
Abstract
Background
Colorectal cancer (CRC) is the third most common cancer worldwide causing approximately 10% of all cancer cases and is the second most frequent disease which is one of the leading causes of cancer-related fatalities. Traditional, complementary and alternative medicine (TCAM) refers to a broad range of health practices, therapies and products typically not part of the ‘conventional medicine’ system, and its use is substantial among the general population. The knowledge and awareness levels about TCAM and the use of allopathic medications for the treatment of cancer are varied among individuals. The studies were conducted on the knowledge and awareness of the public on cancer, however, no studies specifically addressing the knowledge, attitude and practice of TCAM about CRC were found in Malaysia.
Purpose
The present study aims to assess the knowledge of CRC and attitude towards TCAM in terms of CRC among a representative sample in Malaysia and identifying the sources of information about CRC and gauging the satisfaction levels with the services of a traditional medicine practitioner.
Materials and Methods
A validated self-administered questionnaire and educational brochure were utilized for this study. Convenience sampling was employed to recruit respondents (n = 548) from Kedah and Penang. The calculated sample size was 500. SPSS v25 was used to analyse the data.
Results
The demographic data were statistically significant (p < 0.05), the inference could be the sampling technique. Of the 548 respondents, 50.7% (n = 278) of them were CRC survivors. About 96.2% (n = 527) understood that CRC occurs in the colon or rectum. The majority were aware that rectal bleeding (75.4%) and blood in the stool (80.7%), are CRC’s signs and symptoms, while only 24.6% identified weakness and fatigue as CRC’s signs and symptoms. The respondents had poor knowledge scores (13.72 out of 31.00) as per Bloom’s cut-off scoring system. In terms of attitude towards TCAM, the majority had a ‘neutral’ (neither agree nor disagree) opinion for all the statements, meaning that the respondents surveyed were very undecided (neither positive nor negative opinion).
Conclusion
Knowledge of CRC was poor for the cohort, while the attitude towards TCAMs was neutral. The average ‘neutral’ response in the attitude domain could indicate that the respondents had minimal understanding of TCAM about CRC. Further, longitudinal studies can be conducted to better gauge the public’s knowledge, attitude and practice (KAP) towards CRC and TCAM. This highlights the importance of educational interventions which may help to improve the public’s KAP towards CRC and TCAM.
Keywords
Introduction
Colorectal cancer (CRC) is the third most common cancer worldwide causing approximately 10% of all cancer cases and is the second most frequent disease which is one of the leading causes of cancer-related fatalities. 1 CRC is the second most common cancer in Malaysia with 13.5% cases. 2 CRC was the most common cancer in men (54.1%) and second most common in women (45.9%) during the years 2007–2017 in Malaysia and the third most common cause of cancer deaths in Malaysia.3, 4 It is estimated that by the year 2035, the total number of deaths globally, from rectal and colon cancer will increase by 60% and 71.5%, respectively. 5 In 2018, the Malaysian study on cancer survival (MySCan) reported an observed five-year survival of 40.8% and a relative five-year survival of 51.1% for CRC. 6 CRC is considered a largely preventable cancer by various lifestyle modifications and regular health screening. 7 In Malaysia, there are various modalities of managing CRC which include surgery, radiation therapy, chemotherapy, immunotherapy, hormone therapy, and also includes traditional, complementary and alternative medicine (TCAM). 8
TCAM refers to a broad range of health practices (e.g., chiropractic, acupuncture), therapies (e.g., yoga, traditional Chinese medicine, Ayurvedic medicine, hypnotherapy, Siddha medicine) and products (e.g., herbal medicines, dietary supplements) typically not part of the ‘conventional medicine’ system, and its use is substantial among the general population.9, 10 TCAM has been used for centuries to treat numerous health conditions including non-communicable illnesses such as cancer. The use of TCAM is prevalent among various cancer patients worldwide, including Malaysia, ranging from 33.4% to 62%.11–14 In 2020, Razali et al. reported that the highest CAM users in Southern Peninsular Malaysia were breast cancer patients followed by gynaecology cancer and CRC patients. 14
There are numerous cancer treatments available worldwide such as chemotherapy, radiotherapy, immunotherapy, cryotherapy, surgical procedures and many more. 15 The choice of treatment depends on various factors including the type of cancer, cancer staging, patient’s age, symptoms and comorbidities.16, 17 For diseases like cancer, people have different treatment options which include TCAM. The knowledge and awareness levels about TCAM and the use of allopathic medications for the treatment of cancer are varied among individuals. Studies in knowledge and awareness of the public on cancer were addressed, however, none specifically addressing the knowledge, attitude and practice of TCAM about CRC were found in Malaysia. 18 The present study aimed to assess the knowledge of CRC and attitude towards TCAM in terms of CRC among residents of Kedah and Penang, apart from identifying the sources of information about CRC and gauging the satisfaction levels with the services of a traditional medicine practitioner.
