
Abstract
Background
Improving patient safety is vital, with medication errors posing serious risks. Understanding health professional students’ views on errors is crucial for fostering vigilant patient safety practices among future healthcare providers.
Objectives
This study aims to assess healthcare professional students’ knowledge of medication errors, their attitudes toward medication safety, and their perspectives on medication errors. Additionally, it seeks to identify educational gaps and provide recommendations for enhancing healthcare safety practices.
Materials and Methods
This is a cross-sectional, self-administered survey study. All students in the university, excluding students from years 1 and 2, were invited to complete an anonymous survey questionnaire addressing attitudes, practices, and views on medical error reporting.
Results and Discussion
Our survey involved 282 subjects, with a mean standard deviation (SD) age of 21.2 years (1.26). The mean score was 36.36 (5.2). 66.4% of participants agreed on having knowledge about medication error reporting. 39.4% disagreed with being fearful of getting blamed if they reported a medication error they made. However, a majority of participants, 44.1%, preferred to educate those who made a medication error rather than report it.
Conclusion
The participants showed good knowledge and a modest attitude toward reporting medication errors. However, translating this knowledge into practice necessitates additional training in medication safety.
Keywords
Introduction
Medication errors are generally understood to be any avoidable incident that could lead to the improper administration of medication, thereby causing harm to patients. They are also considered treatment process failures. A multidisciplinary team typically treats a patient with medication in phases: a prescription from a doctor, a pharmacist’s examination, and the administration of the medication by medical personnel. Errors can occur at any one of these three phases. 1 The consequences of medication errors include severe morbidity, prolonged hospital stays, unnecessary diagnostic tests and treatments, and even death. 2
Medication errors are recognized as one of the biggest threats to the global healthcare system.3, 4 Rising rates of morbidity and mortality linked to prescription errors have made these errors a major global patient safety concern. 1 In the United States alone, more than 250,000 patients die each year due to medication errors, leading to significant human suffering and economic losses. 5
Medication errors are a common cause of iatrogenic adverse events. 2 According to a 2019 World Health Organization (WHO) brief on patient safety, adverse events occurring from unsafe patient care are among the top 10 global causes of death and disability. Annually, preventable adverse events cause between 44,000 and 98,000 hospital deaths in the United States, more than the number of deaths attributable to motor vehicle accidents. 6
The scientific literature on medication errors published in Middle Eastern countries is limited. Most studies have been conducted in high-income countries like the United States and Europe. 7 Only a few studies have explored medication error awareness among Middle Eastern healthcare providers. For example, Tobaiqy and Stewart identified poor awareness, workload, and time constraints as critical factors hindering the reporting of medication errors. 8
Another study in Saudi Arabia by Alsulami et al. highlighted significant underreporting despite sufficient awareness of medication errors and reporting knowledge among healthcare professionals. 7 The consequences faced by physicians after medication errors can include loss of patient trust, civil actions, criminal charges, and medical board discipline. Learning more about medication errors may enhance healthcare professionals’ ability to provide safe care. 9 Despite substantial improvements in patient safety over the past decade, healthcare delivery continues to face safety issues. Education in medical schools is essential for cultivating a culture of patient safety from the start of training. 10
Patient safety content is increasingly included in the education of health-related professions worldwide.11–13 Furthermore, research shows that learning about patient safety early in one’s career, especially at the undergraduate level, is more effective than at the postgraduate level.14, 15 Therefore, students need to start their careers with a solid foundation in patient safety knowledge, skills, and attitudes. This can improve patient safety practices and service quality. To achieve this, students need both formal teaching about patient safety concepts and clinical learning environments that reflect this education. 16
There is a notable gap in studies focusing on the attitudes of health professional students toward medication errors. Understanding the knowledge, perceptions, and attitudes of these students is crucial, as they represent the future workforce. These factors are influential determinants of their future patient safety practices. 17 Studies assessing patient safety training interventions18, 19 have reported that receiving patient safety education is associated with positive behavioral changes as well as improvements in knowledge, skills, and attitudes among medical students. To date, no study has specifically assessed the attitudes of health profession students toward patient safety concepts within the United Arab Emirates (UAE).
The findings of our study can provide baseline data on health profession students’ attitudes and help improve educational programs to promote a culture of patient safety. Therefore, in this cross-sectional study, we aim to assess the knowledge, perception, and attitudes (KPA) of health professional students at our university.
