
Abstract
Background
Chronic kidney disease (CKD) is a condition that deteriorates over time and causes the loss of nephrons, leading to impaired kidney function and finally bringing on end-stage renal disease (ESRD). As the world’s 12th biggest cause of mortality, CKD presents a serious public health concern, with an exceptionally high prevalence of diabetic nephropathy among diabetic patients. The economic burden of ESRD, especially in the context of renal replacement therapy, is substantial and can be financially challenging for patients. Oxidative stress is recognized as a prominent and advancing factor in CKD, irrespective of its underlying causes. Imbalances in gut microbiota have also been associated with CKD, potentially exacerbating its progression. Elevated urea levels in CKD patients can compromise the integrity of the gut epithelial barrier, permitting the entry of bacterial toxins into the bloodstream and consequently triggering systemic inflammation. This inflammatory milieu, along with microbiota imbalances, can contribute to increased oxidative stress, heightened susceptibility to infections, immunological dysfunction, and insulin resistance, all of which negatively impact the prognosis of CKD.
Objectives
The purpose of this research is to postpone the progression of CKD to lower the risk of ESRD, eventually improving the quality of life for impacted patients. The study utilizes creatinine and glomerular filtration rate (GFR) as markers to assess CKD progression and renal function. The research aims to compare the reno-protective efficacy of two treatment regimens: N-acetylcysteine with keto analogs instead of probiotics and keto analogs in individuals with predialytic CKD receiving care in a nephrology department.
Materials and Methods
A prospective observational study was carried out for 6 months in a nephrology department of a super specialty hospital. Patient data were collected from case sheets and through history interviews. Categorical variables were analyzed using frequencies and percentages.
Results
Following the application of the inclusion criteria, 50 patients were chosen for the investigation. While there was significant variation in age and CKD stages between the two groups, no significant gender differences were observed. Statistically significant differences were identified between the research groups concerning the percentage reduction in creatinine and improvements in GFR.
Conclusion
The study’s outcomes show that probiotics and keto analogs work well together for patients with and without diabetes, especially those with severe CKD. Conversely, combining N-acetylcysteine with keto analogs appears to be more effective in early CKD stages. A noteworthy negative correlation was observed between creatinine and GFR in patients receiving the probiotic and keto analogs combination compared to those receiving N-acetylcysteine and keto analogs.
Introduction
Chronic kidney disease (CKD) is defined as an impairment in kidney structure or function that lasts longer than 3 months. The phrase “renal damage” describes a wide range of issues found during a clinical examination, some of which may be non-specific and insensitive to the illness’s underlying cause but may manifest before kidney function is lost. In most chronic kidney conditions, excretory, endocrine, and metabolic functions all degrade together. 1 There are five stages in which CKD develops. Stage 5D is a dialytic stage of end-stage renal disease (ESRD), whereas stages 1–4 non-dialytic (ND) are known as predialytic. CKD ranks 12th in terms of mortality and 17th in terms of disability, with an ESRD incidence of 160–232 patients per million (ppm) and a prevalence of 785–870 ppm every year. Raising public and general practitioner knowledge of renal illness might lead to earlier diagnosis of chronic renal failure and the development of preventative interventions to postpone the onset of ESRD.2, 3
Affected populations with CKD range from 8% to 16% worldwide and are commonly misunderstood by patients and doctors. 4 It is estimated that over 80% of the patients undergoing therapy for ESRD live in wealthy nations with substantial senior populations and universal access to health care. 5 Over 70% of diabetic individuals who receive dialysis die within 5 years, making ESRD a disease with a worse prognosis than most malignancies. 6 It is widely assumed that CKD advances unabatedly toward ESRD when glomerular filtration rate (GFR) goes beyond a certain level. The loss of an essential number of nephrons starts a deadly cycle that escalates nephron loss, which endures irrespective of the treatment administered for the disease’s primary cause. 7
Renin–angiotensin–aldosterone system (RAAS) inhibitors and, more recently, medications that block sodium-glucose cotransporter 2 (SGLT2) at the convoluted tubule at the proximal end have been shown in multiple clinical trials to be able to prevent GFR decline over the long term. The most effective medication for lowering urine protein, CKD development, and cardiovascular disease risk is angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers (ARBs) that suppress the RAAS. 8
The purpose of the study was to decelerate the progression of kidney failure. In this investigation, we used the mechanisms above in various combinations [N-acetylcysteine + keto analog (NACK) and probiotics + keto analog (PROCK)].
