
Abstract
Background
Rheumatoid arthritis (RA) is a systemic autoimmune disease that imposes significant challenges globally. This research seeks to contribute valuable insights that can inform the development of targeted interventions, enhancing the quality of care for RA patients and potentially mitigating the broader societal burden associated with this chronic autoimmune condition.
Objectives
The main objective of the current study is to investigate the demographic, psychosocial, and clinical aspects of RA patients.
Materials and Methods
The study included 93 RA patients and examined their demographic characteristics, brief-Coping Orientation to Problems Experienced (COPE) strategies, the prevalence of depression and anxiety, pain experiences (Mankoski Pain Scale), and diagnostic markers (Disease Activity Score [DAS-28], Rheumatoid Factor [RF], Anti-Cyclic Citrullinated Peptide [ACCP]).
Results
The study revealed a bimodal age distribution, with a gender predominance aligning with established RA prevalence patterns. Patients exhibited a tendency toward adaptive coping strategies, notably religious coping, active coping, and positive reframing, with variability in maladaptive strategies. The prevalence of depression (14.0%) and anxiety (18.3%) among RA patients was consistent with documented mental health burdens. Pain experiences exhibited a heterogeneous spectrum, and diagnostic markers indicated elevated disease activity in a substantial proportion of patients, with varied distribution in RF and ACCP subcategories.
Conclusion
This study provides nuanced insights into RA, emphasizing the importance of personalized coping and pain management strategies. The prevalence of mental health challenges and the spectrum of pain experiences underscore the multidimensional nature of RA, informing holistic approaches to care for enhanced patient outcomes.
Keywords
Introduction
Rheumatoid Arthritis (RA) is a systemic autoimmune disease that primarily targets the synovium the lining of the joints. Unlike osteoarthritis, RA is not solely a consequence of wear and tear but rather caused by autoimmunity. The result is chronic inflammation, pain, and, if left unmanaged, irreversible joint damage. 1 RA’s impact extends far beyond the individual level, reaching into the global realm of public health. With millions of people affected worldwide, RA stands as a formidable contributor to disability, compromised quality of life, and increased healthcare costs. Globally, there were an estimated 18.5 million prevalent cases of RA, with 1.07 million incident cases per year and almost 2.43 million years lived with disability in 2019. 2 The burden is not limited to physical symptoms; mental health and social aspects are also significantly influenced by the challenges posed by RA. 3 One of the hallmark features of RA is persistent pain, a complex and subjective experience that significantly diminishes the overall well-being of affected individuals. Pain in RA is not only a result of inflammation and joint damage but also a consequence of the intricate interplay between physiological and psychosocial factors.4, 5 Understanding and effectively managing pain in RA patients is paramount to improving their quality of life and mitigating the broader consequences of this debilitating condition. As patients navigate the daily challenges of RA, coping strategies become pivotal in influencing their ability to manage pain and maintain a semblance of normalcy in their lives. Coping mechanisms may encompass a spectrum of approaches, including psychological interventions, lifestyle adjustments, and social support networks. 6 Recognizing the diverse array of coping strategies and their impact on pain intensity is essential for tailoring interventions that can enhance the resilience and overall well-being of individuals living with RA. 7 Medication adherence remains a cornerstone, with strict compliance to prescribed therapeutic regimens essential for managing symptoms and mitigating disease progression. 8 Furthermore, employing pain management modalities, including temperature-based therapies and targeted exercises, proves integral in alleviating pain and ameliorating joint stiffness. 9 Psychosocial interventions, including stress management techniques, participation in support groups, and cognitive-behavioral therapy, are paramount for addressing the emotional toll of RA. 10 Occupational therapy provides tailored guidance on optimizing daily activities, while the judicious use of assistive devices and adaptive equipment enhances functional independence. 11 Striking a balance between rest and activity is underscored, with adaptive clothing and equipment facilitating the mitigation of physical challenges. 12 As such, a comprehensive and individualized approach to coping strategies in RA entails a synthesis of pharmacological, lifestyle, and psychosocial interventions, necessitating ongoing collaboration with healthcare professionals for optimized patient outcomes. This study aims to systematically investigate and identify effective coping strategies employed by individuals with RA, elucidating their impact on pain management and overall well-being. By comprehensively understanding coping mechanisms, this research seeks to contribute valuable insights that can inform the development of targeted interventions, enhancing the quality of care for RA patients and potentially mitigating the broader societal burden associated with this chronic autoimmune condition. Through a rigorous examination of coping strategies, we aspire to optimize patient outcomes and refine clinical approaches tailored to the unique challenges posed by RA.