Materials and Methods
Our study adopted a cross-sectional design. The research was conducted over 3 months, from November 2023 to January 2024, at Medical and Health Sciences University, UAE. The target population for our study comprised undergraduate students, except for first- and second-year students. Random sampling was utilized to select the participants from the health professional student population.
Our sampling approach prioritized fifth-year students, who were included first to ensure a comprehensive understanding of medication errors among those nearing graduation. Following this, we allocated slots to fourth-year students and third-year students in order of decreasing academic year priority. This strategy allowed us to gather insights from students at various stages of their medical education, contributing to a well-rounded analysis of medication error awareness.
We used the Raosoft calculator to determine the sample size, 20 initially estimating it to be 278 participants with a 95% confidence level and a 5% margin of error based on an assumed population of 1,000. To account for a projected 10% rate of incomplete questionnaires, we aimed for a sample size slightly higher, successfully obtaining responses from 282 participants.
Inclusion and Exclusion Criteria
The inclusion criteria for the study encompassed all students in their clinical years, specifically those in their fifth, fourth, and third years across the MBBS, dental, nursing, and pharmacy programs as applicable at Medical and Health Sciences University. Conversely, students in their first and second years, who are in preclinical stages and lack clinical experience, as well as interns, were excluded from participation.
Data Collection
The self-administered questionnaire, adapted from a validated instrument by Alsulami et al., 1 consisted of 10 questions designed to assess knowledge, perceptions, attitudes, and demographic information relevant to the study. The internal consistency of the questions was confirmed by administering them to a group of 30 students, which showed a Cronbach alpha of 0.72 before the start of the study. The questionnaire distribution was conducted in person by the research team members to ensure consistent administration and immediate collection upon completion.
The introduction page outlined the study’s aims and emphasized voluntary participation. Participants were assured of confidentiality, and informed consent was obtained before answering the questions. Confidentiality was ensured by using unique codes for identification, and personal details, including names and phone numbers, were not collected. Responses were measured using a 5-point Likert scale, ranging from “strongly disagree” to “strongly agree.” Responses were summed, and mean scores were calculated for each participant.
Data collection procedures included measures to accommodate participants’ schedules, ensuring they had adequate time to complete the questionnaire without external pressure. Completed questionnaires were securely stored to protect participant confidentiality, with appropriate measures taken for data-entry accuracy and completeness as applicable to maintain data integrity.
Data Analysis
The responses were analyzed using Statistical Package for the Social Sciences (SPSS) (version 26); a p value of <.05 was considered statistically significant. Descriptive data analysis was performed for all questions on the Likert scale, assuming it was interval data. The normality of the data was analyzed using the Shapiro–Wilk test before the analytical comparisons.
Results
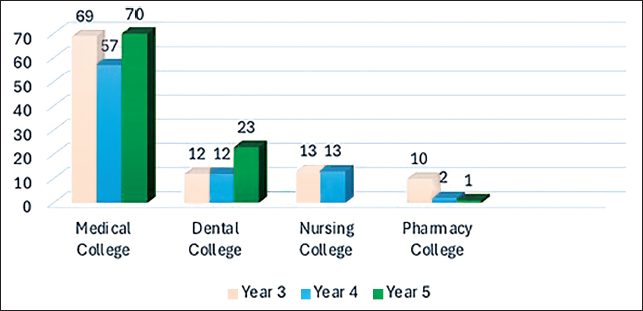
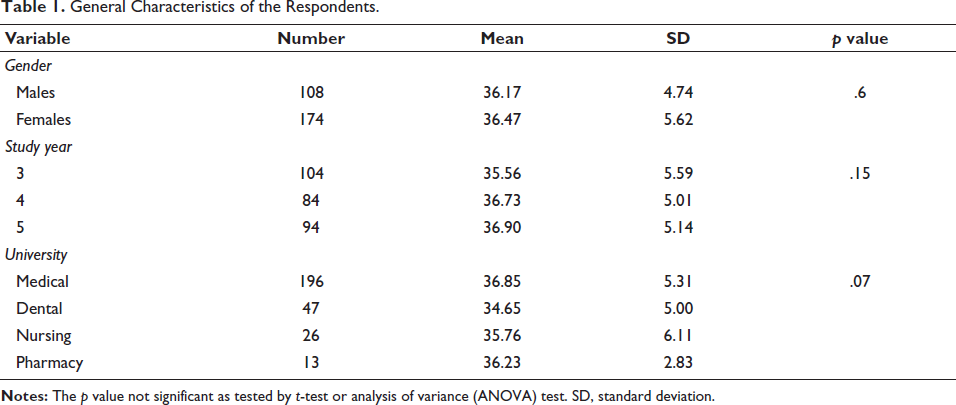
Out of 282 students surveyed, 196 were from the MBBS program, 47 were from the dental program, 26 were from the nursing program, and 13 were from the pharmacy program, ensuring diverse representation from various clinical disciplines within the university (Figure 1). The participants’ ages ranged from 19 to 27 years, reflecting a narrow age distribution centered around a mean age of 21.2 years, with minimal variation indicated by a standard deviation (SD) of 1.26 years (Table 1). Participants achieved a median score of 36 with an interquartile range of 6 (mean score of 36.36, with an SD of 5.2).
