
Abstract
Background
Varicocelectomy is one of the main complications that, if left untreated, results in male infertility. Various approaches have been adopted to manage it, but there is a variation in the consensus.
Objectives
This systematic review aims to summarize the evidence on the various clinical trials and post-varicocelectomy recovery for patients consuming different supplements or regimens.
Methodology
An organized and systematic literature search was conducted in five electronic databases from their inception till 2021. Upon applying the PICOT format and student inclusion criteria, only n = 13 articles fulfilled the eligibility criteria and were selected for this systematic review.
Results
A total of 13 studies were included in this systematic review, and different outcomes were measured in all the studies. Generalizing the outcomes measured, they are classified in semen parameters, including sperm count, sperm motility percentage, sperm with standard morphology percentage, semen volume, sperm density, hormonal profile including testosterone (nanograms/liter), follicle-stimulating hormone (international units/liter), luteinizing hormone (international unit/liter), seminal oxidative stress including total antioxidant capacity (mm Trolox equivalent per liter), and pregnancy outcome.
Conclusion
This systematic review suggests improved sperm count and pregnancy outcomes with pharmacotherapeutic interventions. Oral antioxidants, vitamin C, and vitamin E showed marked improvements in sperm density and reduction in sperm DNA damage. Oral supplements, that is, saffron, were also effective but needed larger, well-conducted randomized clinical trials to validate the findings and estimate the overall impact of these interventions in the post-varicocelectomy period.
Keywords
Introduction
Infertility in the current healthcare setting is one of the leading challenges to the global population. A couple is declared infertile if they fail to conceive after 1 year. In most cases of infertility, fertile females and infertile men account for 40–50%. 1 Several factors account for male infertility, ranging from physiological, hormonal, and anatomical abnormalities, that lead to erectile dysfunction, premature ejaculation, oligospermia, asthenospermia, azoospermia, teratozoospermia, non-obstructive azoospermia, and sperm DNA damage. 2 The sperm count fewer than 20 million, which indicates oligospermia. Under normal circumstances, a healthy male should have sperm counts from 40 to 50 million. Oligospermia is one of the factors responsible for more than 25% of total infertility. 3 The World Health Organization (WHO) recently reclassified levels lower than 15 million as oligospermia. 4 Asthenospermia is another condition which is resulting in 50% non-motile sperm, possibly leading to infertility. 5 However, non-obstructive azoospermia is a complete absence of spermatozoa in the ejaculate due to intrinsic and gonadal causes. 6 Teratospermia is the less-than-abnormal morphology of more than 70% spermatozoa. 7
In addition to these sperm deformities and abnormalities, varicocele is a common pathophysiological condition that influences all the above-defined causes of male infertility. Varicocele is defined as the dilated veins (varicose veins) of the testicles predominant on the left side. 8 Varicocele is a common condition responsible for male infertility, and its repair profoundly improves male fertility. 9 Clinically, varicocele is divided into three clinical grades—grade 1: palpable varicose vein upon Valsalva maneuver; grade 2: varicocele is a varicose vein without the Valsalva maneuver; and grade 3: a visible varicose vein through the scrotal skin and upon standing without the Valsalva maneuver. 10 This study back then established the influence of varicocele on male fertility as a massive 25.4% of infertile males had varicocele. 11 Multiple factors lead to varicocele-induced infertility, including increased temperature of the testicles, hormonal imbalance, increased venous pressure, and reactive oxygen species (ROS). Pooling of blood may elevate the temperature of the testicles and affect spermatogenesis. 12
Varicoceles affect different age groups regardless of race and region.13, 14 Delays in diagnosis and treatment result in compilations that may be uncurable later on. 15 Various non-invasive methods are used to diagnose varicocele in male patients, the simplest being physical examination and the most complex being color Doppler sonography, contact thermography, and radionuclide angiography. 16 Both pharmacotherapeutic and surgical treatment options are available for varicocele-related infertility. Herbal supplements, vitamins, hormone replacement therapy, and surgical interventions are the standard procedures implemented to treat varicoceles.17–21 The Valsalva maneuver is a specialized procedure of forced breathing where excessive pressure is exerted on various body parts, with effects like increased blood pressure and heart rate. 22 To date, various interventions have been implemented to improve the condition of patients suffering from varicoceles, ranging from invasive procedures to supplements. However, to date, there is limited consensus on the effectiveness and quality of the clinical studies aiming to treat and improve the outcome of patients suffering from varicoceles. Varicocelectomy is the only treatment available up till now to resolve infertility problems induced by varicocele. Furthermore, other pharmacotherapeutic adjuncts can be used as a treatment choice concomitantly with surgical intervention. There is a need of an hour for sufficient evidence generation for varicocele-induced male infertility and a comparison of various pharmacotherapeutic options available after varicocelectomy. This systematic review aims to summarize the evidence on the various clinical trials and post-varicocelectomy recovery for patients consuming different supplements or regimens.
