
Abstract
Background
Studies indicated that smoking alters the response to anesthetics and alters the outcome of perioperative care. A full understanding of the impact of smoking cessation to enhance surgical outcomes is pertinent.
Purpose
This research aimed to compare perioperative cardiopulmonary complications in smokers and non-smokers during elective surgery under general anesthesia. We aimed to determine the incidence of complications in patients with a history of smoking, identify those at an increased risk, and assess the relationship between smoking duration and complications
Materials and Methods
A total of 100 patients, comprising 50 smokers and 50 non-smokers, were enrolled in the study. Various parameters, including heart rate increase during intubation, severe coughing, bronchospasm, oral secretions, oxygen desaturation, reintubation, opioid antagonist use, pulmonary edema, and other cardiopulmonary events, were assessed perioperatively. Statistical analysis involved both continuous and categorical variables. For continuous variables, the Student’s t-test and the Mann–Whitney U test were used for normally and non-normally distributed data, respectively. For categorical variables, chi-squared tests were employed. Sub-group analysis assessed the influence of smoking duration on the measured parameters.
Results
Smokers exhibited significantly higher incidences of severe coughing, heart rate elevation during intubation, and bronchospasm compared to non-smokers. Additionally, smokers experienced more pronounced oxygen desaturation throughout the perioperative period. Furthermore, a longer history of smoking was associated with an increased risk of complications, with individuals smoking for 10 or more years displaying a higher incidence of adverse events.
Conclusion
Smokers, particularly those with extended smoking histories, are at an increased risk of cardiopulmonary complications during elective surgery under general anesthesia. Emphasizing preoperative optimization, meticulous airway management, and smoking cessation support is essential to mitigate these risks. The study underscores the significance of these measures for enhancing perioperative safety and calls for further research to explore the long-term impacts and patient satisfaction associated with these interventions. These steps are essential not only for perioperative care but also for long-term health benefits among this patient population.
Keywords
Introduction
Tobacco smoking, an ancient practice, involves the inhalation of smoke containing active substances that enter the bloodstream through the lungs. 1 Nicotine, the primary component, binds to receptors in the brain, triggering dopamine release and reinforcing dependence. 2 Smoking is associated with a heightened risk of heart attacks, strokes, COPD, emphysema, and cancer. 3 Smokers also face increased perioperative complications, such as respiratory issues and infections. Consequently, quitting smoking before surgery is crucial to mitigate these risks.
Studies have shown that smokers who quit closer to surgery have a higher incidence of postoperative purulent sputum than non-smokers.4–6 Both active and passive smokers are more likely to experience adverse events during anesthesia induction. 7 Smokers exhibit elevated heart rates and neuroendocrine responses following tracheal intubation, indicating an increased risk of ischemic heart disease. 8 Furthermore, smokers have higher rates of respiratory complications, wound infections, and postoperative arterial oxygen desaturation.7–11 Current and former smokers also experience a greater incidence of pulmonary complications.10, 12 Intraoperative sputum volume is higher among smokers, and they are at an increased risk of respiratory complications. 13 Heavy smokers exhibit lower arterial oxygen tension during one-lung ventilation. 14 Smoking is linked to a heightened risk of perioperative respiratory complications, postoperative morbidity, and increased risk for passive non-smokers and passive ex-smokers. 15 These studies collectively highlight the adverse impact of smoking on perioperative outcomes, emphasizing the importance of smoking cessation before surgery to enhance overall surgical results.
Tobacco smoke, with its thousands of substances, significantly affects cardiovascular health and contributes to over 10% of global cardiovascular deaths. 16 Smokers face higher risks of coronary heart disease, cerebrovascular disease, and atherosclerotic cardiovascular disease.16–18 They also have an increased risk of myocardial infarction and higher all-cause and cardiovascular mortality, and are more prone to peripheral arterial disease and sudden cardiac death. 19 Smoking promotes atherosclerosis through mechanisms involving endothelial damage, inflammation, and metabolic abnormalities. 20 Additionally, smoking impairs lung function, leading to heightened infection susceptibility. 21 It causes lung cell damage, inflammation, and compromised immune function. Childhood smoking impairs lung function, while adult smokers experience accelerated decline. Although quitting smoking slows the age-related decline, complete restoration of lost lung function remains challenging. 16 Smoking cessation plays a pivotal role in ameliorating the adverse effects on both the cardiovascular and respiratory systems. 17
Considering the effects of general anesthesia on smokers is crucial. Smokers and those exposed to passive smoke require more anesthesia and painkillers during surgery, indicating an altered response to anesthesia.22, 23 General anesthesia in smokers leads to central respiratory depression, reduced lung compliance, atelectasis, decreased functional residual capacity, impaired oxygen exchange, increased ventilation–perfusion mismatch, and elevated alveolar–arterial oxygen difference. 24 Chronic smokers experience pronounced postoperative hypoxia, decreased pain tolerance, and higher analgesic requirements. 23 Monitoring oxygen saturation using pulse oximetry is essential, considering the effects of carbon monoxide on hemoglobin binding. Smokers may have changes in oxygen delivery and have erroneous pulse oximeter results. Smokers are also more likely to experience laryngospasm, bronchospasm, and coughing under anesthesia, requiring immediate treatment and management.25–27 Understanding the effects of anesthesia on respiratory function as well as the effects of smoking on oxygenation is critical for delivering the best perioperative care. 28
In summary, stopping smoking is an important step in reducing the risk of cardiovascular diseases, COPD, and cancer. 28 It will bring significant health benefits regardless of age or smoking history and reduce financial burdens while protecting others from secondhand smoke. It plays an important role in ameliorating the adverse effects of smoking on both the cardiovascular and respiratory systems. As smoking alters the response to anesthetics and alters the outcome of perioperative care, healthcare professionals need to have a comprehensive understanding of the impact of cigarette smoking and the importance of smoking cessation to enhance surgical outcomes.