Number of Clinical Students from Each College Who Took Part in the Survey Regarding Medication Errors.
General Characteristics of the Respondents.
The majority (91.4%) of respondents indicated they would report a medication error if a patient had been prescribed an inadequate dose. A significant majority (87.2%) of respondents expressed willingness to report errors where medication was prevented from reaching the patient. This highlights a high level of awareness and responsibility among the surveyed students toward ensuring medication reaches patients as intended, emphasizing their commitment to patient safety (Figure 2).
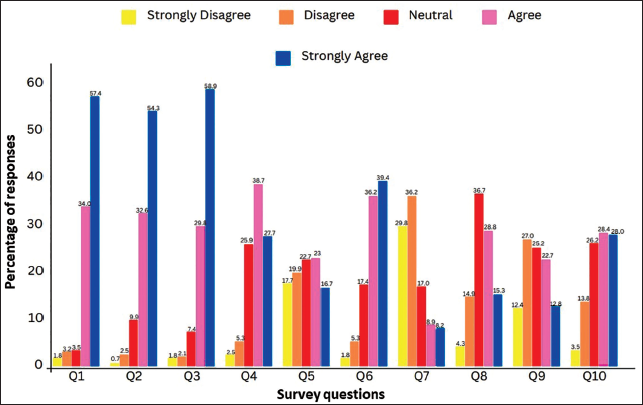
Similarly, a large majority (88.7%) of respondents indicated they would have reported a medication error if a patient had not received medication as prescribed. This underscores a strong sense of accountability and recognition of the importance of adherence to medication regimens among the surveyed students.
Responses indicated a mixed level of confidence among respondents regarding their knowledge of when a medication error should be reported. While a significant portion (66.6%) expressed confidence in their knowledge, there was also a notable percentage (32.6%) who may have felt less assured in this aspect, suggesting a need for further education or clarification (Figure 2).
Perception Regarding Medication Errors
The majority (76.3%) of respondents disagreed with the statement that medication errors did not need to be reported if detected before reaching the patient. A substantial majority (75.6%) of respondents expressed confidence that information disclosed when reporting a medication error would be kept confidential. This suggests a level of trust in the reporting system’s ability to maintain confidentiality, which may have encouraged reporting among the surveyed students (Figure 2).
Responses indicated varying opinions among respondents regarding their responsibility to report medication errors caused by someone else. While a significant percentage (65.4%) believed it was their responsibility, a notable portion (29.0%) expressed disagreement. This suggests differing perspectives on accountability and the role of individuals in error reporting within healthcare settings (Figure 2).
Attitude Toward Medication Errors
A considerable percentage (65.1%) of respondents indicated a preference for educating people who made medication errors rather than reporting the errors. This suggests a recognition of the value of education in error prevention but also highlights a potential barrier to proactive reporting practices among the surveyed students (Figure 2).
A significant percentage (77.9%) of respondents expressed some level of fear of being blamed if they reported a medication error they had made, and 86.9% of respondents indicated they hesitated before deciding to report a medication error. This suggests a degree of uncertainty or reluctance among the surveyed students when it comes to error reporting, potentially influenced by factors such as fear of blame or perceived consequences.
In summary, a substantial portion (66.4%) of respondents demonstrated familiarity with medication error reporting protocols, indicating a baseline level of awareness in the surveyed population. Interestingly, a notable 39.4% disagreed with concerns about potential blame when reporting medication errors, indicating a willingness to engage in reporting practices despite perceived risks. Moreover, a majority (44.1%) expressed a preference for addressing medication errors through education rather than formal reporting, highlighting a preference for corrective measures that prioritize learning and improvement over punitive actions (Figure 2).