Materials and Methods
This study was approved by the Medical Research Ethics Committee Ministry of Health, Malaysia (NMRR-20-3255-57235) and the AIMST University Human and Animal Ethics Committee (AUHEC/FOP/05/05/2021). The study was conducted by recruiting respondents from Kedah and Penang from March to August 2022. Two main groups were recruited namely CRC patients and non-cancer patients (general public). The CRC respondents were obtained from a public tertiary hospital, Hospital Pulau Pinang (HPP). The non-cancer cohort was recruited via an online survey using Google Forms. Raosoft® automated software programmes were used to calculate the sample size. The estimated sample size was calculated at a 95% confidence interval, 5% margin of error was 377. As this study sample was intended to serve as the baseline of a triphasic longitudinal educational intervention study, a 30% margin19, 20 for dropouts (n = 113) was allocated giving a final sample of 500 respondents. Convenience and purposive sampling were employed dividing the required number of samples into four categories namely CRC patients who use TCAM, CRC patients who do not use TCAM, the public who use TCAM and the general public who do not use TCAM. The general public here refers to individuals who are not diagnosed with CRC at the time of data collection. Adult (≥18 years old) Malaysian citizens from Kedah and Penang who were able to speak, read and understand English or Malay were included in the study.
Study Instruments
A self-administered questionnaire and an educational brochure were utilized for this study.
Questionnaire
A self-administered customized, adapted questionnaire was used as the data collection tool for this study. An informed consent form was attached to the questionnaire to inform the potential respondents about the study’s aim, assurance about the confidentiality of their information, and willingness to participate. The questionnaire was prepared through an extensive literature review with inputs and suggestions from a clinical oncologist.
The customized semi-structured questionnaire was prepared in English and Malay languages. The questionnaire comprised two domains: Section ‘A’ (knowledge regarding CRC) 6 items, and Section ‘B’ (attitude towards TCAM) 12 items. Question 6 of Section ‘A’ (sources of information regarding CRC) and question 12 of section ‘B’ (satisfaction levels towards services provided by traditional medicine practitioners) were not included in the main statistical analyses as they were subjective response-based items. The translation-retranslation process was done during the initial stages of validation by two Malay language teachers. The internal reliability test (Cronbach’s alpha) was performed for both the knowledge and attitude domains after completing the pilot study. The result of Cronbach’s alpha for the knowledge domain was 0.856 while the attitude domain scored 0.884. Since the values were greater than 0.70, indicating that the questionnaire was reliable and could be utilized for the main study. 21 The Automated Readability Index (ARI) was performed as well before recruiting respondents for the main study to gauge text understandability. 22 After the amendments, the ARI score of the questionnaire was 9.8, indicating that was even comprehensible by 14–15-year-old individuals. 22
Content validation was performed by a clinical oncologist and a general practitioner. It was followed by a readability test and face validation by 30 participants as part of the pilot study. The content of the questionnaire was then amended as per the reviewer’s and participants comments and suggestions.