Aim and Objectives
This research aimed to compare perioperative cardiopulmonary complications in smokers and non-smokers during elective surgery under general anesthesia. We aimed to determine the incidence of complications in patients with a history of smoking, identify those at an increased risk, and assess the relationship between smoking duration and complications. By examining these aims, we can provide valuable insights into smoking’s impact on perioperative outcomes and help identify patients who may need additional care and interventions to mitigate complications.
Materials and Methods
Study Design and Setting
This study adopts a prospective cohort design to investigate perioperative cardiopulmonary complications in smokers and non-smokers undergoing elective surgery under general anesthesia, which was the main objective of this prospective comparative study. The study was carried out at Yashoda Hospital, a private general hospital located in Malakpet, Hyderabad, India. This hospital setting serves a diverse patient population and offers a range of surgical services, making it suitable for our investigation.
Study Population
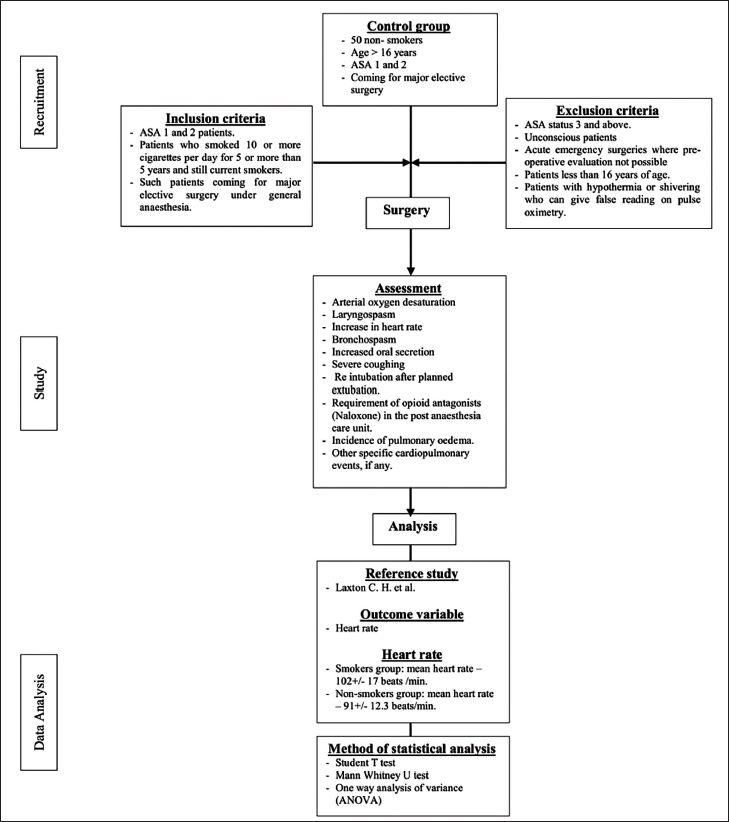
The study included a total of 100 patients who met the inclusion criteria. 50 consecutive smokers and 50 non-smokers were enrolled. The inclusion criteria comprised patients classified as American Society of Anesthesiologists (ASA) 1 and 2, individuals who smoked 10 or more cigarettes per day for at least five years, and patients scheduled for major elective surgery under general anesthesia. The term “smokers” refers to individuals who were actively smoking at the time of enrollment. Conversely, “non-smokers” include individuals who have never smoked. The control group consisted of non-smokers who had a clear history of never smoking, were aged above 16 years, and were classified as ASA 1 and 2 physical status undergoing major elective surgery. The control group was selected based on the absence of a smoking history, and efforts were made to match them to the smoker group. However, there were baseline differences in age between the groups that were not fully balanced. Exclusion criteria included unconscious patients, patients less than 16 years of age, patients classified as ASA status 3 and above, patients with acute emergency surgeries where preoperative evaluation was not possible, and patients with hypothermia or shivering, which could yield false readings on pulse oximetry. To enhance comprehension of the methodology, we have crafted a flow chart outlining the process, as illustrated in Figure 1. This study followed the inclusion criteria established by the original study conducted by Morton in 1944. 29 Additionally, possible explanations for the hemodynamic response to laryngoscopy and tracheal intubation in smokers were considered, including (a) the effect of nicotine, which increases heart rate through sympathetic stimulation, and (b) chronic smoking–induced changes in the epithelium and mucosa of the respiratory tract, rendering them highly sensitive to these stimuli. 30 In the context of intubation, an increase in heart rate was specifically considered in smokers, as previous studies did not demonstrate a significant difference in blood pressure rise among smokers during intubation.
Study Workflow.
Ethical Clearance and Patient Consent
Ethical clearance was obtained from the institution with the registration number ECR/49/Inst/AP/2013, and informed consent was obtained from each patient prior to their participation in the study. We employed a prospective comparative study design to approach potential patients for this research, and a systematic and ethical approach was employed. Eligible individuals were identified through comprehensive screening by the authors, and informed consent was obtained, ensuring understanding of the study. Participants were unequivocally assured that their decision to participate, or not, in the study would in no way impact their medical care or clinical relationship with the healthcare institution. This assurance was a cornerstone of our ethical approach, preserving the integrity of the doctor–patient relationship. Sensitivity and confidentiality were maintained, respecting autonomy and privacy. Moreover, we established clear and open communication channels to facilitate ongoing dialogue and follow-up with participants. This included providing participants with the necessary information and support they may require throughout their involvement in the study. We are dedicated to upholding the principles of transparency, respect, and ethical integrity throughout this research.