Methodology
A systematic search of the literature in health sciences databases, mainly Medline and PubMed, was conducted to identify the main research articles that are relevant to the aims of this research. The search was done using the Medical Subject Headings (MeSH) terms of Varicocele and/or Varicocele and male fertility, Varicocelectomy; Varicocele and/or teratozoospermia, oligospermia, and Pharmacotherapy of varicocele. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used as the main principle to conduct this review.
Selection Criteria
All clinical trials published in the English language were considered for this evidence-generation exercise. Only those studies which involved a properly defined intervention (medical or pharmacotherapy-based intervention) were considered for inclusion. Only studies with a confirmed diagnosis of varicocele were considered for inclusion. All observational studies and any study published in a language other than English were excluded from consideration.
Data Extraction
The data extraction from the selected studies was conducted using a standardized Excel sheet. The prime focus of the data extraction was on the characteristics of studies, nature of intervention and control, patients’ details, disease classification, and other biomarkers relevant to the improvement of varicocele.
Outcomes and population that are explored in this systematic review:
Population of interest (P) = Male patients with varicoceles;
Intervention (I) = Any intervention in modern medicine/supplements or complementary and alternative medicines;
Comparator (C) = Placebo or any comparator whose effect was compared with the intervention;
Outcome (O) = Improvement in the level of hormones, physiology, and morphology of sperms or conception or gestation.
Quality Assessment of Studies and Data Analysis
To estimate the quality of the included trials, the Cochrane Risk of Bias tool was used. 23 This criterion assesses the quality of the clinical trials using this tool and addresses six domains of studies to determine the risk of bias: sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting, and other issues. Each of these items in the tool was labeled as “high risk,” “low risk,” or “unclear risk.”
Results
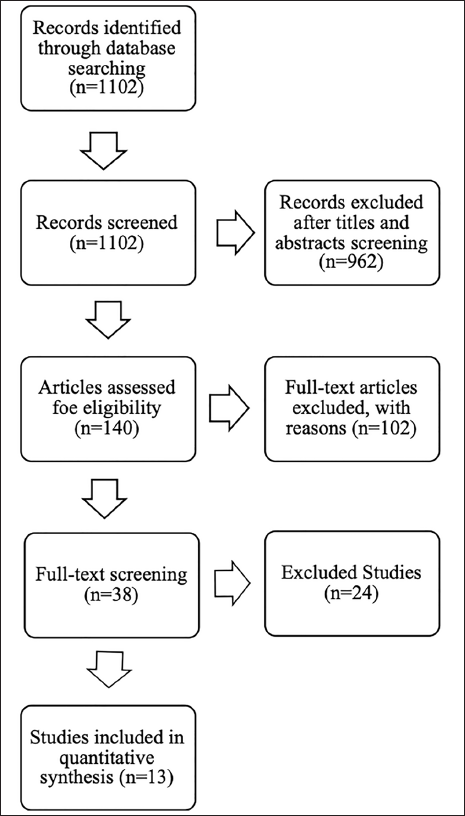
Upon performing the initial search at PubMed and Medline, N = 1,102 papers were identified using the MeSH terms outlined in the “Methodology” section. Of these studies, upon applying the inclusion and exclusion criteria, n = 13 papers were found eligible for inclusion in this study. Details are described in Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Flow Diagram.
