95% CI: 2.568–8.337), indicating the highest risk.
Odds Ratio (95% Confidence Interval) of Studies Investigating the Association Between Indications and Measured Drug Levels Among the Four Antiepileptic Drugs (AEDs).
The study found varying proportions of samples within the therapeutic range for different AEDs. Carbamazepine had the highest at 78.9%, followed by phenobarbitone at 61.3%. Valproic acid had 40.6%, and phenytoin had the lowest at 18.1%. These results highlight the need for better monitoring, particularly for phenytoin and valproic acid, which are prone to sub-therapeutic and toxic levels.
Discussion
This study examined the relationship between plasma drug concentrations and TDM indications in a Malaysian tertiary care hospital, analyzing 780 samples from 467 epileptic patients. The patient group included 125 Chinese, 210 Malays, and 132 Indians. TDM was most often performed for valproic acid (56.8%), followed by phenytoin (27.7%), carbamazepine (11.5%), and phenobarbitone (4.0%). Phenytoin’s variability, saturable kinetics, and interactions with other drugs, like carbamazepine and valproic acid, can affect its serum levels. Drugs such as chloramphenicol and diazepam can increase phenytoin levels, while carbamazepine and alcohol can decrease them.9, 23
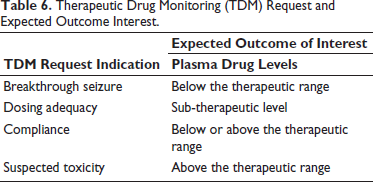
Table 6 outlines the expected outcomes for each TDM indication. TDM helps manage drug therapy by ensuring plasma concentrations stay within the therapeutic range. For breakthrough seizures, sub-therapeutic levels indicate the need for dose adjustments. Sub-therapeutic levels also suggest inadequate dosing, while TDM monitors compliance by revealing missed doses or overcompensation. Elevated levels in suspected toxicity highlight potential adverse effects. Ultimately, TDM optimizes therapy for improved efficacy and safety. 13
Therapeutic Drug Monitoring (TDM) Request and Expected Outcome Interest.
In the study of 780 samples across four AEDs (Table 3), breakthrough seizures were most common in 53.4% of cases, as expected. However, 38.2% of cases experienced breakthrough seizures within the therapeutic range, and 8.4% occurred in the toxicity range. Seizures at toxic levels may be drug-induced, which can happen at very high drug concentrations. 26 Toxicity thresholds in this study were based on clinical guidelines: phenytoin >20 mg/L, valproic acid >100 mg/L, and similar thresholds for carbamazepine and phenobarbitone. Samples exceeding these levels were classified as “toxic,” indicating potential harm. This approach allowed for targeted interventions and improved AED therapy management. For dosing adequacy and compliance, a high percentage of patients were in the sub-therapeutic range, though about 10% were in the toxicity range, suggesting non-compliance. For suspected toxicity, only 32.3% were in the toxicity range, showing that toxicity can occur at any concentration.
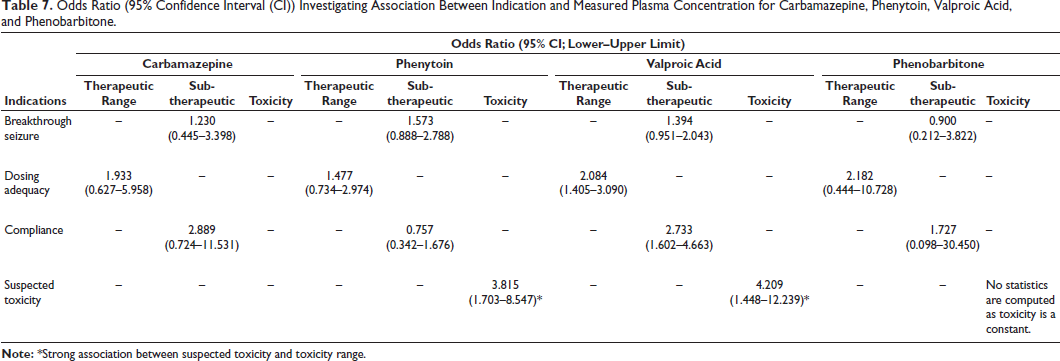
For carbamazepine (Table 3), 78.9% of concentrations were in the therapeutic range, similar to studies by Shakya et al. (79.3%) 9 and Garg et al. (75%). 11 Despite its complex pharmacokinetics, most patients achieved the therapeutic range. The odds ratio (Table 7) shows a positive association between breakthrough seizures and sub-therapeutic concentrations, as well as compliance and therapeutic range, although the CI includes values below 1.0. For phenytoin (Table 3), only 18.1% of concentrations were in the therapeutic range, and 25.9% were toxic. Breakthrough seizures showed 63.2% in the sub-therapeutic range, while 51.7% were in the toxicity range, highlighting the complexity of phenytoin management. Phenytoin (Table 7) showed a statistically significant association between suspected toxicity and toxic concentrations, with breakthrough seizures and dosing adequacy showing a positive co-relationship, although with a wide CI. For valproic acid, the most commonly monitored drug (56.8% of TDM), there was a strong correlation between dosing adequacy and therapeutic levels, compliance and sub-therapeutic levels and a significant association between suspected toxicity and toxic levels (odds ratio of 4.209). This suggests that TDM is particularly effective for managing valproic acid. Though it does not induce enzymes, valproic acid can cause drug interactions and hepatotoxicity, especially with long-term use, potentially leading to fatal outcomes. 9
Odds Ratio (95% Confidence Interval (CI)) Investigating Association Between Indication and Measured Plasma Concentration for Carbamazepine, Phenytoin, Valproic Acid, and Phenobarbitone.