Sample Size Method
The sample size for this research was determined using a standard formula, where n represents the needed sample size. Based on the reference study by Laxton et al. 31 and the outcome variable of the heart rate, the mean heart rates of the smoker and non-smoker groups were considered. The formula utilized the standard deviation (σ) of the outcome variable, desired power (Zβ), desired level of statistical significance (Zα/2), and effect size (difference in means).
The following is the calculation:
n = [2σ 2 (Zβ + Zα/2) 2 ]/(difference in means) 2
= [2 × (17) 2 × (0.84 + 1.96) 2 ]/(102 − 91) 2
= [2 × (17) 2 × (2.8) 2 ]/(11) 2
= [2 × (289) × (7.84)]/121
= 37.45
n = 38 (hence, the minimum number of samples needed is 38).
The minimum needed sample size was calculated as 38, but a sample of 50 participants was selected for each group to ensure an adequate representation. This sample size calculation was aimed at achieving sufficient statistical power to detect significant differences between the groups. In addition, the choice of heart rate as the primary outcome for sample size calculation was based on its potential to provide valuable insights into perioperative stress responses, which is one of the primary objectives of this research. The study followed the inclusion criteria and serves as a point of comparison to assess changes in clinical practice and outcomes over time set by the original study by Morton in 1944, 29 which included patients smoking more than 10 cigarettes per day. By adhering to this sample size methodology, we aimed to obtain reliable and meaningful results in the comparison of various parameters between smokers and non-smokers.
Preoperative Procedures
Prior to surgery, all patients underwent pre-anesthetic evaluations. Smokers received counseling regarding the harmful effects of smoking and the benefits of smoking cessation. Patients were admitted to the hospital 24 hours before surgery for the optimization of preexisting comorbid conditions. Smoking was prohibited for smokers after admission in accordance with hospital protocols. All patients observed an eight-hour fasting period before surgery and were pre-medicated with oral alprazolam 0.25 mg and ranitidine 150 mg. In the operating room, patients were connected to monitors for ECG, non-invasive blood pressure, and pulse oximetry. Baseline values for heart rate, blood pressure, and arterial oxygen saturation were recorded, and intravenous access was established. Pre-oxygenation with 100% oxygen was performed before anesthesia induction, and medications including injection of glycopyrrolate 0.2 mg I.V., ondansetron 4 mg I.V., and fentanyl (2 mcg/kg) were administered. General anesthesia was induced using 2 mg/kg propofol, and tracheal intubation was performed within 15 seconds. Patients with prolonged surgeries lasting more than three hours were excluded from the study.
Perioperative Monitoring and Data Collection
Throughout the perioperative period, a vigilant assessment of various study parameters was conducted, spanning from induction to post-anesthesia care unit discharge. These parameters encompassed several crucial factors. Arterial oxygen desaturation was closely monitored, identified by a pulse oximeter indicating an SpO2 value below 92% for more than a minute at any stage of anesthesia. Noteworthy laryngospasm was documented when audible stridor or persistent airway obstruction persisted despite the intervention of experienced anesthesiologists. The extent of heart rate increase during intubation was categorized into four grades: Grade 1, for an increase of over 10 beats per minute; Grade 2, for over 20 beats per minute; Grade 3, for over 30 beats per minute; and Grade 4, for over 40 beats per minute. The presence of bronchospasm was determined by identifying audible wheezing or unexplained elevation in airway pressure. Furthermore, oral secretions were classified according to severity: Grade 1, for wet secretions (cleared by one suction); Grade 2, for moderate secretions (two to three suctions); Grade 3, for copious secretions (more than three times); and Grade 4, for thick secretions. Instances of severe coughing were documented if there were more than two paroxysms or if coughing persisted for longer than five seconds. Reintubation subsequent to planned extubation was closely monitored, and the administration of opioid antagonists (naloxone) in the post-anesthesia care unit was recorded. Additionally, the incidence of pulmonary edema and any other specific cardiopulmonary events were diligently observed.
Statistical Analysis
Statistical analysis was conducted using Microsoft Excel and SPSS Statistics 27.0 (IBM SPSS Inc., Chicago, IL, USA). The reference study by Laxton et al. was primarily for guidance in designing our statistical approach and was not used directly for analysis. 31
Analysis of Continuous Variables
To assess the differences between smokers and non-smokers, continuous variables such as heart rate increase were analysed. For normally distributed data, the Student’s t-test was employed to determine statistical significance. For non-normally distributed data, the Mann–Whitney U test was utilized. The two-tailed p value threshold for statistical significance was set at less than .05.
Analysis of Categorical Variables
Categorical variables including the incidence of cough, increased secretions, oxygen desaturation, bronchospasm, and laryngospasm were examined for differences between the two groups. We employed chi-squared tests to determine statistical significance in these categorical outcomes. p Values were used to assess the significance of associations, and a two-tailed p value of less than .05 was considered statistically significant.
Subgroup Analysis
As a pre-planned subgroup analysis, we explored the influence of years of smoking on the measured parameters. This was conducted using appropriate statistical tests, with adjustments made for multiple comparisons where necessary. The rationale for this subgroup analysis was to investigate potential dose-response relationships and variations in outcomes among smokers with varying durations of smoking.