N-acetylcysteine
N-acetylcysteine may be able to halt renal function loss by lowering serum creatinine, increasing endogenous creatinine clearance, and improving podocyte ultrastructure. N-acetylcysteine has been shown to considerably lower urine protein in diabetic rat models and may even postpone the onset and development of nephropathy due to diabetes.9–11 The Kidney Disease: Improving Global Outcomes (KDIGO) guidelines promote utilizing NAC owing to its low cost and lack of side effects. 12 When used to treat the most severe damage, NAC has the best antioxidant and anti-inflammatory strengths, like in patients with ESRD undergoing hemodialysis or dialysis through the peritoneum.13, 14
Keto Analogs (KAs)
The body uses KAs, which are transformed into branched-chain amino acids via the urea cycle, to supplement a very low protein diet (VLPD) to avoid nutritional shortages. Leucine and keto leucine, which may respectively promote muscle protein synthesis and decrease protein breakdown, are included in significant amounts in KA supplements. 15 According to several earlier research, KA supplements may help CKD patients with VLPD delay the course of their condition. 16 The most common applications of alpha-KA in CKD are as diet supplements or as an adjuvant to nutritional therapy. Dietary variables may impact the development of CKD and its consequences. However, early treatment can also successfully slow down CKD progression. This drug protects patients with renal failure against an unnecessary increase in urea blood levels caused by using non-essential amino acids. 17
Probiotics
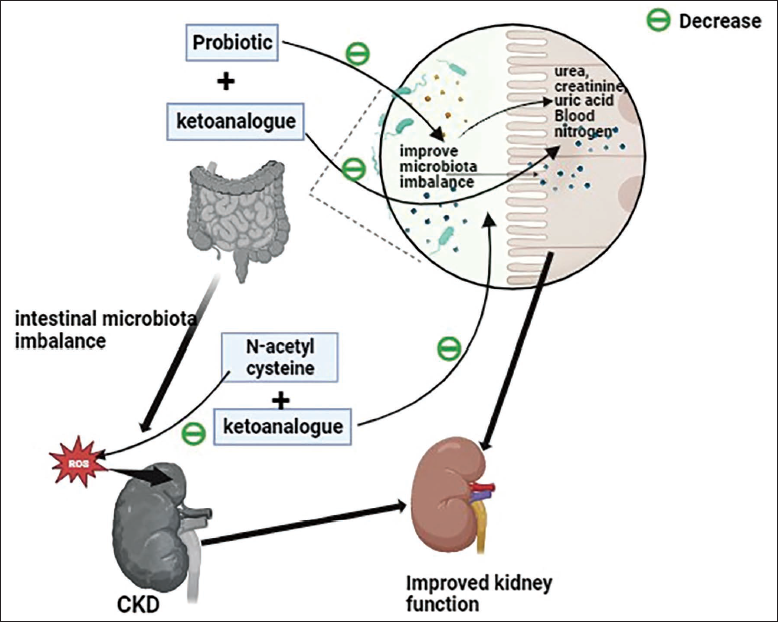
Probiotics are the subject of extensive research as a natural biotreatment because of their range of health-improving benefits and innate capacity to combat ailments such as CKD. Probiotics reduce the absorption of uremic toxins through food (indoxyl sulfate, p-cresyl sulfate) and suppress the growth of aerobic bacteria that produce uremic toxins. 18 According to some studies, a combination of probiotics and prebiotics promotes the growth of symbionts and probiotics when used together. 19 KA supplements may help CKD patients with VLPD delay the progression of the disease.20, 21 Another possibility is that probiotics and prebiotics promote the growth of symbionts and probiotics when used together. Nine MHD patients have shown evidence of this type of chemical relationship, known as “symbiotics,” being able to lower serum p-cresol levels.22–24 The graphical abstract of reno-protection with a combination of N-acetylcysteine and KAs versus probiotics and KAs in predialytic CKD, as shown in Figure 1.
