
Abstract
Background
Oral cancer is a significant global burden in the present scenario, and early detection has critical importance in improving the survival rate. Devices which aid in the early diagnosis of dysplastic lesions non-invasively are necessary to reduce the oral cancer burden and improve the quality of life of the patients.
Objectives
To evaluate the efficacy of DrOroscope in diagnosing dysplasia in oral mucosal lesions.
Methodology
A cross-sectional study was conducted among 40 individuals clinically diagnosed with oral mucosal lesions from various demographics in Hyderabad. Participants were screened using the DrOroscope device, which detects dysplastic changes via fluorescence imaging analyzed by artificial intelligence algorithms. Based on the image analysis, lesions were categorized as variable, borderline, or severe. Confirmatory biopsies were performed on all examined lesions, with histopathological results as the gold standard. Statistical analyses, including Chi-square tests, Fisher’s exact test, Cohen’s kappa, and receiver operating characteristic (ROC) curve analysis, were conducted using SPSS version 26.0 with a confidence interval at 95% and p < 0.05 significance.
Results
DrOroscope exhibited a sensitivity of 100.00% and a specificity of 69.23%. Positive predictive value was 87.10%, negative predictive value was 100.00%, and overall diagnostic accuracy was 90.00%. Cohen’s kappa value for agreement between DrOroscope and biopsy results was 0.752, indicating substantial agreement, and 0.539 for detecting dysplasia levels, indicating moderate agreement. The ROC curve analysis supported these findings, demonstrating excellent diagnostic performance.
Conclusion
The DrOroscope device is highly sensitive and accurate in detecting dysplastic changes in oral lesions, making it a promising adjunctive non-invasive diagnostic tool, especially in screening larger populations. This aids in the early diagnosis of dysplasia and thus reducing patients’ morbidity. However, further refinement and larger studies are needed to improve agreement with biopsy for grading of dysplasia.
Clinical Significance of the Study
DrOroscope plays a promising role in the early diagnosis of dysplasia. This can have a huge impact on the treatment plan, thereby improving the quality of life of the patient. Such devices play a crucial role in oral cancer screening programs, thus promoting awareness on early detection of oral cancer and also enhancing the effectiveness of oral cancer prevention.
Introduction
Oral cancer is a significant public health issue in India, characterized by high incidence and mortality rates. The incidence of oral cancer has been rising in India and hence there is a growing demand for non-invasive diagnostic tools for the early diagnosis of dysplasia and malignancies in the oral cavity. Despite the critical importance of early detection, participation in oral cancer screening remains alarmingly low. According to the National Family Health Survey (NFHS-5), only 0.9% of women and 1.2% of men have undergone oral cancer screening. 1 The Government of India has initiated population-based screening programs for oral, breast, and cervical cancers. These programs employ visual inspection methods conducted by trained health workers. However, the uptake of these screenings is insufficient. Community-based screening programs, such as those conducted in the Ranipet district of Tamil Nadu, have demonstrated that systematic visual and oral screenings can effectively identify potentially malignant and malignant lesions. These programs boast a sensitivity of 88% and a positive predictive value (PPV) of 61%. 2
Innovative adjunct screening tools are being explored to improve early detection rates. Tools like fluorescence visualization (FV) and DNA image cytometry (DNA-ICM) have shown promise in high-risk clinics and are being evaluated for use in rural settings. Additionally, the prevalence of oral potentially malignant disorders (OPMDs) is notably higher among people living with HIV (PLHIV) who use smokeless tobacco, underscoring the need for targeted screening strategies in this high-risk group. 3
Training programs, such as Project ECHO, have effectively enhanced the knowledge and skills of primary care physicians in cancer screening. However, further support is needed to implement these clinical services more broadly. Despite these efforts, the overall participation in cancer screening in India remains extremely inadequate, highlighting the necessity for increased public awareness and well-organized screening programs to ensure broader coverage and early detection. 4