Materials and Methods
Study Design
A prospective observational study was conducted from November 2019 to May 2020.
Study Department and Site
The study was conducted in the Departments of Rheumatology and Psychiatry at Sri Venkateswara Institute of Medical Sciences, a tertiary care teaching hospital located in Tirupati, Andhra Pradesh, India.
Sample Size
A non-probability sampling method (convenience sampling) was chosen for the sample size calculation. The study included a sample size of 93 participants.
Source of Data
Data collection was performed on outpatients of Rheumatology. Demographic details, including age, gender, diagnosis, co-morbid conditions, and medication information, were extracted from case sheets. Patient interviews, involving the patients and their representatives, as well as relevant sources, were conducted.
Study Duration
The study spanned 6 months, commencing in November 2019 and concluding in May 2020.
Study Criteria
Inclusion Criteria
Participants aged > 18 years.
Newly diagnosed patients with RA based on American College of Rheumatology/European League Against Rheumatism (ACR/EULAR 2010) criteria.
Patients were willing to provide informed consent for study participation.
Exclusion Criteria
Patients were unwilling to participate in the study.
Patients with other connective diseases such as spondyloarthropathy, crystal arthropathy, systemic lupus erythematosus, systemic sclerosis, mixed connective tissue disease, Sjogren’s syndrome, etc.
Study Procedure
Written informed consent was obtained from all subjects (Annexure-I).
Patient data, including demographic information, was collected from both patient interviews and case profiles (Annexure-II).
Pain, coping strategies, anxiety, and depression were assessed using the Mankoski Pain Scale (Annexure-III), Brief-Coping Orientation to Problems Experienced (COPE) (Annexure-IV), and Hospital Anxiety and Depression Scale (HADS) (Annexure-V), respectively.
Statistical Analysis
Data were transcribed from case report forms (CRF) to Microsoft Excel and analyzed using R Studio 1.3. Descriptive statistics outlined demographic characteristics and coping strategies, employing frequencies, percentages, mean ± standard deviation, and median (interquartile range [IQR]) for categorical and quantitative variables. Normality assessment guided the presentation of variables, with parametric and non-parametric analyses (Chi-square test and paired t-test) applied. Statistical significance was set at α level of 0.05.
Results
This study provides a comprehensive analysis of demographic, psychosocial, and clinical factors influencing coping strategies, pain experiences, and diagnostic markers among 93 RA patients. The descriptive measures of demographic characteristics of study participants are summarized in Table 1.
Summary of Demographics.