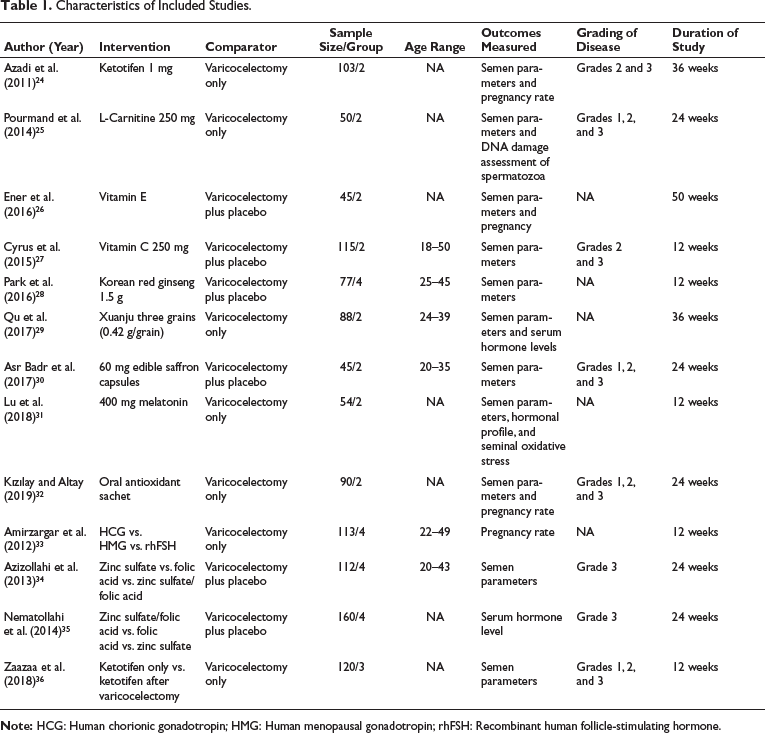
A variety of interventions were used among the included studies during the post-varicocelectomy. These mainly include zinc sulfate/folic acid versus folic acid versus zinc sulfate, ketotifen only versus ketotifen after varicocelectomy, ketotifen 1 mg, l-carnitine 250 mg, vitamin E (VIT E), vitamin C (VIT C) 250 mg, Korean red ginseng 1.5 g, Xuanju three grains (0.42 g/grain), 60 mg saffron capsules, 400 mg melatonin, antioxidant sachet, human chorionic gonadotropin (HCG) versus human menopausal gonadotropin (HMG) versus recombinant human follicle-stimulating hormone (rhFSH), zinc sulfate versus folic acid versus zinc sulfate/folic acid. In most of the cases, grades 1, 2, and 3 patients were included among these 13 studies. Details are shown in Table 1.
Characteristics of Included Studies.
Impact of Interventions on Sperm Count
Sperm count was addressed as a primary outcome among eight studies. Most of these studies have compared the effect of the intervention in both control and intervention groups pre- and post-varicocelectomy. A variety of supplementations were used as intervention, that is, oral l-carnitine 250 mg (for 24 weeks), oral VIT E 300 mg (50 weeks), oral VIT C 250 mg for 12 weeks, oral Korean ginseng 500 gm (12 weeks), oral saffron capsules 60 mg (24 weeks), Oral melatonin 400 mg (12 weeks), VIT C 10 mg of ZnO 200 µg folic acid 50 µg and vitamin B12 (VIT B12) for (24 weeks) and 1 mg ketotifen for 12 weeks. Details are described in Table 2.
Quantitative Parameters of the Included Studies on Sperm Count.
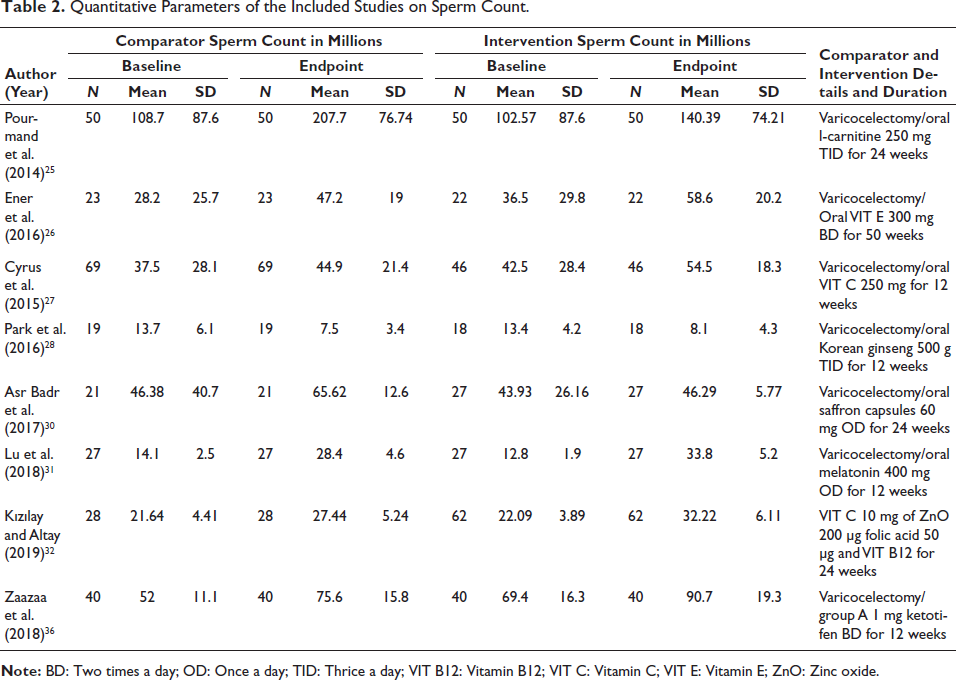
Overall, in comparison to the baseline parameter, a very substantial increase in sperm count was observed at the endpoint assessment for the groups consuming l-carnitine and VIT E supplementation. It was observed that the increase in sperm count for the l-carnitine users as a post-varicocelectomy intervention was 37.82 × 10 6 from the baseline values; for VIT E, it is observed to 22.1 × 10 6 from the baseline values.