While conventional clinical examination and histopathology remain the standard approach for the diagnosis of oral cancer, the former lacks the potential for early detection of dysplasia. Not all patients are compliant with invasive procedures such as a biopsy. Early diagnosis of dysplasia not only adds up to a better prognosis and survival rate but also alleviates the psychological and financial burden of the patient. Therefore, the need for an efficient non-invasive diagnostic tool that plays a crucial role in oral cancer community screening programs has spiked. One promising tool in the fight against oral cancer is the DrOroscope. This novel device is specifically designed for the early detection of dysplastic lesions. The DrOroscope is a portable, intraoral non-invasive diagnostic tool designed to detect dysplasia based on the autofluorescence principle. Upon exposure of the lesion to blue light, green fluorescence indicates normal tissue, while a loss of fluorescence indicates dysplasia. The novelty of the device lies in its intraoral approach and image analysis. Images taken by DrOroscope were analyzed using software algorithms generated from artificial intelligence (AI) concepts. By integrating such innovative technologies into screening programs, India can enhance its early detection and intervention capacity, ultimately reducing the burden of oral cancer. 5
While participation in oral cancer screening in India is currently low, advancements like the DrOroscope offer a promising avenue to improve early detection rates. Combined with increased public awareness and well-organized screening programs, these innovations can significantly enhance the effectiveness of oral cancer prevention and control efforts in India. The study aims to evaluate the efficacy of DrOroscope in diagnosing dysplasia in suspicious oral mucosal lesions. Evaluating the lesions with DrOroscope and comparing the image analyses with the standard histopathological results remain the objectives of the study.
Methodology
The study methodology involved screening the general population, and patients with oral mucosal lesions were examined using the DrOroscope device, followed by confirmatory biopsies to evaluate the effectiveness and accuracy of the device in detecting dysplasia. The study was conducted in accordance with ethical standards and received approval from the Institutional Review Board (IRB) of Panineeya Dental College, Hyderabad (PMVIDS&RC/IEC/OM/PR/0348-2019). Written informed consent was obtained from all participants prior to the study. Participants were thoroughly informed about the study’s purpose, procedures, potential risks, and benefits. Participant information was confidential, and data were anonymized to protect privacy. The study adhered to the ethical principles outlined in the Declaration of Helsinki, ensuring the safety and well-being of participants throughout the screening and biopsy procedures. Additionally, participants were given the right to withdraw from the study at any point without any repercussions.
Study Design
Study Population
A cross-sectional study was conducted involving 40 individuals with oral mucosal lesions selected from various demographics, including urban, rural, and high-risk populations. The patients were examined with DrOroscope when camps were organized in and around Hyderabad. Participants were recruited from areas with varying participation rates in screening camps.
Inclusion and Exclusion Criteria
Individuals aged 18 years and above clinically diagnosed with red, white, or mixed oral mucosal lesions were included in the study and those individuals with previously diagnosed oral cancer or who had undergone recent oral surgeries and were not willing to participate in the study were excluded.
Screening Procedure
Examination with DrOroscope
Participants were screened for oral mucosal lesions, and those lesions were subjected to DrOroscope examination focusing on identifying dysplastic lesions. The examiner was trained in the operation of DrOroscope and interpreting its results. On blue light exposure, the normal tissues reflect green fluorescence, and there is a loss of fluorescence in abnormal tissues, due to which the areas appear dark. The pictures were captured with the image sensor. Image analysis was done using software algorithms generated from AI concepts. After a thorough image analysis by DrOroscope, the lesions were categorized into variable, borderline, and severe. Lesions with no dysplastic changes, mild and moderate dysplastic changes, and severe cases were categorized under variable, borderline, and dysplasia, respectively.
Documentation and Data Collection
Detailed records of each screening were maintained, including demographic information, risk factors, and findings from the DrOroscope. Images captured by the DrOroscope were analyzed in real-time and stored for further evaluation.
Confirmatory Biopsy
The lesions examined under DrOroscope were referred for a confirmatory biopsy. A trained oral surgeon or pathologist performed the biopsy, collecting tissue samples from the identified lesions. Collected biopsy samples were sent to a pathology lab for histopathological examination. The histopathological results served as the gold standard for confirming the presence of dysplasia among the lesions.