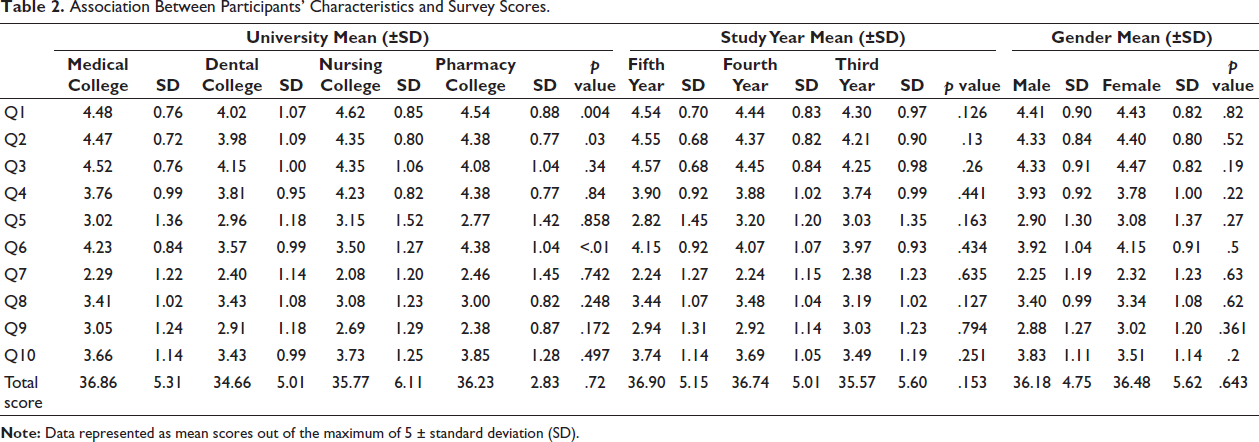
A Bonferroni multiple comparisons test was conducted to examine the differences in participants’ responses to the survey across the colleges. Significant differences were observed between medical college and dental college (p = .005) and between dental college and nursing college (p = .023) for errors related to inadequate dosing. In terms of reporting errors where medication was prevented from reaching the patient, medical college participants had a mean score of 4.47, which was significantly higher than the mean score of 3.98 for dental college (p = .001). For confidence in the confidentiality of reporting, significant differences were found between medical college and dental college (p < .001), medical college and nursing college (p = .001), pharmacy college and dental college (p = .016), and pharmacy college and nursing college (p = .016) (Table 2).
Association Between Participants’ Characteristics and Survey Scores.
To assess whether there was a significant difference in the outcomes across different year groups, we conducted a Bonferroni post hoc test following a one-way analysis of variance (ANOVA), with participants categorized into three levels based on year of admission: level 1 (2021 and 2022), level 2 (2020), and level 3 (2017, 2018, and 2019). Out of the 10 questions included in our survey, questions two and three were found to be statistically significant. For question two, the p value obtained was .013 (Table 2). Given that this value is below the significance threshold of .05, we reject the null hypothesis, indicating a statistically significant difference in the outcomes between the year groups for this question. Similarly, for question three, the p value was .026. This suggests that the differences in responses across the year groups are statistically significant for this question as well. These findings demonstrate that the year of study is a significant factor influencing the responses to both questions two and three of our survey, with meaningful differences observed between the specified year groups.