Impact of Interventions on Sperm Motility
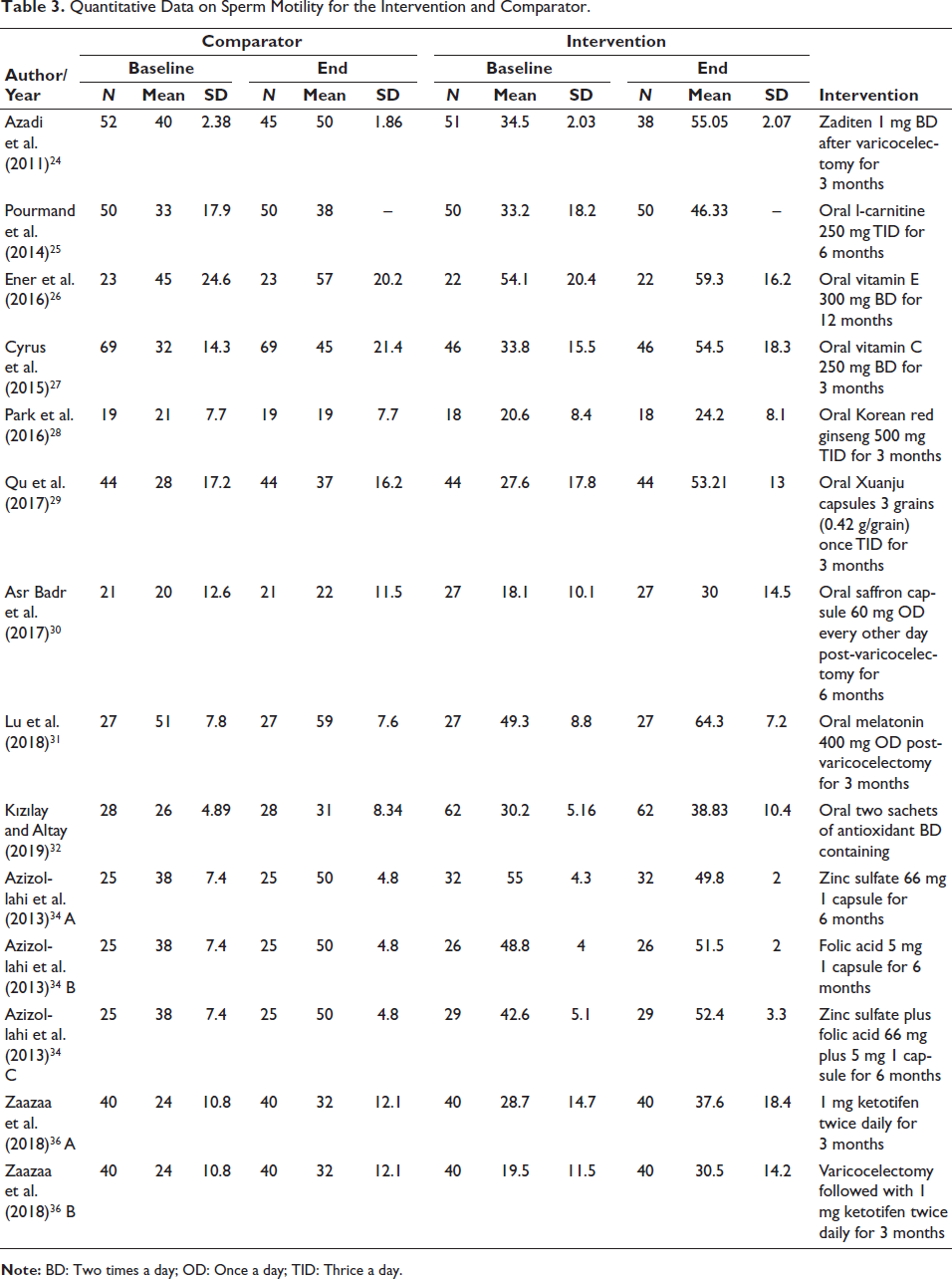
The number of studies measuring the outcome percentage of sperm motility pre- and post-varicocelectomy in both control and interventional groups was n = 11. The most common parameter measured in all studies was the percentage of motile sperm cells. A comparison of the percentage of motile sperm cells between the baseline and end values of both the control and interventional groups showed that the percentage of motile spermatozoa was markedly increased in the interventional group than in the control. This shows that like sperm count, the percentage of motile sperm cells also had a marked effect of that adjunct pharmacotherapeutic intervention.