Graphical Abstract of Reno-protection with the Combination of N-acetylcysteine and Keto Analogs Versus Probiotics and Keto Analogs in Predialytic Chronic Kidney Disease.
Materials and Methods
Study Design and Subjects
The prospective observational research was carried out over 6 months at the Department of Nephrology in a tertiary care hospital in Hyderabad, India. The study’s primary goal was to compare the effects of two different treatment regimens on predialysis patients with CKD.
Study Participants and Eligibility Criteria
Inclusion Criteria
Predialytic patients were included in the study including CKD stage 1-4 and CKD stage 5 ND, age group 18-85 years, comorbidities such as hypertension; and both diabetic and non-diabetic patients.
Exclusion Criteria
Patients were excluded from participation if they presented any conditions: inflammatory bowel disease, acute gastroenteritis, chronic diarrhea, and known metallic allergies.
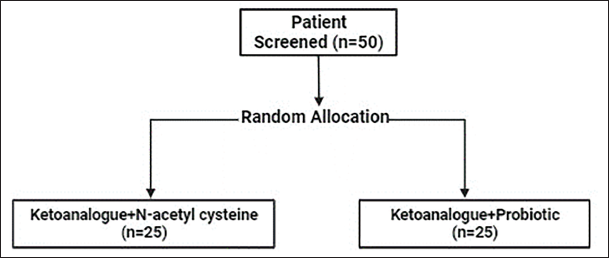
Study procedure: A total of 100 patients participated in the study with 50 patients receiving probiotics and ketoanalogues and 50 patients receiving N-acetyl cysteine and ketoanalogue. The selected patients were randomly assigned to one of two treatment groups: (a) PROCK and (b) NACK. Randomization was performed rigorously to minimize selection bias and ensure comparability between the two groups, as shown in Figure 2.
Treatment Groups and Randomization of PROCK: Probiotics + Keto Analog and NACK: N-acetylcysteine + Keto Analog.
Patients underwent assessments during three successive visits at Owaisi Hospital and Research Centre from August 2016 to April 2017. The study subjects were aged from 30 to 80 years. A detailed patient history was employed as a standardized tool to systematically gather relevant patient data, including demographics, comorbidities, and renal function parameters. Patients matching our study criteria were included. Serum creatinine levels and GFR were meticulously measured before and after administering the respective treatment combinations. The Jaffe reaction method was employed to determine serum creatinine levels, and the modification of diet in renal disease (MDRD) equation was used for GFR calculations. Steps were taken to avoid patients who were dialytic along with comorbid conditions. Following a thorough examination and history collection, patients who met the study’s eligibility requirements were chosen, and informed consent was obtained.
Statistical Analysis
The data were analyzed using suitable statistical software version 20.0 to determine the effect of treatment regimens on serum creatinine and GFR. Statistical tests were applied, such as unpaired t-tests for baseline comparisons and chi-square tests for categorical variables. A significance level of p value <.05 at a 5% significance level was established to determine statistical significance.
Results
Patient Demographics
Age Distribution
Out of 50 participants based on inclusion criteria, 47% of patients between the age range of 51–60 years are affected with predialysis stage 1–4 and stage 5 ND, followed by the age group 30–50 years with 23.3%. The mean age (Mean ± SD) is 53.8 ± 13.54.
Gender Segregation
Of all the participants, 31% were men, while only 19% were women.