Primary and Secondary Outcomes
The primary outcome of this study was the change in heart rate during the perioperative period in both the smoker and non-smoker groups. This change will be assessed both within each group and as a between-group difference. The rationale for using heart rate as a primary outcome is that it can serve as an indicator of sympathetic nervous system activation, which is a key component in perioperative stress responses. This choice also aligns with the study’s objective to assess cardiopulmonary consequences. Patients with cardiac arrhythmia will be included in the study, and their data will be analysed separately to account for any potential impact on the results. The categorization of heart rate increase during intubation will be based on the following grades: Grade 1, for an increase of over 10 beats per minute; Grade 2, for over 20 beats per minute; Grade 3, for over 30 beats per minute; and Grade 4, for over 40 beats per minute. The study will account for concomitant drugs and their doses administered peri-intubation and aim to balance these factors across both the smoker and non-smoker groups.
Demographic Considerations in Perioperative Complications: Exploring the Impact of Age and ASA Status in Smokers and Non-smokers Undergoing General Anesthesia
In this study, we meticulously considered the influence of age and ASA physical status on perioperative outcomes in smokers and non-smokers undergoing general anesthesia. Only ASA I and II patients were included, ensuring a relatively homogenous study population with similar baseline health statuses. Comorbid conditions, if present, were pre-optimized before surgery to minimize their potential impact on outcomes. Although patients were well matched in terms of age, ASA status, and the type of surgery, our investigation acknowledged the potential impact of these demographic factors on the observed outcomes. Given the established association between age and physiological responses to stress, as well as the ASA grading reflecting overall health status, we included these variables in our analysis. The rationale behind this inclusion was to explore potential variations in perioperative complications based on age and ASA status, providing a more nuanced understanding of how these demographic factors might contribute to the observed differences in adverse cardio-pulmonary events between smokers and non-smokers. By comprehensively considering these factors, we aimed to enhance the robustness and applicability of our findings to diverse patient populations. The analysis revealed a statistically significant increase in perioperative events among smokers compared to non-smokers (p < .005), underscoring the importance of accounting for demographic factors in the assessment of smoking-related complications during surgery.
Methodology Flow Chart
Results
Table 1 presents data on the age distribution of smokers and non-smokers, which reveals that in the 25–35 age range, there were four smokers (8%) and 19 non-smokers (38%). The 35–45 age group consisted of 22 smokers (44%) and 13 non-smokers (26%). Within the 45–55 age range, there were 18 smokers (36%) and 11 non-smokers (22%). In the 55–65 age group, there were five smokers (10%) and five non-smokers (10%). Finally, in the >65 age category, there was one smoker (2%) and two non-smokers (4%). The mean age of smokers was approximately 42 years with a standard deviation of 7.8, while non-smokers had a mean age of approximately 39 years with a standard deviation of 10. In Table 1, we categorized patients into age groups for the purpose of comparing age distributions between smokers and non-smokers. The age groupings were chosen to provide a comprehensive overview of the distribution of patients across different age brackets and were based on clinically relevant considerations.
Age Distribution of Smokers and Non-smokers.
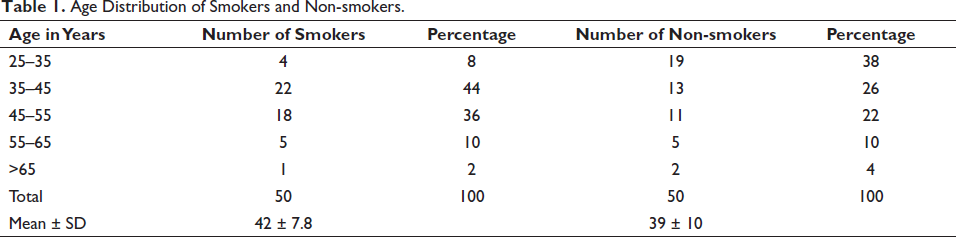
Overall, the age distribution between the two groups was found to be statistically different, with a p value of .023, indicating a significant variation in the age distribution between smokers and non-smokers, emphasizing the percentages within each category and presenting the mean age with standard deviation for both groups.
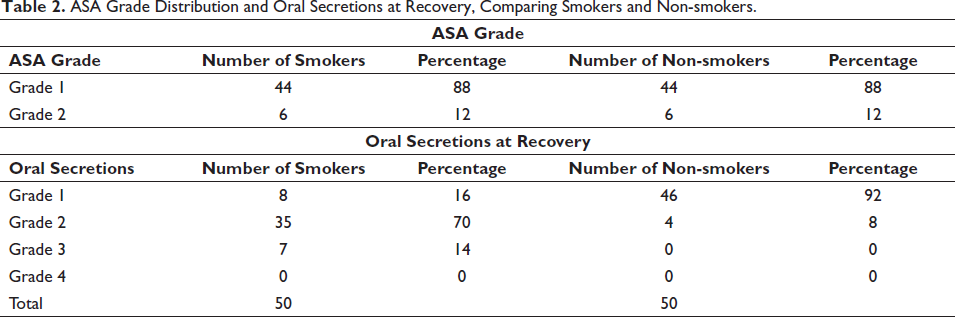
Table 2 provides information on the distribution of ASA grades among smokers and non-smokers. It is observed that both smokers and non-smokers exhibit a similar distribution. Grade I constituted the majority in both groups, representing normal healthy patients, with 88% of smokers and 88% of non-smokers falling into this category. Grade II indicates mild systemic disease is less prevalent, comprising 12% of both smokers and non-smokers. Importantly, Table 2 states that the ASA grading among smokers and non-smokers is matched, with a p value of 1, indicating no significant difference in the distribution of ASA grades between the two groups. Shifting focus to the oral secretions at recovery, it is evident that smokers have a higher prevalence of moderate to high-grade oral secretions compared to non-smokers. Grade 1 secretions, indicating minimal secretions requiring only a single suction, are reported in 16% of smokers but in a significantly higher percentage (92%) of non-smokers. In contrast, Grade 2 secretions, representing a moderate amount requiring additional suctioning, are observed in 70% of smokers and 8% of non-smokers. Additionally, Grade 3 secretions, indicating a high amount, are reported in 14% of smokers, while no non-smokers fall into this category. Grade 4 secretions are not observed in either group. These findings suggest that smokers tend to have a higher occurrence of moderate to high-grade oral secretions at recovery compared to non-smokers.