A study performed by Azizollahi et al. 34 divided the participants into three groups: group A received zinc sulfate 66 mg, 1 capsule for 6 months; group B received folic acid 5 mg, 1 capsule for 6 months; group C received zinc sulfate plus folic acid 66 mg plus 5 mg, 1 capsule for 6 months, all of these interventional groups had same controls, that is, only varicocelectomy. The study performed by Zaazaa et al. 36 divided the groups into two groups: group A received 1 mg ketotifen twice daily for 3 months, and group B received varicocelectomy followed by 1 mg ketotifen twice daily for 3 months. These two studies had five subgroups randomized and assessed adjunct pharmacotherapeutic intervention’s efficacy. These studies confirmed the results of nine other studies in improving the percentage of motile sperm. The summary is shown in Table 3.
Quantitative Data on Sperm Motility for the Intervention and Comparator.
Sperm with Normal Morphology %
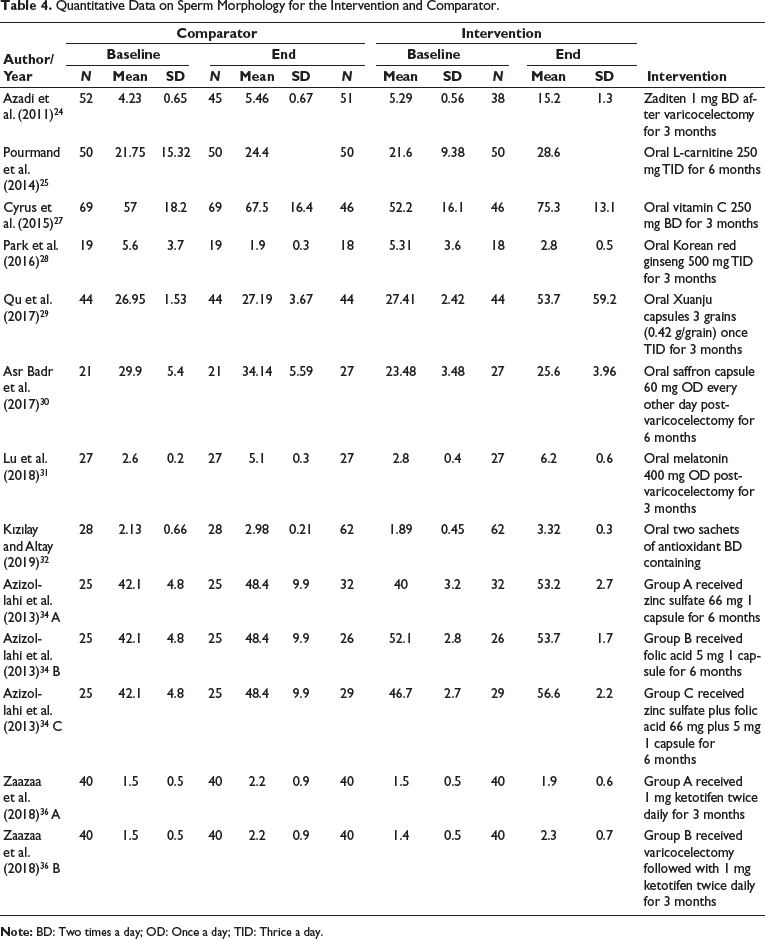
Out of all the included studies, n = 14, only n = 10 studies assessed the outcome of sperms with normal morphology % pre- and post-varicocelectomy in both control and interventional groups. All the studies assessed the percentage of sperm with normal morphology in control groups with only surgical intervention and the interventional group with the adjunct pharmacotherapeutic intervention post-varicocelectomy. Results confirmed the previous results as the percentage of normal sperms increased significantly in interventional groups than in controls. The study performed by Nematollahi-Mahani et al. 35 further divided the interventional groups into three groups: group A received zinc sulfate 66 mg 1 capsule for 6 months, group B received folic acid 5 mg 1 capsule for 6 months, and group C received zinc sulfate plus folic acid 66 mg plus 5 mg 1 capsule for 6 months as described in sperm motility as well. The study performed by Zaaza et al. 36 divided the interventional group into further two subgroups. The summary is shown in Table 4.
Quantitative Data on Sperm Morphology for the Intervention and Comparator.