Distribution Based on Comorbidities
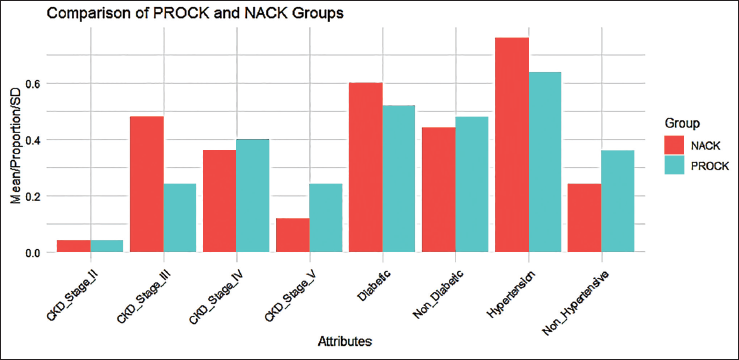
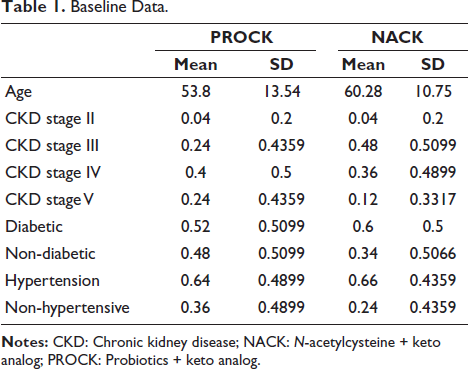
Among all patients with comorbid conditions, there were no significant differences in diabetic, non-diabetic, hypertensive, and non-hypertensive status between the groups. However, a significant difference was found in CKD stages in the probiotic group, as seen in Table 1 and Figure 3.
Distribution of Comorbidities.
Baseline Data.
Comparison of Serum Creatinine Before and After Treatment Between Test and Control Subjects
The average serum creatinine levels in the PROCK group were 0.8292509 units, whereas in the NACK group, serum creatinine levels were 1.4584 units. The p value was found to be significant (i.e., p = .07).
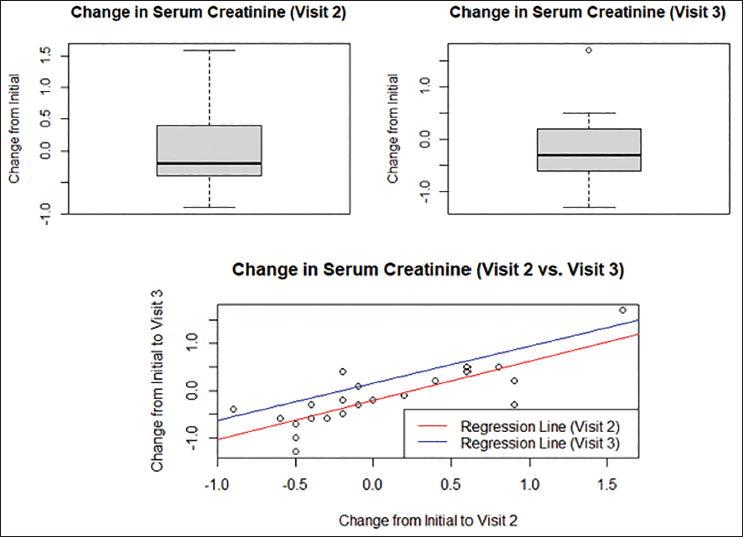
The Welch two sample t-tests were conducted to compare mean serum creatinine levels between the “NACK” and “PROCK” groups at three different visits. They showed a significant correlation in mean serum creatinine levels between both groups, as seen in Figures 4 and 5.
Serum Creatinine N-acetylcysteine + Keto Analog (NACK) Regression Analysis by Comparing Changes in Serum Creatinine from Initial Visit to Visit 3.