Educational Brochure
The interventional educational tool is a customized brochure detailing the concepts and hazards of TCAM usage as well as relevant details on CRC. It was designed through an extensive literature review with inputs from experts in the field. This brochure was also prepared in both English and Malay languages and was validated (face, content, translation-retranslation). The validation process for this brochure consisted of three stages where the initial stage was performed by an oncologist and a general practitioner who reviewed the content. Next, the readability was assessed by respondents of the pilot study and lastly, the finalized version was prepared based on the suggestions obtained from the first two stages and redistributed to those individuals. The finalized version of the questionnaire and brochure were used for this present study.
Statistical Analysis
The data were coded and analysed using IBM® SPSS Statistics software version 25.0. Measures of frequency were used to summarise the socio-demographic data. The overall scores for the knowledge and attitude domains were calculated and the scores were categorised by using Bloom’s cut-off point (Tables 1 and 2). 23 A p value of <0.05 was considered statistically significant. Item 6 of Section A and Item 12 of Section B were analysed based on their frequencies.
Bloom’s Cut-off Score for Knowledge Regarding CRC (Section A).

Bloom’s Cut-off Score for Attitude Towards TCAM (Section B).

Results
Socio-demographic Data
Of the total 548 eligible respondents, 50.7% (n = 278) of them were CRC survivors while only 13.7% (n = 75) of them had a family history of CRC. The respondents were mainly female (57.1%), aged 18–25 years old (32.7%) and Malay (46%). Nearly all the respondents were either single (46.5%) or married (44.3%). About two-thirds of the respondents were from suburban areas (65.7%) and a majority had either completed their secondary (41.1%) or undergraduate (42.2%) education. A majority (29.7%) were employed while 10.9% of them have retired. Most of them had an income range of RM 1,500–RM 3,000 (Table 3). The demographic data were statistically significant (p < 0.05), the inference could be the sampling technique. All the aforementioned variables were deemed statistically significant (p < 0.05) as revealed by the Wilcoxon Signed Ranks test and Kruskal–Wallis test.
Socio-demographic Data of the Respondents (n = 548).
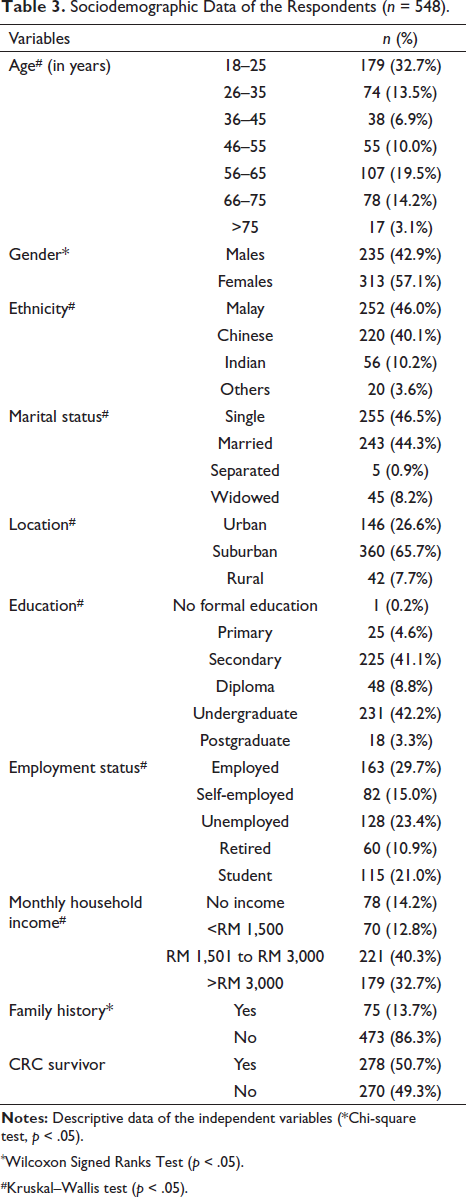
*Wilcoxon Signed Ranks Test (p < 0.05).
#Kruskal–Wallis test (p < 0.05).