Statistical Analysis
To analyze the data, SPSS (IBM SPSS Statistics for Windows, version 26.0, Armonk, NY: IBM Corp. Released 2019) was used. The sensitivity (the ability to correctly identify true positives) and specificity (the ability to correctly identify true negatives) of DrOroscope were calculated by comparing their findings with the biopsy results. Statistical analysis was used to determine the PPV, negative predictive value (NPV), and accuracy of DrOroscope. The Chi-square test was applied to compare proportions between different groups; if any expected cell frequency was less than five, Fisher’s exact test was used. The agreement between DrOroscope and biopsy results was analyzed using Cohen’s kappa. Receiver operating characteristic (ROC) curve analysis was done for diagnostic procedure performance.
Results
Among the 40 participants, 26 were males and 14 females in the study. The mean age was slightly higher among females (48.4 years) than males (47.1 years), resulting in an overall mean age of 47.6 years. Standard deviations were 13.7 years for males and 10.6 years for females, indicating a wider age range among males. Median ages were 47.0 years for males and 50.0 years for females, with an overall median of 47.0 years. The minimum and maximum ages were 27.0 years to 71.0 years for males and 27.0 years to 65.0 years for females, with an overall maximum age of 71.0 years (Table 1).
Distribution of Participants Based on Age and Gender.
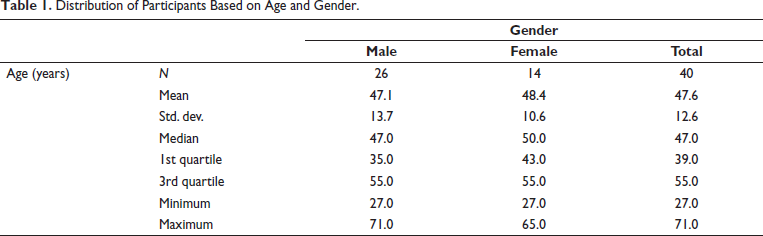
Figure 1 summarizes the symptoms reported by the participants. A majority (52.5%, 21 participants) reported no symptoms. The most common symptom was a burning sensation, reported by 32.5% (13 participants). Reduced mouth opening was reported by 5.0% (2 participants), and 7.5% (3 participants) experienced both burning sensation and reduced mouth opening. Other symptoms were reported by 2.5% (1 participant).
Receiver Operating Characteristic (ROC) Curve of DrOroscope.
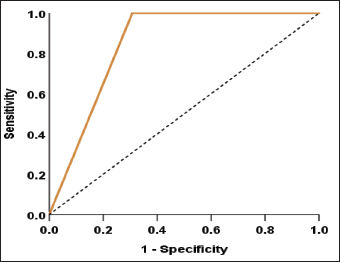
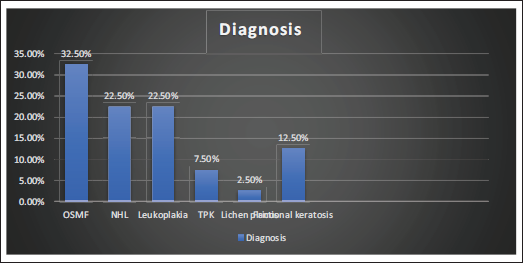
Figure 2 outlines the distribution of diagnoses among the 40 patients. Oral Submucous Fibrosis (OSMF) was the most frequent diagnosis, affecting 32.5% (13 individuals). Nonhomogeneous leukoplakia (NHL) and homogenous leukoplakia each accounted for 22.5% (9 individuals), followed by keratotic lesions and tobacco pouch keratosis (TPK) at 12.5% (5 and 3 individuals, respectively). Lichen planus was identified in one patient.
Frequency Distribution of Symptoms Among the Participants.
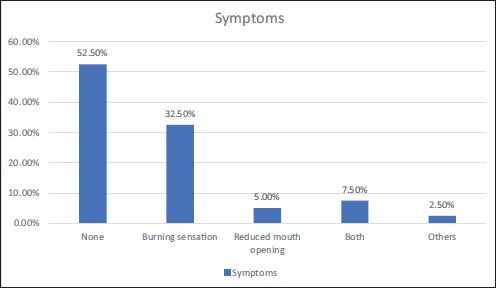
Table 2 presents the biopsy results categorized into no dysplasia, mild dysplasia, and moderate dysplasia for different clinical diagnoses and symptoms. The distribution of these categories across OSMF, NHL, leukoplakia, frictional keratosis, TPK, and lichen planus is shown. Additionally, the table outlines the correlation between symptoms such as no symptoms, burning sensation, reduced mouth opening, and other symptoms with dysplasia levels. The p values highlight the statistical significance of the differences observed in the distribution of dysplasia levels among different diagnoses and symptoms, with significant values marked (*p < .05).