Impact of Interventions on Semen Volume
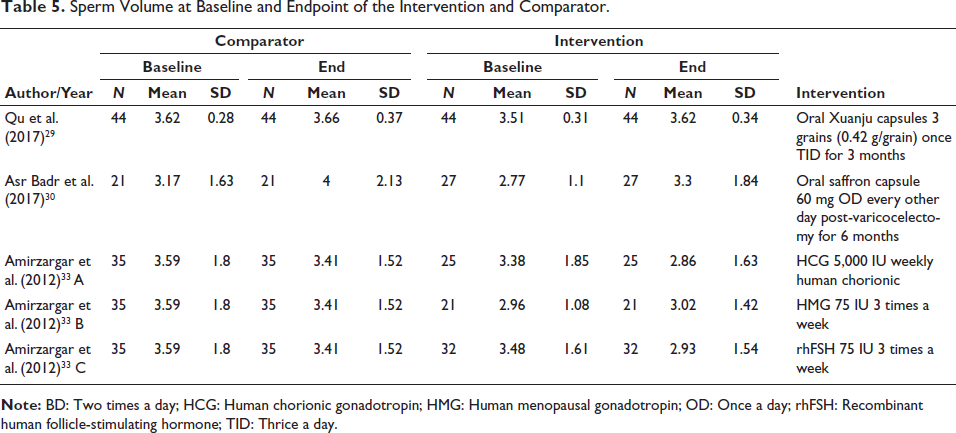
Among the finalized studies, n = 3 discussed and compared semen volume as a main outcome.29, 33 Findings from the study of Qu et al. showed a statistically non-significant increase in the semen volume in comparison to the baseline results. 29 However, results from Amirzargar et al. 33 showed inconclusive results for the use of adjunct supplementation of HCG, and semen volume decreased in both control and interventional groups pre- and post-varicocelectomy. This showed that adjunct pharmacotherapeutic interventions had no significant effect on semen volume. The summary is shown in Table 5.
Impact of Interventions on Sperm Density
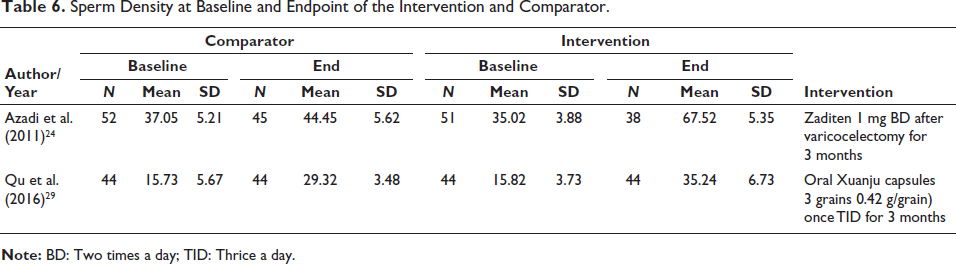
Only two studies discussed sperm density as an outcome assessed pre- and post-varicocelectomy in both the control and interventional groups. Studies discussing sperm density were the result from these two studies have shown a significant increase in sperm density in both groups.24, 29 However, the increase in sperm density in the interventional group was more significant than in the control, showing that adjunct pharmacotherapeutic intervention markedly affected sperm density. The summary is shown in Table 6.
Sperm Volume at Baseline and Endpoint of the Intervention and Comparator.
Sperm Density at Baseline and Endpoint of the Intervention and Comparator.
Impact of Interventions on the Hormonal Profile of Patients
Exploration in this regard has shown the main three hormones that were investigated in the selected studies: testosterone, follicle-stimulating hormone (FSH), and luteinizing hormone (LH).28, 29, 35 Three studies have investigated the impact of the intervention on testosterone. Two studies have shown an increase in the level of testosterone in both the control and interventional groups.28, 29 However, the increase was not significant, and the last study assessed zinc sulfate and folic acid as adjunct pharmacotherapeutic interventions and showed a decrease in the testosterone level. This reveals that the adjunct pharmacotherapeutic intervention did not affect the level of testosterone pre- and post-varicocelectomy.
Interventions having oral Korean red ginseng 500 mg TID for 3 months and oral Xuanju capsules 3 grains (0.42 g/grain) once TID for 3 months post-varicocelectomy interestingly showed a decrease in FSH level after surgery in the interventional group. 35 Two studies assessed the levels of LH in both control and interventional groups.28, 29 Both studies displayed a decrease in the levels of LH post-varicocelectomy interestingly in both groups. The decrease was significant in the interventional group compared to the control group. Furthermore, a decrease in LH levels is considered a factor in improving fertility status in males.