Knowledge on CRC
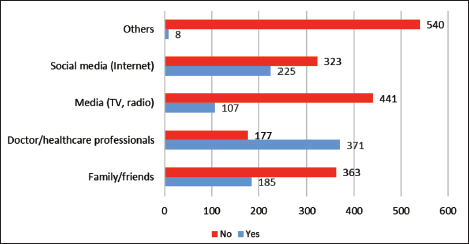
The knowledge scores were obtained by assigning a score of one (1) for the correct answer and zero (0) for the wrong answer. The respondents had poor knowledge scores (13.72 out of 31.00) as per Bloom’s cut-off scoring system (Table 1). Overall, 96.2% (n = 527) of the respondents understood that CRC occurs in the colon or rectum. The majority were aware that rectal bleeding (75.4%) and blood in stool (80.7%) are CRC’s signs and symptoms, while only 24.6% identified weakness and fatigue as CRC’s signs and symptoms. In terms of knowledge of the causes or risk factors of CRC, the top three selected options were family history of CRC (75%), older age (65.9%) and smoking (37%). Overall, 2% of the respondents (n = 11) identified TCAM as a risk factor for CRC as well. Very few respondents (6.8%) were aware of cryotherapy as a treatment option for CRC while surgery (85.9%) and chemotherapy (74.3%) were the most known. Consuming plenty of fibre, fruits and vegetables (80.8%), practising moderate, regular exercise (64.4%), consuming good quality carbohydrates and reducing red/processed meats intake (55.8%) were identified as the most known methods that can be practised to prevent or reduce the risk of developing CRC (Table 4). Figure 1 shows that doctors and healthcare professionals (67.7%) were identified as the main source of information regarding CRC.
Respondents’ Knowledge Regarding CRC.
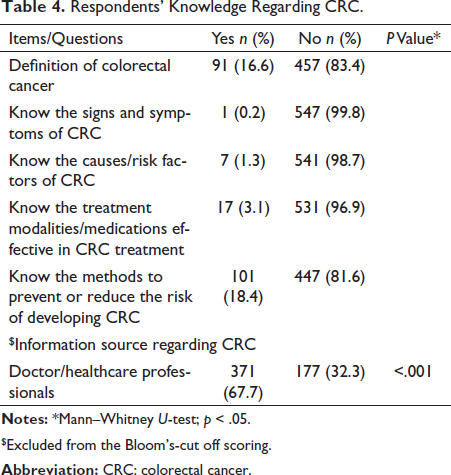
$Excluded from the Bloom’s-cut off scoring.
Frequency of Sources of Information Regarding CRC by the Respondents.
Attitude Towards TCAM
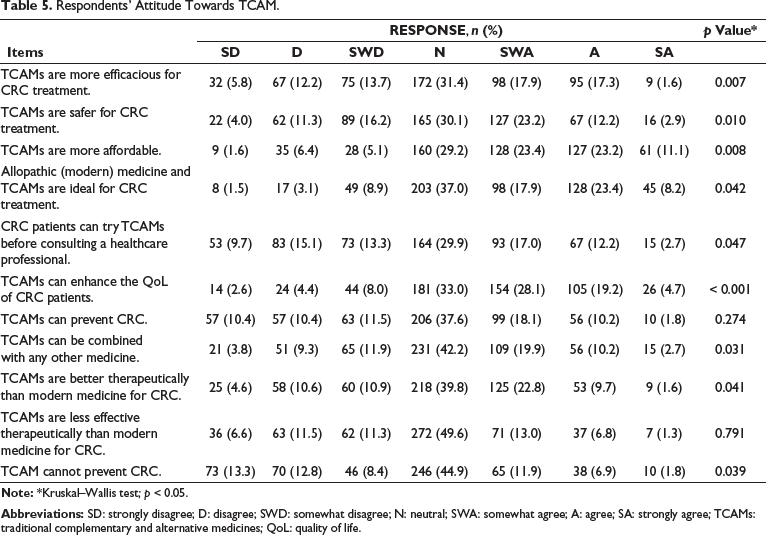
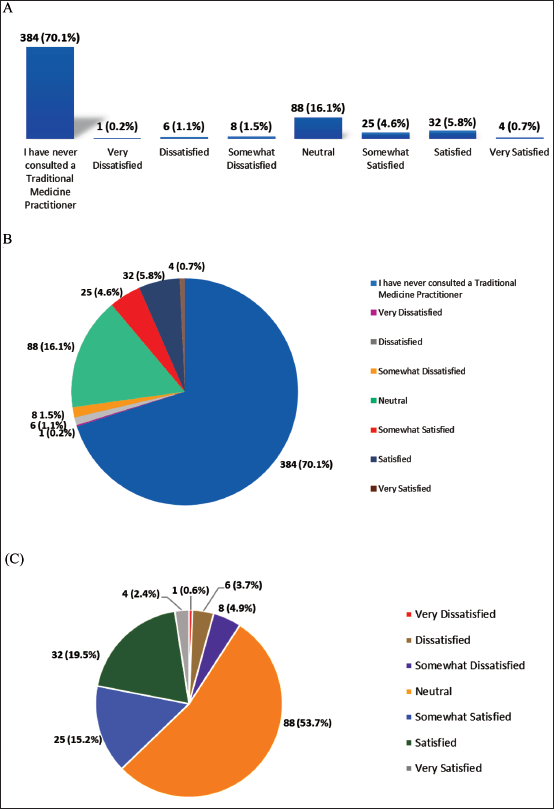
The respondents had an attitude score of 45.10 out of 77.00 as per Bloom’s cut-off scoring system. This indicated that they had a negative attitude towards TCAM in terms of CRC (Table 2). A majority had a ‘neutral’ (neither agree nor disagree) opinion for all 11 statements, indicating that the respondents surveyed were very undecided (Table 5). Only 164 (29.9%) of the respondents had consulted a Traditional Medicine Practitioner and a majority of them (n = 88, 16.1%) rated ‘neutral’ on their satisfaction level towards the services provided by Traditional Medicine Practitioners as depicted in Figure 2. Once again, this suggested that the respondents were undecided in terms of their attitudes towards TCAM usage.