Distribution of Oral Mucosal Lesions and Symptoms Among Varying Dysplasia Grades.
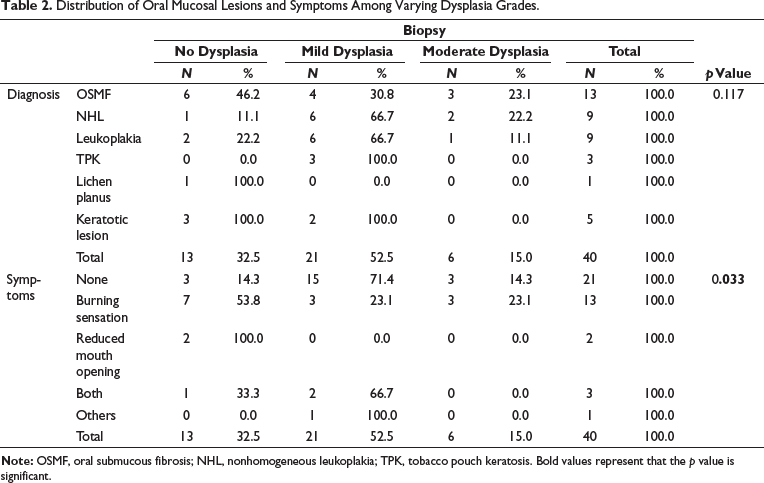
Table 3 displays the agreement between biopsy results and DrOroscope findings regarding the presence or absence of a condition. Out of the total 40 cases, DrOroscope correctly identified 9 cases as negative for the condition, all confirmed by biopsy. For positive results, DrOroscope identified 31 cases, with biopsy confirming 27 cases and identifying 4 cases as negative. These four cases were falsely identified as positive by DrOroscope. This suggests that the test may occasionally incorrectly classify negative cases as positive.
Agreement Between DrOroscope and Histopathology.

Cohen’s kappa value for this agreement is 0.752, indicating a substantial agreement between DrOroscope and biopsy results. The p value less than .001 confirms that this agreement is statistically significant. This analysis underscores the reliability of DrOroscope in diagnosing the condition compared to biopsy results.
Table 4 presents the agreement between the DrOroscope procedure and biopsy results, focusing on detecting different levels of dysplasia. The histopathological results were categorized into no dysplasia, mild dysplasia, and moderate dysplasia. Of the 40 cases, DrOroscope identified 9 variable cases confirmed by biopsy as no dysplasia. DrOroscope identified 17 cases of borderline dysplasia, with the biopsy confirming 14 mild dysplastic cases, 1 with moderate dysplasia, but 2 cases were not dysplastic under histopathological examination. DrOroscope identified 14 dysplasia cases, of which 7 were mild dysplasia, 5 were moderate dysplasia, and 2 were non-dysplastic histopathologically.
Agreement of Various Grades of Dysplasia of DrOroscope with Biopsy Results.
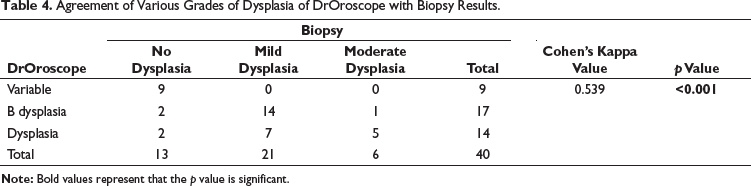
The agreement between the two procedures was quantified using Cohen’s kappa value, which was 0.539, indicating a moderate level of agreement. The p value for this agreement was less than 0.001, suggesting that the agreement is statistically significant. This analysis underscores the reliability of DrOroscope in detecting various grades of dysplasia when compared to the biopsy results.