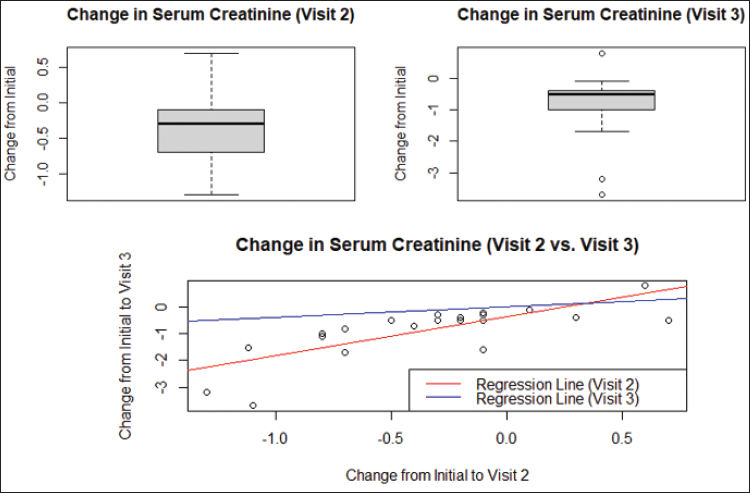
Serum Creatinine Probiotics + Keto Analog (PROCK) Regression Analysis by Comparing Changes in Serum Creatinine from Initial Visit to Visit 3.
Comparison of GFR of Visits 2 Versus 3
The analysis reveals a significant mean of 0.62044 units for the NACK group. This means that for every one-unit increase in GFR at visit 2, there is an estimated increase of 0.62044 units in GFR at visit 3 with a p value of 6.333e-07. These findings underscore the predictive value of GFR at visit 2 for estimating GFR at visit 3 in the NACK group, as seen in Figure 6 and Table 2.
Linear Regression Analysis Summarizes the Results of the Welch Two Sample t-tests Comparing Serum Creatinine Levels Between the “NACK” and “PROCK” Groups at Different Visits.
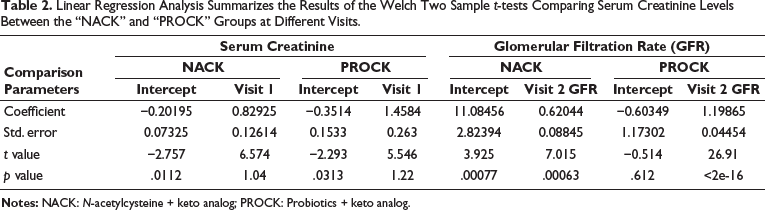
Glomerular Filtration Rate (GFR) N-acetylcysteine + Keto Analog (NACK) Regression Analysis by Comparing Changes in GFR from Visits 2 to 3.
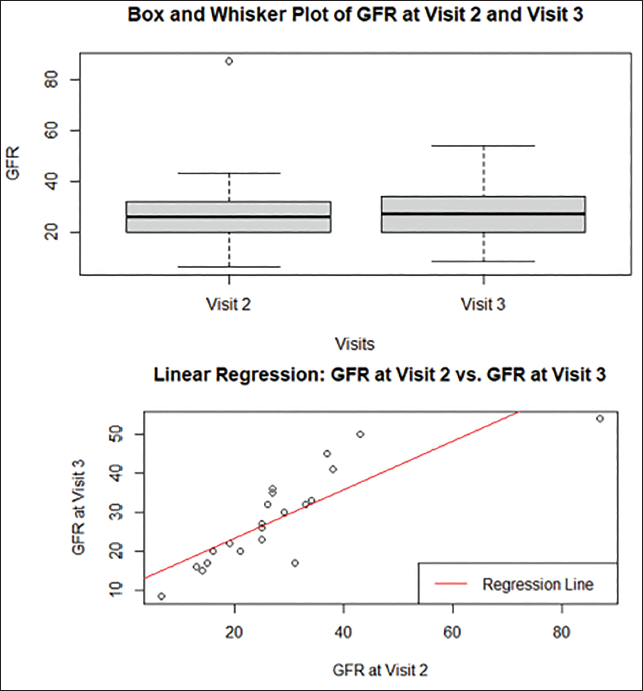
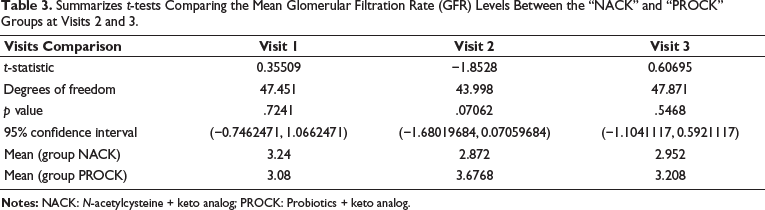
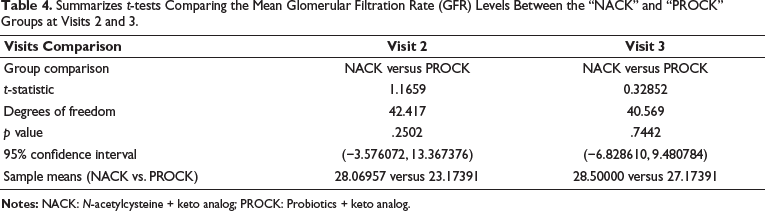
In the PROCK group, the linear regression analysis reveals an approximately 1.19865, which signifies that for every unit increase in GFR at visit 2, there is an estimated increase of 1.19865 units in GFR at visit 3. The model explains an exceptionally high 97.18% of the variability in GFR at visit 3 in Figure 6 and Table 3. The Welch two sample t-tests conducted to compare mean GFR levels between the “NACK” and “PROCK” groups at visit 1 revealed that there is no significant difference in mean GFR levels between these groups. At visit 2, the analysis indicated that the