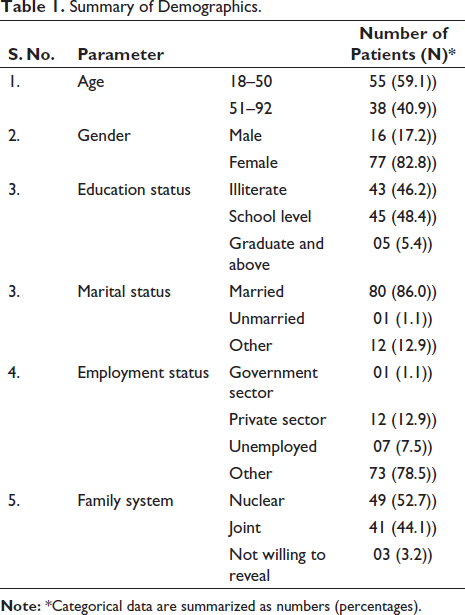
The bimodal age distribution, with a substantial representation of both younger and older individuals, implies the necessity of tailoring coping strategies to cater to age-specific needs, acknowledging potential variations in pain perception and management across different life stages. The predominance of females and the diverse educational backgrounds emphasize the importance of gender-sensitive and health literacy-focused interventions. Marital and employment status shed light on the broader socio-economic context that may influence coping mechanisms. Recognizing the significance of family systems underscores the need for holistic approaches that integrate familial support structures into coping strategies. These demographic insights, therefore, directly inform the development of targeted and inclusive coping interventions for managing pain intensity in patients with RA.
The Brief-COPE scores offer valuable insights into the coping strategies employed by study participants in response to stressful life events, particularly in the context of RA. The Brief-COPE summary scores of study participants are shown in Table 2.
BRIEF-COPE Summary Scores of Study Participants.
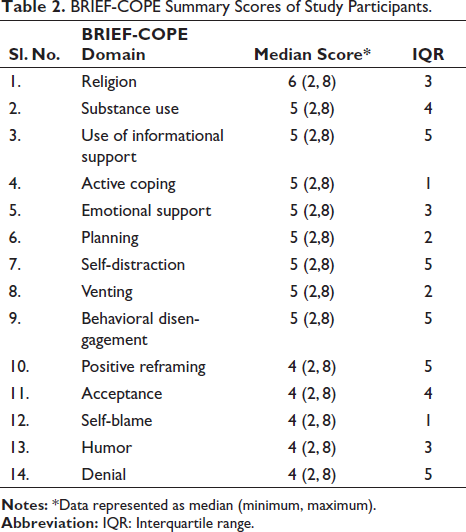
The median scores across various domains demonstrate a general tendency toward adaptive coping strategies. Religious coping emerges prominently with a median score of 6, indicating that participants frequently draw upon their religious beliefs to navigate stress. Substance use, often considered a maladaptive coping mechanism, also shows a median score of 5, suggesting a presence but not necessarily a predominant reliance on this strategy. The utilization of informational support, active coping, emotional support, planning, and positive reframing all exhibit median scores of 5, underscoring a balanced utilization of coping resources. It is noteworthy that the IQR scores provide additional depth to the understanding of coping strategy variability within the population. For instance, domains such as self-distraction, venting, behavioral disengagement, and denial, which exhibit higher median scores, also have IQR scores of 5, indicating substantial variability in the spread of scores within these domains. Conversely, active coping and self-blame, despite having median scores of 5 and 4, respectively, have lower IQR scores (1 and 1), suggesting greater consistency in participant responses within these domains. These findings contribute to a nuanced understanding of coping dynamics among RA patients, potentially guiding the development of targeted interventions that capitalize on adaptive coping strategies while addressing challenges associated with maladaptive ones. The frequency of anxiety and depression among study participants is shown in Figure 1.
Frequency of Anxiety and Depression among Study Participants.
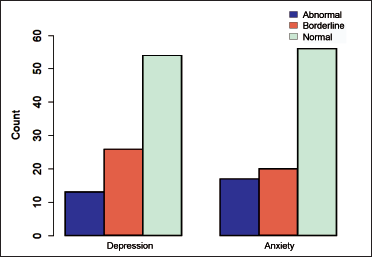
Among 93 RA patients, 14.0% experienced depression, and 18.3% faced anxiety. Patients with abnormal depression and anxiety predominantly employed coping strategies like religion, substance use, informational support, active coping, and emotional support. This shared pattern underscores commonalities in psychological experiences, suggesting the potential for integrated interventions. However, the reliance on coping mechanisms like substance use warrants careful consideration for overall health outcomes. These findings emphasize the need for tailored interventions recognizing the mental health challenges faced by RA patients and the potential interplay with coping strategies.