Table 5 presents key diagnostic performance metrics of a test or procedure, along with their corresponding estimates and 95% confidence intervals (CI). The test’s sensitivity, which measures its ability to correctly identify individuals with the condition, is estimated at 100.00%, with a CI ranging from 87.54% to 100.00%. Specificity, indicating the test’s ability to identify individuals without the condition correctly, is estimated at 69.23%, with a CI of 42.37%–87.32%. The PPV, which indicates the probability that a positive test result accurately indicates the presence of the condition, is estimated at 87.10%, with a CI ranging from 71.15% to 94.87%. The NPV, indicating the probability that a negative test result accurately indicates the absence of the condition, is estimated at 100.00%, with a CI from 70.08% to 100.00%. Overall diagnostic accuracy, representing the proportion of correct test results, is estimated at 90.00%, with a CI of 76.95%–96.04%. These metrics collectively provide a comprehensive assessment of the test’s reliability and effectiveness in clinical diagnosis, supported by the respective CIs that reflect the precision of these estimates.
Diagnostic Performance Metrics.
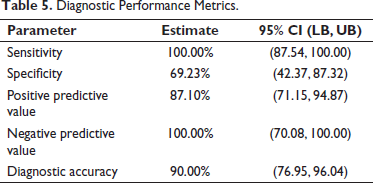
Figure 3 is a ROC curve. It is a graphical representation that illustrates the diagnostic performance of a binary classifier system as its discrimination threshold is varied. In a ROC curve, the true positive rate (sensitivity) is plotted against the false positive rate (1-specificity) for different threshold settings.
Frequency Distribution of Various Oral Mucosal Lesions.
Discussion
Oral squamous cell carcinoma (OSCC) is considered a significant public health concern on a global scale, with a prevalence that is particularly notable among the population of India, affecting both men and women, as highlighted in the data from the National Cancer Registry Program. The incidence of OSCC accounts for a substantial percentage, ranging from 84% to 97%, of all oral cancer cases. 6 The development of OSCC is often linked to the presence of potentially malignant lesions or arising from normal epithelial cells. These potentially malignant disorders (PMDs), such as oral submucosal fibrosis, erythroplakia, leukoplakia, candidal leukoplakia, dyskeratosis, and lichen planus, serve as indicators of the preclinical phase of oral cancer as these lesions have high potential in turning to malignancy. The lack of awareness, exposure to harsh environmental conditions, and certain behavioral factors further contribute to the wide disparity in the prevalence of oral cancer globally. The PMDs represent a group of lesions with a high propensity for malignant transformation if not promptly addressed or monitored. 7 This fact supports the case selection that included various oral mucosal lesions such as OSMF, leukoplakia, keratotic lesions, and lichen planus in the study. The subtle changes observed in the clinical presentation of these lesions often necessitate histopathological assessment, causing distress to the patient while awaiting a definitive diagnosis. To minimize the morbidity associated with oral cancer, a novel device known as DrOroscope was developed. 5
DrOroscope is a portable tool that utilizes FV technology by employing blue light (at wavelengths of 400–460 nm) and green, amber light to distinguish abnormal oral tissues from inflammatory tissues that may not be visible under white light. 5 This approach builds upon autofluorescence properties of healthy and abnormal tissues, a concept initially explored with the VELscope. Various factors such as the fluorophore flavin adenine dinucleotide (FAD), histomorphological changes in abnormal tissue, and levels of hemoglobin collectively contribute to the success of using blue light for the precise detection of tissue abnormalities, including dysplasia and cancer. The concept of tissue autofluorescence and its potential application in cancer detection dates back to 1924, with naturally occurring fluorochromes like collagen, elastin, keratin, FAD, and nicotinamide adenine dinucleotide (NADH) in the epithelial cell lining and submucosa of the oral cavity exhibiting fluorescence in the green spectral range upon excitation with light between 375 and 440 nm. 8 Malignant or dysplastic alterations disrupt the normal tissue fluorescence, leading to FV loss due to changes in the distribution of these fluorochromes.9, 10
The demographic pattern of our study aligns with previous research indicating that oral cancer, particularly OSCC, predominantly affects males in their third to fifth decades of life. Early detection and screening are crucial across different age groups.11, 12