mean GFR for the “NACK” group is approximately 28.07, while for the “PROCK” group, it is around 18.17, with a p value of .2502, suggesting a statistically significant difference. Similarly, at visit 3, the mean GFR for the “NACK” group is approximately 28.50, and for the “PROCK” group, it is approximately 17.17, with a p value of .7442, again indicating a significant difference. These findings suggest that, on average, GFR levels at these time points are comparable between the two groups despite individual variations within each group. This implies that the mean GFRs differ significantly, as seen in Table 4.
Summarizes t-tests Comparing the Mean Glomerular Filtration Rate (GFR) Levels Between the “NACK” and “PROCK” Groups at Visits 2 and 3.
Summarizes t-tests Comparing the Mean Glomerular Filtration Rate (GFR) Levels Between the “NACK” and “PROCK” Groups at Visits 2 and 3.
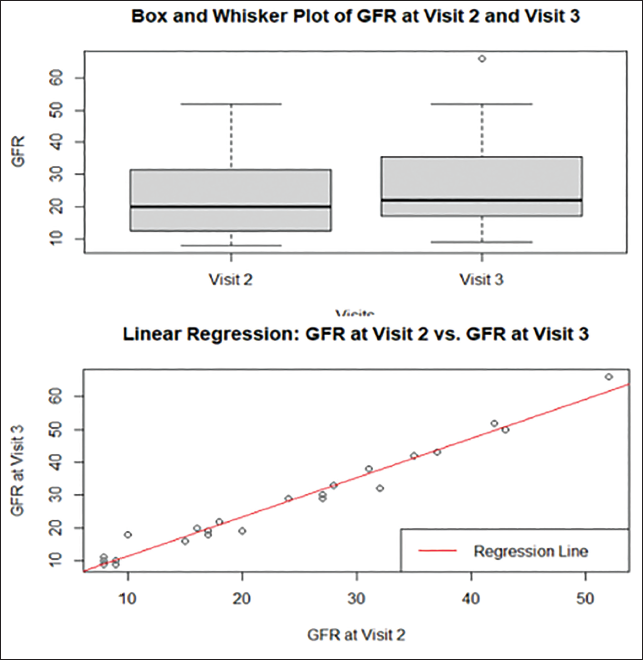
This underscores the need for personalized patient care and monitoring. The linear regression analyses also demonstrated strong predictive relationships between GFR levels at different visits within both groups. This predictive power highlights the clinical relevance of understanding how changes in GFR at a one-time point can inform expectations for future GFR levels. Notably, the “PROCK” group exhibited an exceptionally high predictive power, suggesting that GFR levels at visit 2 strongly forecast GFR levels at visit 3 within this group. In clinical practice, monitoring and intervention strategies should consider these individual variations to provide the most effective care and treatment outcomes, as seen in Figure 7.