The responses to the Mankoski Pain Scale reveal a heterogeneous spectrum of pain experiences within the study cohort. Mankoski Pain Scale Ratings by study participants are shown in Table 3.
Mankoski Pain Scale Ratings by Study Participants.
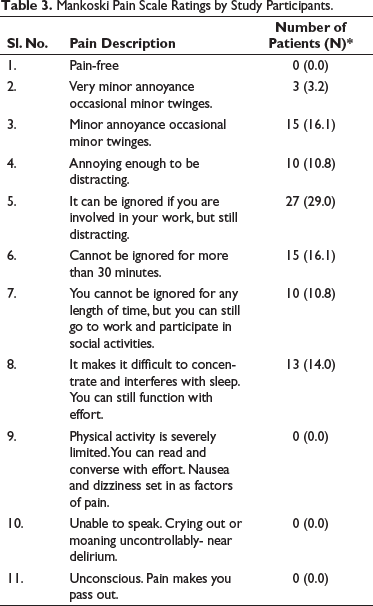
The majority of participants reported pain levels ranging from very minor annoyances to distractions that could still be managed with effort. Interestingly, a substantial proportion noted that the pain could be ignored when deeply engaged in work but remained distracting. Notably, the absence of participants in the extreme categories suggests that severe limitations to physical activity, unconsciousness, or near delirium were not reported within this cohort. This indicates a level of resilience among individuals, as they were able to maintain functionality and consciousness despite varying pain intensities. The findings underscore the importance of personalized pain management approaches, considering the diverse pain thresholds and impacts on daily life reported by the study participants. Tailoring interventions based on individual pain experiences is crucial for optimizing patient care and enhancing the effectiveness of pain management strategies within this specific population. The distribution of diagnostic markers reveals valuable insights into the prevalence and severity of RA among the studied population. Frequency distributions of ACCP, Rheumatoid Factor (RF), and DAS-28 scores among study participants are shown in Figure 2.
Multi-panel Chart of Rheumatoid Arthritis Diagnostic Markers Distribution across Study Population.
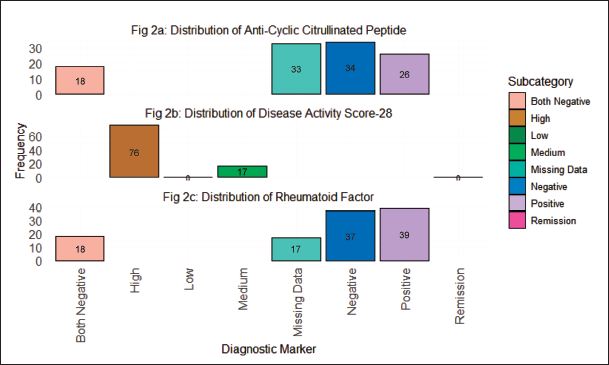
The Disease Activity Score-28 (DAS-28) categorization, spanning from High to Remission, signifies the spectrum of disease activity levels. The substantial frequency in the “High” category (76 cases) suggests a considerable proportion of patients experiencing elevated disease activity, warranting vigilant management strategies. The distribution in the RF subcategories, including both positive and negative cases, underlines the heterogeneity of the RA population and the varied immunological responses involved. Similarly, the frequencies in Anti-Cyclic Citrullinated Peptide (ACCP) categories provide insight into the autoimmune component of RA. The prevalence of missing data across parameters highlights potential challenges in complete diagnostic information, warranting attention in future studies. These numbers collectively underscore the nuanced clinical landscape of RA, emphasizing the need for tailored interventions and personalized coping strategies for patients across different disease activity levels and immunological profiles.