Quality of Studies
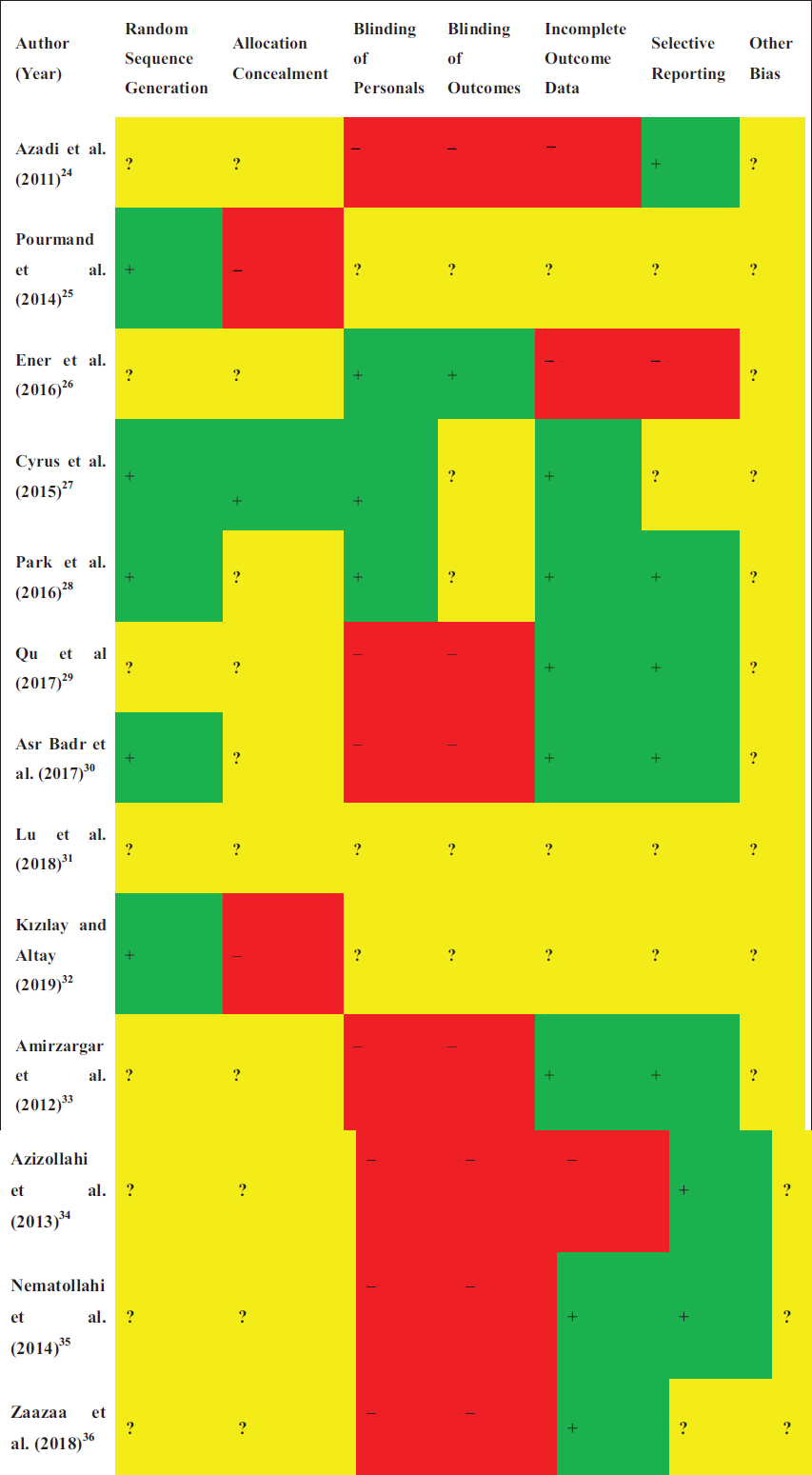
Cochrane risk of bias criteria was used to assess the risk of bias among the included studies. It was observed that overall, the blinding of personnel and the blinding of outcomes were observed to be the main areas with a higher risk of bias among the selected studies. Details are shown in Figure 2.
Quality of the Selected Studies.
Discussion
One of the most contentious issues surrounding male infertility is varicocele. While the majority of international fertility societies concur that virtual reality (VR) should be used when a man is infertile and has a clinically detectable varicocele and abnormal semen parameters,37–39 some medical professionals continue to have doubts about varicocelectomy’s positive effects on semen parameters and reproductive status.40–42 The present study is primarily assessing the impact of supportive pharmacological and supplemental care among post-varicocelectomy patients.
In summation of the results, it was observed that ketotifen supplementation has shown significant improvement in semen parameters, chromatin integrity, and pregnancy rates. Cumulative pregnancy significantly improved in the treatment group compared to the control group, except for DNA integrity. 24 For the improvement of the DNA damage, it was observed that 750 mg of l-carnitine and mast cell stabilizers improved the semen analysis and DNA integrity compared to the comparator; however, the improvement in DNA integrity was not statistically significant.25, 36 However, due to the limited number of studies, it remains challenging to recommend any of the measures above as a first-line regimen for the post-varicocelectomy management of patients.