The distribution of diagnoses reveals a significant prevalence of OSMF, affecting 32.5% of the individuals. This aligns with findings from Shah et al., who reported OSMF as the most common precancerous lesion among tobacco consumers, with a prevalence of 70.58% in their study. 13 NHL and homogenous leukoplakia each accounted for 22.5% of the diagnoses, which is consistent with the study by Ashwini and Krishnan, where leukoplakia was predominantly found in the buccal mucosa and had a strong male predilection, particularly among smokers. 14 The presence of frictional keratosis and TPK at 12.5% further supports the findings of Gabhane et al., who identified various tobacco-related lesions, including leukoplakia and TPK, in their clinical evaluations of patients with tobacco habits. 15 Additionally, the identification of lichen planus in one patient corresponds with the study by Vijayan and Muthukrishnan, which highlighted the clinicohistopathological association in diagnosing oral lichen planus (OLP) and its potential for dysplastic changes. 16
The efficacy of DrOroscope in diagnosing dysplasia in OPMDs is a crucial aspect of early detection. While various studies have explored different diagnostic tools like VELscope, autofluorescence examination, and videoroscopy in detecting dysplastic changes in oral lesions, the symptoms reported by participants can also provide valuable insights. In the study, most participants (52.5%) reported no symptoms, the most common being a burning sensation (32.5%). Reduced mouth opening was reported by 5.0% of participants, while 7.5% experienced both a burning sensation and reduced mouth opening. Other fewer common symptoms were reported by 2.5% of participants. 17 This study emphasizes that all the patients need to present with symptoms in dysplastic cases, and there is a necessity for regular screening of the lesions. Understanding both the diagnostic efficacy of tools like DrOroscope and the symptoms reported by individuals can aid in the early identification and management of dysplastic changes in OPMDs.
Cohen’s kappa value of 0.752 and p value less than .001 show that DrOroscope findings are more reliable than biopsy results in diagnosing conditions. This supports other oncology studies emphasizing accurate diagnostic tools. Oral cancer biopsies showed that deep tissue with underlying stroma improves diagnostic success, emphasizing the need for adequate tissue sampling to avoid false negatives. 18 The grading of oral epithelial dysplasia (OED) in oral leukoplakia showed low agreement among pathologists (κ = 0.30), highlighting the need for more objective systems, possibly incorporating AI, to enhance diagnostic consistency. 19 Comparing conventional cytology (CC) and liquid-based cytology (LBC) for oral cancer screening showed similar sensitivities of around 60%, but cellularity and clinical subtype significantly affect false negative rates. 20 These studies demonstrate the importance of accurate and reliable diagnostic tools like DrOroscope in early detection and treatment of various conditions, improving patient outcomes.
In Table 5, the test or procedure’s diagnostic performance metrics show high sensitivity (100.00%, CI: 87.54%–100.00%) and NPV (100.00%, CI: 70.08%–100.00%), indicating that it accurately diagnoses the condition and excludes others. The lower specificity (69.23%, CI: 42.37%–87.32%) and PPV (87.10%, CI: 71.15%–94.87%) suggest that identifying people without the condition may be difficult. The VOE and ZNF582 methylation (ZNF582m) tests detected OED and OSCC better than VOE alone (56.1% and 37.7%). 21 ZNF582m was more sensitive (90.2%) but less specific (44.9%). 21 A systematic review found that autofluorescence had 86% sensitivity and 72% specificity, while chemiluminescence had 67% and 48%. 22
A study conducted by Dania Sawan and Ammar Mashlah found that 9.4% of detected lesions were confirmed as abnormal, while 83.09% exhibited a loss of fluorescent light effect when examined with VELscope. The diagnostic device demonstrated a sensitivity of 74.1% and a specificity of 96.3%, as determined by surgical biopsy results. This device was also designed based on the principle of autofluorescence but the lesions are to be examined extraorally. The present study exhibited a sensitivity of 100.00%, indicating the test’s high effectiveness in detecting cases of the condition. The specificity observed in the current study was 69.23%, which is lower than the findings reported by Sawan and Mashlah, yet still reflects the test’s ability to accurately identify individuals without the condition. Variations in sample characteristics or lesion presentation may account for the differences in specificity. The findings underscore the test’s potential for high-sensitivity screening while indicating a need for enhanced specificity to improve overall diagnostic reliability. 23