Discussion
Our study provides a comprehensive understanding of the demographic and psychosocial factors influencing coping strategies and pain experiences among RA patients, offering insights that align with and contribute to existing literature. The bimodal age distribution observed in our cohort, encompassing both younger and older individuals, resonates with previous studies emphasizing the diverse age groups affected by RA.13, 14 This demographic diversity underscores the need for age-tailored coping interventions, acknowledging potential variations in pain perception across different life stages. The predominance of females in our study aligns with the well-documented gender disparity in RA prevalence reported in the literature. 15 Moreover, the diverse educational backgrounds and insights into marital and employment status highlight the socio-economic context influencing coping mechanisms, a finding consistent with studies emphasizing the impact of socio-economic factors on RA outcomes.16, 17
The utilization of Brief-COPE scores to assess coping strategies among RA patients allows for a meaningful comparison with previous research. The predominance of adaptive coping strategies, such as religious coping, active coping, and positive reframing, aligns with studies that highlight the importance of these strategies in promoting psychological well-being among RA patients.18, 19 However, the variability in scores across domains, particularly in maladaptive coping strategies, reflects the complex and individualized nature of coping dynamics, supporting existing literature that emphasizes the need for personalized coping interventions tailored to individual preferences and challenges. 20 The higher median scores in domains like self-distraction, venting, behavioral disengagement, and denial, coupled with wider IQR, underscore the significant variability in the utilization of maladaptive strategies, aligning with studies that emphasize the diverse coping responses observed in RA populations. 21
The prevalence of depression and anxiety among our RA patients, 14.0% and 18.3%, respectively, is consistent with the documented mental health burden in this population.22, 23 The shared reliance on coping mechanisms such as religion, substance use, informational support, active coping, and emotional support among those with abnormal depression and anxiety aligns with literature emphasizing the interplay between mental health challenges and coping strategies among RA patients. 24 However, the use of substance as a coping strategy warrants careful consideration due to its potential impact on overall health outcomes, a concern echoed in studies emphasizing the need for holistic approaches to coping interventions. 25
The responses to the Mankoski Pain Scale in our study reveal a heterogeneous spectrum of pain experiences within the RA population, providing valuable insights into pain management. The majority of participants reported manageable pain levels, aligning with studies that emphasize the variability in pain experiences among RA patients.26, 27 The absence of participants in extreme pain categories suggests a level of resilience, as individuals maintained functionality and consciousness despite varying pain intensities. The spectrum of pain experiences observed underscores the importance of personalized pain management approaches, consistent with studies advocating for individualized care plans that consider diverse pain thresholds and impacts on daily life. 28
The distribution of diagnostic markers (DAS-28, RF, and ACCP) across our study population provides insights into the prevalence and severity of RA, contributing to the existing body of literature on RA management. The substantial frequency in the “High” DAS-28 category indicates a considerable proportion of patients experiencing elevated disease activity, consistent with studies emphasizing the impact of disease activity on RA outcomes. 29 The varied distribution in RF and ACCP subcategories underscores the heterogeneity of the RA population and the varied immunological responses involved, supporting existing literature on the diverse clinical presentations of RA. 30 The prevalence of missing data highlights potential challenges in obtaining complete diagnostic information, emphasizing the need for comprehensive data collection in future studies, a concern echoed in literature advocating for standardized and complete diagnostic assessments in RA research.
Conclusion
Our study contributes nuanced insights into the demographic, psychosocial, and clinical aspects of RA, aligning with and expanding upon existing literature. The findings underscore the need for personalized interventions that consider the diverse socio-demographic backgrounds of RA patients, emphasizing the importance of adaptive coping strategies and individualized pain management approaches. The prevalence of mental health challenges and the spectrum of pain experiences further emphasize the multidimensional nature of RA.
Abbreviations
Footnotes
Acknowledgments
The authors would like to thank Sree Vidyanikethan College of Pharmacy, Tirupati, Andhra Pradesh, India for supporting the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
An institutional ethical comity approval certification was taken to perform the current study (Roc.No.AS/11/IEC/SVIMS/2017).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed Consent has been collected from all th participants of the study.