ASA Grade Distribution and Oral Secretions at Recovery, Comparing Smokers and Non-smokers.
In our study, the procedure distribution for smokers and non-smokers is shown in Table 3 along with the corresponding percentages. It shows that there are significant and comparable percentages of interventions for the upper abdomen, head, and neck in both categories. Our research shows that 12 smokers (24%) who undergo surgery also receive upper abdominal treatments, while 17 (34%) receive head and neck treatments. 12 non-smokers (24%) have upper abdomen operations, and 12 non-smokers (24%) have head and neck operations, both in a pattern similar to that of smokers. These figures suggest that there is a similar distribution of these operations between smokers and non-smokers. Table 3 also provides details on a number of additional procedures. No smokers (0%) and just 1 non-smoker (2%) in this category have undergone chest surgery. Three smokers (6%) and nine non-smokers (18%) have undergone upper extremity surgery. Four smokers (8%) and one non-smoker (2%) have undergone lower extremity procedures. 13 smokers (26%) and 12 non-smokers (24%) have had upper abdominal procedures. Finally, lower abdominal surgery was performed on 6 smokers (12%) and 9 non-smokers (18%). Seven smokers (14%), compared to six non-smokers (12%), have undergone spinal procedures. Last but not least, the information in Table 3 shows that procedures for the head, neck, and upper abdomen are more frequent and comparable in smokers and non-smokers. This shows that whether or not a person will undergo these procedures has little to do with whether or not they smoke. The proportion of procedures in other categories varies between smokers and non-smokers.
Distribution of Procedures Among Smokers and Non-smokers.
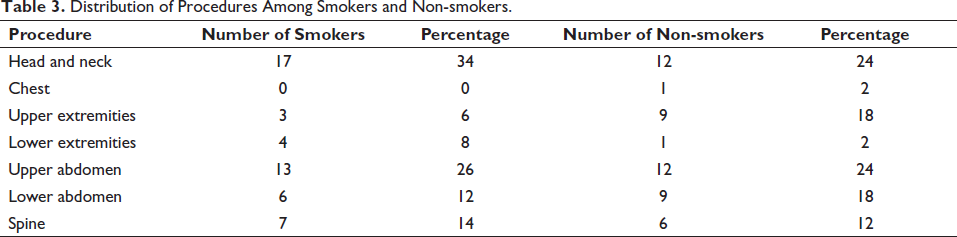
Table 4 shows that smokers have a higher incidence of perioperative adverse events compared to non-smokers. Among smokers, severe cough is reported in 30% of cases, while only 8% of non-smokers experience this event. Oxygen desaturation is observed in 14% of smokers compared to 4% of non-smokers, and bronchospasm occurs in 8% of smokers versus 4% of non-smokers. Laryngospasm is reported in 2% of smokers but is not observed among non-smokers. Table 4 also includes other adverse events, such as reintubation, naloxone usage in recovery, pulmonary edema, and others, which did not occur in either group. The table’s second section analyses the connection between smoking duration and perioperative adverse outcomes. While oxygen desaturation is reported in 3.57% of smokers who have smoked for 5–9 years, it escalates to 27% in those who have smoked for 10 or more years, indicating a significant difference. Bronchospasm and severe cough exhibit comparable patterns, with higher percentages among smokers who have smoked for 10 years or more. It is important to highlight that laryngospasm occurs in 4.5% of smokers who have smoked for 10 years or longer, but not in those who have smoked for 5–9 years. The p values reported show a statistically significant difference between the two groups for oxygen desaturation, bronchospasm, and severe cough. Overall, the data reveal a higher incidence of perioperative adverse events among smokers, particularly those who have smoked for 10 or more years. Adverse events such as severe cough, oxygen desaturation, and bronchospasm are more prevalent among long-term smokers compared to non-smokers and smokers with shorter smoking durations. These findings underscore the detrimental impact of smoking, especially prolonged smoking, on respiratory health and the increased risks associated with adverse events during the perioperative period.
Perioperative Adverse Events and Years of Smoking.