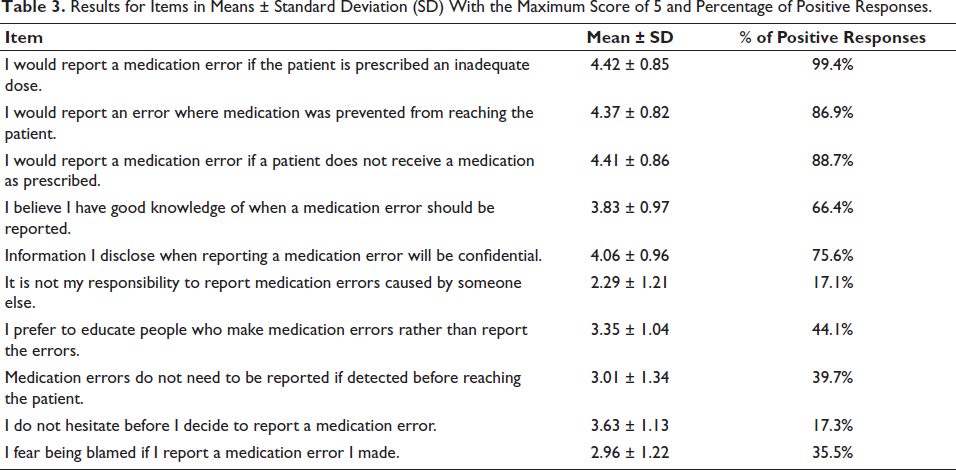
An independent samples t-test was performed across the 10 questions to examine differences between genders. Males (Code 1) had a mean score of 3.83 with an SD of 1.11, while females (Code 2) had a mean score of 3.51 with an SD of 1.14 (Table 2). Question 10 showed a statistically significant result. The two-sided p value for question 10 was .02. This suggests that there is a significant difference between genders in terms of hesitation before reporting a medication error. The mean score for males is higher than that for females, implying that males tend to hesitate more before reporting medication errors compared to females. The significant difference observed suggests that gender may influence hesitation in reporting medication errors. This finding could inform strategies aimed at improving reporting practices and addressing gender-specific concerns in clinical environments. The mean scores with SD for individual item questions are listed in Table 3.
Results for Items in Means ± Standard Deviation (SD) With the Maximum Score of 5 and Percentage of Positive Responses.
Discussion
The aim of using medication is to reach specific therapeutic outcomes, enhancing quality of life while reducing patient risk. 16 Healthcare institutions widely use both internal and external error reporting systems. Preventing these errors is crucial because most of the harm they cause is iatrogenic, which is well attempted to prevent the illness and not due to the presence of any already existing condition in those patients. 21
Medication errors can happen at any stage of the medication process, including prescribing, dispensing, and administering the drug to the patient. These errors raise morbidity and mortality rate rates and increase treatment costs. Additionally, they undermine patients’ confidence in medical care.22, 23 Reporting medical errors is essential for improving patient safety and care quality. By documenting and analyzing these errors, healthcare providers can identify causes and implement preventive measures. This fosters a culture of transparency and continuous improvement, leading to better safety protocols, training, and patient confidence in the medical system. The goal is to reduce risks and ensure more reliable care for patients. 24
According to WHO estimates, a troubling number of people die annually due to unsafe medical care. Reports indicate that 1 in 10 hospitalized patients experiences harm, with at least half of these incidents being preventable. 4
Teaching patient safety to healthcare professionals during undergraduate studies is more impactful than postgraduate training. Establishing a solid foundation in safety concepts, skills, and attitudes early on enhances patient safety practices and improves the overall quality of healthcare services. 16
Our study delves into perspectives, attitudes, and understanding of medication error reporting among health professional students. It reveals that these students show a commendable level of awareness and a strong sense of responsibility toward ensuring patient safety. However, the research also identifies specific areas where there is potential for enhancement in their knowledge and practices related to reporting medication errors. This insight underscores the importance of continuous education and training to further strengthen their skills in healthcare quality and safety.
Participants’ awareness of medication errors was evaluated through 10 questions covering definitions, types, prevention strategies, and response protocols. Most participants demonstrated a strong understanding of medication errors. Participants from nursing college were found to be most likely to report inadequate dosing errors, while dental college participants were significantly less likely, with medical college participants falling in between. Participants from medical college were found to be significantly more likely than dental college participants to report errors where medication was prevented from reaching the patient. Participants from pharmacy and medical colleges were found to have higher confidence in the confidentiality of error reporting. In contrast, dental college and nursing college participants were found to be significantly less confident.
A study conducted by Alsulami et al. showed that approximately 97% of participants had sufficient knowledge, and 90% had a favorable attitude toward medication error reporting. 7 In contrast, our study found that 66.6% of respondents expressed confidence in their knowledge regarding medication errors, 44.1% expressed a preference for addressing medication errors through education rather than formal reporting, 35.5% expressed fear of being blamed if they reported a medication error they made, and 17.3% indicated they hesitated before deciding to report a medication error.