In a study conducted by Anupriya Sharma et al., VELscope examination achieved sensitivity and specificity values of 75.00% and 61.39%, respectively, with PPVs and NPVs of 31.58% and 91.18%. In comparison, the present study showed a higher sensitivity of 100.00%, indicating strong accuracy in identifying individuals with the condition. The specificity was 69.23%, showing moderate capability in correctly identifying individuals without the condition. Additionally, the PPV in the study was 87.10%, suggesting that a positive result was highly indicative of the condition’s presence, while the NPV was 100.00%, indicating reliable confirmation of the condition’s absence in negative results. The overall diagnostic accuracy was estimated at 90.00%, underscoring the test’s robust performance in this study, particularly in high-sensitivity applications. 24
The ROC curve is a fundamental tool for evaluating the performance of binary classification systems, particularly in diagnostic tests. In the given scenario, the test demonstrates an excellent sensitivity of 100.00% (95% CI: 87.54%–100.00%), indicating a high ability to identify positive cases, thus rarely missing true positives correctly. However, the specificity is moderate at 69.23% (95% CI: 42.37%–87.32%), suggesting a tendency to misclassify negative cases as positive occasionally. This balance between sensitivity and specificity is crucial for understanding the test’s diagnostic performance. The ROC curve plots the true positive rate (sensitivity) against the false positive rate (specificity) across various threshold settings, visually representing this trade-off. 25 The area under the curve (AUC) is a summarized accuracy index, with higher values indicating better discriminatory ability. 26
Strengths of the Study
The study employs Cohen’s kappa statistic, a reliable measure of inter-rater agreement, to quantify the concordance between DrOroscope and biopsy. It differentiates between positive and negative results, providing a clearer picture of diagnostic accuracy (true positives, false positives, false negatives). Apart from the efficacy of the device, the correlation between various symptoms and clinical diagnoses was made with the histopathological results.
Limitations and Areas for Further Research
The specific condition under investigation is not disclosed, limiting the generalizability of the findings to other conditions. The sample size is relatively small, and larger studies are needed to confirm the reliability of DrOroscope. The study design does not address potential reasons for discrepancies between the grades of dysplasia given by DrOroscope and biopsy results. Future research could explore factors influencing these variations. Studies with larger sample sizes are needed to confirm these findings. Longitudinal studies can track patients over time to assess the prognostic value of DrOroscope findings, examining if early detection correlates with improved outcomes in dysplasia or cancer prevention. Investigating the reasons behind misclassifications, especially for moderate dysplasia, is crucial. Research on improving DrOroscope’s accuracy for specific dysplasia grades is warranted.
In conclusion, this novel non-invasive tool proved to be efficacious in the early detection of dysplasia with a high sensitivity of 100.00% and overall diagnostic accuracy of 90.00%. Cohen’s kappa value for agreement between DrOroscope and biopsy results was 0.752, indicating substantial agreement, and 0.539 for detecting dysplasia levels, indicating moderate agreement. The ROC curve analysis supported these findings, demonstrating excellent diagnostic performance. DrOroscope shows promise as an adjunctive diagnostic tool, particularly for screening larger populations in the early phase of dysplasia and thus aiding in reducing patients’ morbidity. However, further refinement may be needed to improve agreement with biopsy for dysplasia-level identification. Larger studies investigating the agreement across various conditions and exploring the reasons for discrepancies are recommended.
Footnotes
Acknowledgments
We are extremely thankful to Dr Ramaraju Devaraju, CEO of Raamah Biocare Pvt. Ltd. for providing the DrOroscope device needed for the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was in accordance with ethical standards and received approval from the Institutional Review Board (IRB) of Panineeya Dental College, Hyderabad (PMVIDS&RC/IEC/ OM/PR/0348-2019).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from all participants prior to the study.