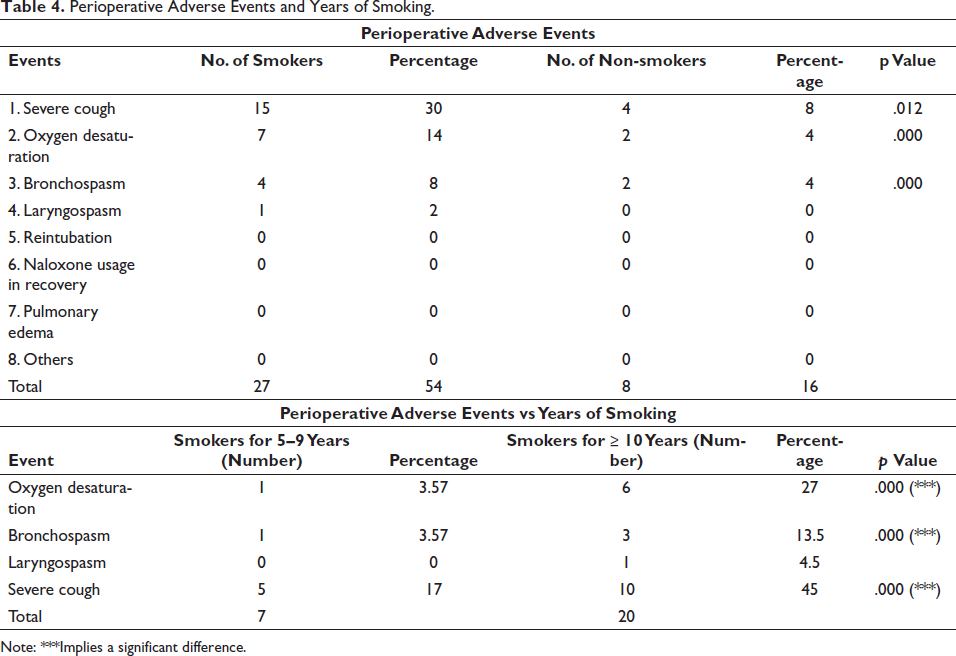
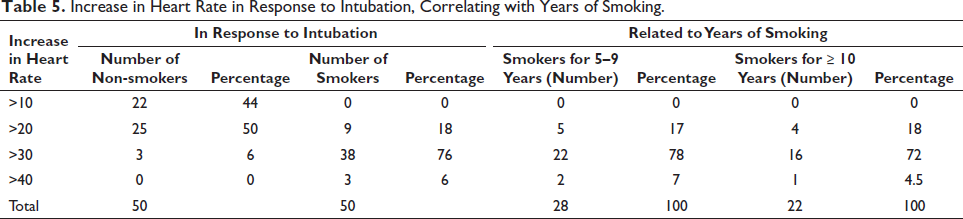
Table 5 presents that among non-smokers, 44% experience an increase in heart rate greater than 10 beats per minute (bpm) during intubation, while no smokers in the 5–9 years smoking group exhibit such an increase. Moving to an increase greater than 20 bpm, 50% of non-smokers and 18% of smokers experience this level of heart rate elevation. Among smokers who have smoked for 5–9 years, 17% experience an increase greater than 20 bpm, while among smokers who have smoked for 10 or more years, 18% have a similar increase. For a more pronounced increase, namely, greater than 30 bpm, only 6% of non-smokers experience this level of heart rate elevation, while a significant majority of smokers (76%) encounter it. Among smokers who have smoked for 5–9 years, 78% have an increase greater than 30 bpm, while among smokers who have smoked for 10 or more years, 72% experience this level of elevation. Furthermore, an increase greater than 40 bpm is not observed among non-smokers, but 6% of smokers encounter this significant heart rate elevation. Specifically, 7% of smokers who have smoked for 5–9 years and 4.5% of smokers who have smoked for 10 or more years exhibit this increase. In summary, the data indicates that smokers, particularly those who have smoked for 10 or more years, experience a more pronounced heart rate response to intubation compared to non-smokers. The percentage of smokers experiencing higher heart rate increases (>20 and >30 bpm) is significantly greater, highlighting the potential influence of smoking duration on physiological responses.
Increase in Heart Rate in Response to Intubation, Correlating with Years of Smoking.
Discussion
The purpose of this study was to compare perioperative cardiopulmonary consequences in smokers and non-smokers undergoing elective surgery under general anesthesia. Correlated to the demographic data, there was a considerable difference in the age distribution of the two groups, with smokers being more prevalent in the 35–45 age group than non-smokers, who were mostly in the 25–35 age group. However, the ASA grades of the two groups were comparable. This demonstrates that the demographics of the patients were well matched, allowing for a more precise comparison of the outcomes. These findings are consistent with prior research that found comparable age distributions and ASA grading between smokers and non-smokers. 32
In our study, we discovered that smokers’ heart rates increased substantially more than those of non-smokers. Most non-smokers experienced an increase in heart rate between 20 and 30 bpm, whereas most smokers experienced an increase greater than 30 bpm. These results, which are consistent with previous research indicating that smokers have a heightened sympathetic response to intubation, are likely due to the effects of nicotine and the respiratory system’s sensitivity.23, 30, 32 According to the greater heart rate response in smokers, which implies potential effects on individuals at risk for ischemic heart disease, smoking status must be considered when administering anesthesia. Hence, we can conclude that a rise in heart rate during intubation is an essential indicator of the body’s response.
Our analysis revealed that while patients were well matched in terms of age and ASA grade, these demographic factors may still play a role in influencing perioperative outcomes. Specifically, our examination of the procedure distribution between smokers and non-smokers (as detailed in Table 3) indicates notable patterns. The percentages of interventions for the upper abdomen, head, and neck were found to be significant and comparable in both categories. Notably, the information in Table 3 underscores that procedures for the head, neck, and upper abdomen are more frequent and comparable in both groups, indicating that the decision to undergo these specific procedures is largely independent of smoking status. These findings prompt further exploration into the intricate relationship between patient demographics and specific surgical interventions, contributing to a more nuanced understanding of perioperative complications in the context of smoking.
Additionally, chronic cough is one of the unfavorable surgical outcomes for smokers. According to our findings, smokers endure severe coughing at a far higher rate than non-smokers. Compared to a very small proportion of non-smokers, about one-third of smokers reported having a severe cough. Many studies that have found a correlation between smoking and an increased risk of postoperative respiratory difficulties, such as a persistent cough, back up these findings.10, 21, 33 The bronchial epithelium’s sensitivity and decreased ciliary function may contribute to the hyperactive cough reflex seen in chronic smokers. Anesthesiologists cannot emphasize enough how important it is to be aware of this increased sensitivity and take the necessary procedures to reduce postoperative cough in smokers.