Phenytoin and valproic acid showed higher rates of sub-therapeutic and toxic levels due to pharmacokinetic factors and patient variability. Phenytoin’s non-linear kinetics and narrow therapeutic index make it sensitive to dose changes, with genetic polymorphisms, drug interactions, and adherence issues contributing to variability. Valproic acid’s high protein binding and complex metabolism increase toxicity risks, especially in hypoalbuminemia or hepatic dysfunction. Non-compliance and age-related metabolic differences also play a role. These findings stress the importance of individualized dosing, TDM, and patient education. For phenobarbitone, odds ratios indicated no significant association for TDM indications, with the drug being used least (4%) due to its sedative effects.
This study shows variability in TDM levels across AEDs. Carbamazepine had the highest proportion of therapeutic samples (78.9%), while phenytoin and valproic acid had higher sub-therapeutic and toxic levels, particularly for breakthrough seizures and dosing adequacy. Phenobarbitone had 61.3% in the therapeutic range. Non-compliance with carbamazepine worsened outcomes, while phenytoin and valproic acid were linked to toxicity, highlighting the need for careful monitoring. The findings suggest that TDM guidelines in Malaysia could be improved by increasing monitoring for AEDs like phenytoin and valproic acid, which show higher rates of sub-therapeutic and toxic levels.
This evidence may prompt revisions to guidelines, emphasizing timely and accurate TDM for AEDs with variable plasma levels. The study also highlights the importance of proper blood sampling timing to avoid non-steady-state measurements, which could shape future patient care protocols. Improved communication between pharmacists and clinicians is crucial to optimizing TDM in epilepsy management. These findings suggest the need for evidence-based protocols to enhance AED therapy, improve patient outcomes and reduce adverse effects in Malaysian healthcare settings.
Limitations
This study has limitations, including varying sample sizes across AEDs, which may affect generalizability. Missing or incomplete data, such as incorrect sample timing, could introduce bias. Variability in sample quality and TDM assay techniques might impact accuracy. The retrospective design and single-hospital data limit generalizability and unaccounted confounding factors could influence results.
Clinical Recommendations
The study suggests refining TDM protocols by increasing monitoring for AEDs like phenytoin and valproic acid, emphasizing correct blood sampling timing and standardizing testing methods. Adjusting dosing for these drugs and improving clinician–pharmacist collaboration can enhance dosing accuracy, patient adherence, and overall AED therapy outcomes.
Conclusion
This study highlights key associations between TDM indications and plasma concentrations, such as phenytoin toxicity and valproic acid for dosing adequacy, compliance, and toxicity. The therapeutic range should be seen as a guide, with clinical response being the primary focus. Breakthrough seizures can occur at any concentration, but toxicity is most strongly linked to the toxicity range in phenytoin and valproic acid. Therapeutic ranges should be viewed as flexible, considering individual variations. The study emphasizes the need for further research on TDM in epilepsy management, exploring newer AEDs, polytherapy, and personalized TDM based on genetics to improve treatment strategies and patient safety.
Footnotes
Abbreviations
AEDs: Antiepileptic drugs; CI: Confidence interval; MREC: Malaysian Ministry of Health; TDM: Therapeutic drug monitoring.
Acknowledgments
The authors are thankful to the management, Quest International University, Ipoh, Perak, Malaysia, for their support.
Authors’ Contributions
Conceptualization, AM and SAA; methodology, CHY; validation, AM, SAA, and CHY; formal analysis, CHY and AK; investigation, CHY and AK; resources, CHY, AM, and SAA; data curation, CHY, AM, and SAA; writing—original draft preparation, CHY; writing—review and editing, AM and AK.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The ethical approval was obtained from Quest International University’s Joint Research and Ethics Committee and the Malaysian Ministry of Health (MREC) (Ref. No. NMRR-18-2254-43591 (IIR)). Data were kept confidential, with only summarized results presented. The data, sourced from the tertiary hospital, were considered valid and reliable patient records.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.