Glomerular Filtration Rate (GFR) Probiotics + Keto Analog (PROCK) Regression Analysis Comparing Changes in GFR in Visits 2 and 3.
Discussion
There is no effectiveness in reducing the progression of CKD. Decreasing serum creatinine levels can help reduce the progression of CKD. A combination of PROCK improves GFR by decreasing serum creatinine levels. The statistical analysis indicates that it is important to recognize that the “PROCK” group shows higher individual variability, as demonstrated by the correlation between visits. This variability within the “PROCK” group has clinical implications, suggesting that while the group’s mean remains similar to that of the “NACK” group, some individuals in the “PROCK” group have experienced more significant changes in serum creatinine over time. The study investigated the impact of two different treatment regimens, NACK and PROCK, on patients with CKD. The analysis of patient demographics revealed that both groups were well-matched in gender distribution, with no significant differences observed. However, there was a notable difference in age, with the NACK group having a higher mean age than the PROCK group. This age difference underscores the importance of considering age as a potential factor when evaluating treatment outcomes, as older individuals may respond differently to treatments. Regarding comorbidities, the study found that both groups had a similar distribution of diabetic and non-diabetic patients, as well as hypertensive and non-hypertensive patients. Notably, there were no significant differences in diabetic and hypertensive status between the two groups. However, a significant association was found between the variable of CKD stages and the treatment groups. This suggests that the severity of CKD may have influenced the allocation of patients to the NACK and PROCK groups.
The analysis of serum creatinine levels before treatment (visit 1) and after treatment (visits 2 and 3) revealed interesting findings. In the NACK group, there was a positive relationship between changes in serum creatinine levels at visits 2 and 3, indicating that elevations in serum creatinine at visit 2 were associated with higher levels at visit 3. Similarly, changes in serum creatinine levels from the initial visit to visit 1 showed a strong positive relationship with changes from the initial visit to visit 3. This suggests a consistent pattern of serum creatinine changes within the NACK group. In contrast, the PROCK group exhibited a strong and positive relationship between changes in serum creatinine levels at visits 2 and 3. This relationship was supported by residuals falling within a specific range, quartile breakdowns indicating a distribution around the regression line, and highly significant coefficients. These findings suggest that changes in serum creatinine at visit 2 strongly predict changes at visit 3 within the PROCK group.
Study Limitations
It is extremely important to recognize any potential limitations of this research, including the small sample size and single-center design of the study, which may influence the generalizability of the findings. In determining our sample size of 25 participants in each group, we also considered the constraints related to the availability of funding and resources. Conducting a larger-scale study would have required additional financial resources, personnel, and logistical support, which were not feasible within the scope of this research.
Conclusion
According to the results of our investigation, stage 2–4 and stage 5 ND CKD patients have higher serum creatinine levels. Patients with high serum creatinine levels had significantly higher GFR levels, leading to ESRD. Thus, serum creatinine levels can be decreased more significantly with the PROCK group, which will help delay the progression of ESRD. This study reinforces the importance of tailoring patient care based on individual profiles and trends, even when group means appear similar. In clinical practice, monitoring and intervention strategies should consider these individual variations to provide the most effective care and treatment outcomes for patients with CKD. Additionally, because PROCK therapy lessens the strain on the remaining nephrons, it may have a greater effect on patients, especially those who are older and have had CKD.
Future research with bigger sample sizes and longer follow-up periods may give more insights into the efficacy of various treatment regimens and further improve individualized therapy options for CKD patients.
Footnotes
Abbreviations
CKD: Chronic kidney disease; GFR: Glomerular filtration rate; KDIGO: Kidney Disease: Improving Global Outcomes; MDRD: Modification of diet in renal disease; NACK: N-acetylcysteine + keto analog; PROCK: Probiotics + keto analog.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
This study was approved by the Institutional Review Board (IRB No: 2016/14/014) on November 30, 2016, at Deccan College of Medical Sciences and Allied Hospital, Hyderabad, Telangana, India. Informed consent was obtained from each participant, providing comprehensive information about the study’s objectives and potential risks.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.