A variety of supplements, that is, VIT E and VIT C, were also investigated among post-varicocelectomy patients. It was observed that these supplements were found to have a positive impact on parameters like sperm count, percentage of change in sperm count, motile sperm count, and percentage of change in motile sperm count.26, 27 However, antioxidant treatment increases the likelihood of getting pregnant and has a significant impact on varicocelectomy results. 32 One may draw the conclusion that co-administering folic acid and zinc greatly enhanced sperm parameters and improved varicocelectomy results. Therefore, following surgery, medical therapy with appropriate medications may be beneficial for getting satisfactory results on hormonal and sperm parameters.34, 35
Korean ginseng was also investigated for its effect on the serum levels of testosterone, LH, and FSH did not differ significantly between the groups though. Korean ginseng may be a helpful treatment for male infertility; however, its impact on spermatogenesis may need to be clarified. 28 Xuanju capsule and the effect of the therapy on levels of sex hormone and anti-sperm antibody (AsAb) was also assessed in comparison to the control group. The group receiving Xuanju had a substantially higher rate of clinical efficacy, 84.09%. In addition, sperm density, percentage, and sperm survival rate were all significantly greater in the Xuanju supplementation group. Conclusions: Xuanju capsules were observed to have a significantly higher semen quality and level of sexual hormones as well as lower serum AsAb levels in comparison to the control group. 29 Similar assessment was performed among infertile males with clinical varicocele following varicocelectomy using saffron as a herbal supplement. Saffron improves sperm motility but does not affect other semen parameters. 30 When comparing the melatonin group to the placebo group, there were statistically significant improvements in the post-operative parameters of semen analyses (sperm concentration, motility, and proportions of normally produced spermatozoa), peripheral blood inhibin B, and total antioxidant capacity. Thus, can be used as a recommended regimen in the post-varicocelectomy patients. 31
The effect of rhFSH, HCG, and HMG was also assessed. It is proven that these hormones may shorten the period needed to induce spermatogenesis and fertility when compared to varicocelectomy alone. Compared to other medications, rhFSH is more useful for these objectives. 33 When comparing the melatonin group to the placebo group, there were statistically significant improvements in the post-operative parameters of semen analyses (sperm concentration, motility, and proportions of normally produced spermatozoa), peripheral blood inhibin B, and total antioxidant capacity. Thus, it can be used as a recommended regimen in the post-varicocelectomy patients. 31
There was no evidence of publication bias in the analyzed papers on sperm volume, total sperm count, total sperm motility, and normal morphology. No investigation was sensitive enough to affect the conclusion of our findings regarding sperm concentration and progressive motility. Researchers who are against using varicocelectomy to treat male infertility primarily fear that, even in the absence of treatment, semen quality may naturally increase. A lack of a suitable control group resulted in poor analysis, which prevented several researchers from taking this issue into account. 41 Results of the current systematic review have shown a significant improvement after varicocelectomy, specifically in the case when various supplements and anti-inflammatory agents had a very fruitful effect on sperm count and motility, but this was not statistically significant. Furthermore, keeping in view the current evidence-based synthesis guidelines, there is an immediate need for more well-planned studies with selective control groups so that the entire effect of the intervention can be assessed scientifically.
Conclusion
Selected studies in the review have revealed improvements in the various physical and morphological markers associated with sperm and other parameters associated with fertility among men. However, the main limitation observed in the published scientific data is the limited studies on the supplements that are used in the post-varicocelectomy. To begin with, not all RCTs met the requirements to be included in the analysis. Second, all tested outcomes showed high heterogeneity. Third, research examining the effect of VR on sperm concentration and progressive sperm motility showed notable results, but several studies are lacking to conclude using the effect size of the selected intervention.
Limitations and Implications of This Research
One of the main limitations of this study is the lack of quantitative comparison, which was unfortunately not possible due to differences and deficiencies across the different studies and the parameters they measured as an outcome. The rest of this study has given the researchers a new perspective on exploring the impact of various pharmacotherapy regimens as adjunct therapies for managing varicoceles.
Footnotes
Abbreviations
AsAb: Anti-sperm Antibody; BD: Two times a day; FSH: Follicle-stimulating hormone; HCG: Human chorionic gonadotropin; HMG: Human menopausal gonadotropin; LH: Luteinizing hormone; MeSH: Medical Subject Headings; PICOT: Population, intervention, comparator, outcome; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCTs: Randomized clinical trials; ROS: Reactive oxygen species; TID: Thrice a day; VIT B12: Vitamin B12; VIT C: Vitamin C; VIT E: Vitamin E; VR: Virtual reality; WHO: World Health Organization; ZnO: Zinc oxide.
Acknowledgments
None.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Not applicable.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.