One of our study’s fascinating findings was that smokers had worse oxygen desaturation throughout the perioperative period than non-smokers. This is consistent with previous research that revealed smokers are more likely to have oxygen deficiency.9, 10, 21 This greater prevalence might be explained by the negative consequences of long-term smoking on pulmonary function, such as decreased gas exchange and increased airway responsiveness. Smokers’ oxygen saturation levels should be continuously monitored by anesthetic experts at all times, especially during extubation and the first few hours after surgery. This will allow them to respond effectively and avoid any potential hypoxemia-related complications. The findings emphasize the importance of preoperative optimization and smoking cessation therapy in lowering the incidence of perioperative oxygen desaturation in smokers. Extended periods of smoking can significantly influence surgical outcomes through a multitude of physiological alterations. Prolonged exposure to tobacco smoke has been associated with systemic effects, as mentioned previously. Chronic smoking induces structural changes in the airways, leading to conditions such as chronic bronchitis and emphysema, which can escalate the vulnerability to perioperative respiratory challenges. Additionally, cumulative exposure to noxious substances in cigarette smoke can instigate inflammatory responses and oxidative stress, potentially exacerbating preexisting health conditions. Consequently, elucidating the intricate ways in which long-term smoking impacts these physiological processes is crucial for comprehending the heightened risks and complications that individuals with an extensive smoking history may face during surgery.
Bronchospasm is a serious perioperative complication that can lead to significant respiratory compromise. Consistent with our findings, our study revealed a higher incidence of bronchospasm among smokers compared to non-smokers. 27 Specifically, 8% of smokers experienced bronchospasm, whereas only 4% of non-smokers were affected. This statistically significant difference highlights the heightened risk of bronchospasm in smokers. Previous studies have also reported a similar association between smoking and increased bronchospasm risk.6, 27 The sensitization of bronchial epithelium and decreased ciliary function in chronic smokers, as discussed earlier, may contribute to the heightened airway reactivity observed in this group. Given the potential severity of bronchospasm, anesthesia providers must be vigilant in identifying and promptly managing this complication in smokers. Appropriate bronchodilatory interventions, such as beta-agonists and anticholinergic agents, should be employed to alleviate bronchospasm and optimize ventilation strategies.
Our study also investigated the relationship between the duration of smoking and perioperative cardiopulmonary complications. We found a significant association between longer smoking duration and increased risk of complications. Smokers who had smoked for 10 or more years showed a higher incidence of adverse events than those who had smoked for 5–9 years. For example, oxygen desaturation was observed in 27% of smokers with a smoking duration of 10 or more years, whereas it was present in only 3.57% of smokers with a shorter smoking duration. This significant difference underscores the cumulative effects of chronic smoking on the respiratory system. The longer individuals engage in smoking, the greater the risk of adverse events during the perioperative period. Consequently, clinicians should consider the duration of smoking as a crucial factor in assessing the preoperative risk profile of smokers and tailoring management strategies accordingly. Smoking cessation interventions and preoperative optimization of respiratory function should be strongly advocated to mitigate the risk of perioperative complications and enhance patient outcomes in this population. 12
Increased oral secretions during the perioperative period can pose challenges to airway management and increase the risk of aspiration. We observed that smokers had a higher incidence of increased oral secretions compared to non-smokers, with 70% of smokers requiring Grade 2 suctioning to clear the secretions. Moreover, there was a significant correlation between the duration of smoking and oral secretions. Smokers who had smoked for 10 or more years had a mean deviation of 2.09 in the oral secretions grading, compared to 1.89 in smokers who had smoked for 5–9 years. These findings suggest that chronic smoking may contribute to increased oral secretions, possibly due to changes in salivary gland function and increased mucus production, which correlate with the findings of a study done by Yamashita et al. Oral secretions in large quantities may impede airway control and increase the risk of respiratory complications during surgery. Hence, regular monitoring and proper suctioning procedures can help smokers, especially those with a longer smoking history, keep their airways clear and lower their risk of aspiration. The persistent increase in mucus production in individuals with a history of long-term smoking can be attributed to the complex interplay of various factors associated with tobacco smoke exposure. Chronic smoking triggers an inflammatory response in the respiratory epithelium, leading to hypersecretion of mucus-producing cells, notably goblet cells, in the airways. The components of cigarette smoke, including irritants and toxic substances, provoke ongoing irritation and damage to the respiratory mucosa. In response, the respiratory tract attempts to protect itself by producing an excess of mucus as a defense mechanism against these harmful agents. Over time, this chronic irritation and inflammation contribute to hypertrophy and hyperplasia of mucous glands, resulting in an increased baseline of mucus production. Consequently, individuals with a prolonged smoking history may exhibit heightened mucus levels in the mouth, potentially impacting their ability to control airways during surgical procedures.