This could further be supported by another study conducted by Alandajani et al., where between 50% and 60% of individuals chose not to report medication errors to avoid blame, being labeled as troublemakers, adverse reactions from managers, punitive actions, legal issues, malpractice suits, and appearing incompetent to their coworkers. 25 Similarly, another study concluded that the fear of being blamed could discourage some doctors and pharmacists from reporting medication errors. 26 A study conducted by Isaacs et al. identified the inexperience of health professionals and nurse-patient ratios as major challenges. Addressing these could involve training junior staff and better managing nurse workloads. 27 Another study concluded that a non-punitive environment is crucial to encouraging error reporting. Implementing a simple, anonymous reporting system, along with providing feedback and rewards, can help increase the rate of error reporting by nurses.
Similarly, Patel et al. reported in their study that automating the medication process in hospitals and providing thorough pharmacological education to prescribers and nurses can help decrease medication errors. Additionally, establishing and enforcing drug use policies can curb the inappropriate use of drugs. 29 Comparatively, the studies conducted by Alser et al. and Al-Sawalha et al. demonstrated positive attitudes toward patient safety among students.16, 30
Ezzi et al. reported that students tend to have an overall positive perception of patient safety culture, with a global mean score of 5.33 ± 0. 10 Whereas in our study, perceptions of medication errors varied. Most respondents (76.3%) disagreed that errors detected before reaching the patient did not need reporting. Additionally, 75.6% trusted that reported information would remain confidential, suggesting faith in the system’s confidentiality and encouraging reporting. However, views on responsibility for reporting others’ errors differed. 65.4% felt that it was their duty, while 29.0% disagreed, indicating differing opinions on accountability in healthcare settings.
In contrast to other studies, the students who participated in our study indicated a mixed level of confidence among respondents regarding their knowledge of when a medication error should be reported. A significant portion (66.6%) expressed confidence in their knowledge, demonstrating awareness of the importance of medication safety and its impact on patient well-being. However, there was also a notable percentage (32.6%) who may have felt less assured in this regard, suggesting a need for further education or clarification.
We found that there existed a discrepancy between perception and reality; hence, translation to practice necessitates more training in medication safety. Finally, our study showed modest attitudes among students toward reporting and preventing medication errors. It could be seen that the fear of blame and repercussions hindered proactive reporting and prevention efforts.
The findings of our study have several important implications. First, the data provide a comprehensive understanding of the knowledge and attitudes of students regarding medication errors. Educational institutions can use this information to tailor their curricula to address gaps in knowledge and enhance training programs such as simulation-based modules aimed at reducing medication errors. Additionally, the insights gained from the study can inform policymaking at the institutional level, promoting a culture of safety and awareness in healthcare settings.
Limitations of our study include the questionnaire-based study design, which is subject to recall bias. The use of a self-administered questionnaire may introduce response bias, as participants might provide socially desirable answers rather than truthful responses. The sample size, restricted to students from one university, limits the generalizability of the findings to the rest of the healthcare population. Moreover, the cross-sectional nature of the study provides a snapshot in time, making it difficult to conclude changes in knowledge and attitudes over time.
Future research should consider longitudinal studies to track changes in students’ knowledge and attitudes over their academic careers. Expanding the study to include multiple institutions would enhance the generalizability of the findings. Additionally, qualitative research methods, such as interviews or focus groups, could provide deeper insights into the reasons behind the observed attitudes and behaviors. Investigating the impact of specific educational interventions on reducing medication errors would also be a valuable area of study.
Conclusion
Our study highlights that while healthcare professional students are aware of the importance of medication safety and its impact on patient well-being, there is a significant gap between their perception and actual practice. Our findings indicate that students exhibit moderate attitudes toward reporting and preventing medication errors. The fear of blame and potential repercussions often hinders proactive reporting and prevention efforts, suggesting that a cultural shift toward a non-punitive approach may be essential to encourage better practices in medication safety. Further, there is a necessity for training modules in medication safety during program delivery.
Footnotes
Abbreviations
KPA: Knowledge, perception, and attitudes; MBBS: Bachelor of Medicine, Bachelor of Surgery; RAKCOMS: Ras Al Khaimah College of Medical Sciences; RAKMHSU: Ras Al Khaimah Medical and Health Sciences University; REC: Research Ethics Committee; SD: Standard deviation; SPSS: Statistical Package for the Social Sciences; UAE: United Arab Emirates; UG: Undergraduate; WHO: World Health Organization.
Acknowledgments
The authors are grateful to the volunteers and RAKMHSU administration for their support and encouragement.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
The study was approved by the university’s Ethics Committee under the reference number RAKCOMS-REC-32-2023/24-UG.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.