Our study attempts to better comprehend the relationship between long-term smoking and the development of cardiopulmonary complications during surgery. Our research showed that the longer one smoked, the greater their risk of experiencing negative outcomes. Consistent with the findings of Movahed et al., 34 we found that long-term smokers (defined as those who have smoked for at least 10 years) had a higher incidence of complications than short-term smokers. Oxygen desaturation, bronchospasm, severe cough, and increased oral secretions were all significantly more common in long-term smokers (those who had smoked for 10 years or more). Bronchospasm, for example, was 13.5% more common in long-term smokers (those who had smoked for 10 years or more) than in short-term smokers (those who had smoked for 5–9 years) (p = .000). Similarly, 45% of long-term smokers reported to have a severe cough, compared to 17% of those who had smoked for 5–9 years (p .0001). These findings underscore the escalating nature of smoking-related health problems. Airway inflammation, impaired mucociliary clearance, and increased airway reactivity are just some of the long-term smoking effects that likely contribute to the observed differences. When evaluating the perioperative management of smokers, clinicians should be aware of the increased risks associated with prolonged smoking. Smoking cessation programs and preoperative respiratory therapy are two examples of strategies that aim to optimize respiratory function, potentially reduce these risks and improve patient outcomes.
In brief, our prospective study evaluates the perioperative cardiopulmonary complications between smokers and non-smokers who underwent elective surgery. Increased heart rate, severe cough, bronchospasm, and oxygen desaturation were all more common in smokers than in non-smokers, as was noted repeatedly by our study. Further, we discovered that longer periods of smoking were associated with a higher risk of complications, with those who had smoked for 10 or more years experiencing a higher incidence than those who had smoked for a shorter period. These results highlight the need for optimizing perioperative management strategies for smokers, which must take into account the patient’s smoking status and duration as part of the preoperative risk assessment. To reduce the likelihood of perioperative complications and improve patient outcomes, interventions aimed at helping smokers quit should be encouraged.
Limitations
Several considerations must be acknowledged when interpreting our findings. Initially, despite efforts to equate smoker and non-smoker groups, an age discrepancy surfaced, potentially introducing confounding variables that could impact the attribution of perioperative complications solely to smoking. Additionally, this study, conducted in a private general hospital in Malakpet, Hyderabad, India, though serving a diverse patient population, might not fully represent other healthcare settings, such as public or tertiary hospitals, thus potentially limiting the generalizability of our results. A pre-planned subgroup analysis based on years of smoking was performed, introducing potential multiple comparison issues that might affect result interpretation. Challenges in managing patient exclusions for surgeries exceeding three hours may have introduced selection bias, and the lack of specificity regarding the number of patients excluded could affect the study’s representativeness. In terms of data analysis, while one-way ANOVA was primarily employed for categorical variables, the appropriateness of this approach may be questioned. Furthermore, while chi-squared tests were conducted for categorical variables, this was not explicitly mentioned in the initial methodology, leading to ambiguity in our statistical methods. Although multiple statistical tests were conducted without explicit consideration for multiple comparison adjustments, increasing the likelihood of false positives, we believe our study, despite these limitations, provides valuable insights into perioperative complications related to smoking, offering guidance for future research and clinical practice in this critical area.
Conclusion
In our investigation of perioperative cardiopulmonary complications among smokers and non-smokers during elective surgery, we observed that smokers exhibited significantly higher risks of adverse events, including heightened heart rates during intubation, severe coughing, bronchospasm, and lower oxygen saturations post-extubation. Long-term smokers faced an even greater risk. To address these concerns, we recommend comprehensive preoperative optimization, the use of supplemental oxygen, and careful airway management. Emphasis on oral suctioning is crucial to tackle excessive secretions, especially in specific surgical scenarios. Minimizing airway instrumentation and promoting smoking cessation are vital measures to mitigate risks and improve overall patient outcomes. Our study underscores the importance of these actions for enhancing the safety and well-being of smokers undergoing surgery, calling for further research to explore long-term impacts and patient satisfaction with these interventions.
Recommendations
In light of the acknowledged limitations of this study, several recommendations can be made to enhance the validity and applicability of future research in this area. To address the age-related differences observed between smoker and non-smoker groups, future investigations should employ more rigorous matching techniques, such as propensity score matching, to ensure greater comparability of baseline characteristics. Additionally, expanding the research to include multiple healthcare settings, including public and tertiary hospitals, would help improve the generalizability of findings, considering that patient populations and healthcare practices may vary. Regarding subgroup analyses, pre-planned comparisons should be explicitly addressed in the study design to effectively handle potential multiple comparison issues. For exclusions based on surgical duration, investigators should report the exact number of excluded patients to provide transparency and account for the representativeness of the study sample. Addressing the statistical approaches, studies should ensure that the choice of statistical tests aligns with the nature of the variables examined, and researchers should explicitly state the methods used for each analysis. Finally, in consideration of the potential for multiple comparisons, studies should adopt strategies, such as Bonferroni corrections, to mitigate the risk of Type I errors. These recommendations aim to optimize future research endeavors in the field of perioperative cardiopulmonary complications and foster robust and comprehensive insights into the relationship between smoking and surgical outcomes.
Author Contributions
Conceptualization: VVR, DM, KWG; data curation: VVR, DM, SRK, VK; formal analysis: VVR, DM, SRK, WHC; investigation: VVR, DM, SRK, VK, WHC; methodology: VVR, DM, SRK, VK, MMK, SAA, KH; project administration: VVR, DM, SRK, VK; supervision: VVR, DM, SRK, VK; validation: VVR, DM, SRK, VK, WHC, KWG, LCM, MMK, SAA; visualization: WHC, KWG, LCM, MMK; writing—original draft: VVR, DM, SRK, VK; writing—review and editing: WHC, KWG, LCM, MMK, SAA, KH. All authors have read and agreed to the published version of the manuscript.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Research Ethics Committee (REC), Research Management Centre (RMC).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Sunway University Internal Grant Scheme (GRTIN-IGS(02)-DMS-12-2023).
Informed Consent
All of the study participants gave their informed consent.