Respondents’ Attitude Towards TCAM.
Discussion
Cancer treatment and care remain challenging, and, in such circumstances, many patients and their families turn to TCAM either as a standalone approach or in conjunction with standard treatments. The prevalence of TCAM can be attributed to several factors including treatment ineffectiveness, unmet patient needs, adverse effects, rising costs of conventional treatments, and the public’s perception that traditional and natural remedies are safer and more cost-effective. One of the major challenges with TCAM is the lack of supporting evidence on its therapeutic claim. 24
The current study evaluated the knowledge of CRC and attitude towards TCAM among Northern Malaysia residents where the respondents had poor knowledge of CRC and a negative attitude towards TCAM concerning CRC with Bloom’s cut-off scores of 8.0% and 51.67%, respectively. Mohd Suan et al. reported that the awareness of CRC in terms of cancer statistics, CRC symptoms and risk factors was found to be relatively good among Malaysians. 25 In another study among undergraduate Malaysian students reported that the majority of the respondents had a moderate level of knowledge and perceptions regarding CRC. 26
The present study revealed that the majority of the respondents were aware that CRC is a cancer that occurs in the colon or rectum and this finding was aligned with studies by Zainuddin et al. and Ramírez-Amill et al.26, 27 Majority of the present study participants were aware about the symptoms of CRC such as rectal bleeding (75.4%), and blood in stool (80.7%). Among Asians, knowledge of CRC was found to 40.6% (n = 909) participants identified bloody stool as a warning sign for CRC. 28
The present study findings highlighted that the majority of the respondents were not well aware of other CRC risk factors such as high-fat diets, history of ulcerative colitis or Crohn’s disease and radiation. The occurrence of CRC is associated with nonmodifiable risk factors such as age and hereditary factors and modifiable factors including environment and lifestyle. Lewandowska et al. reported that obesity, low physical activity, active and passive smoking and high salt and red meat consumption have been associated with an increased risk of CRC. 29 The present study also revealed that family history of CRC, older age, smoking and red meat consumption are the most common CRC risk factors.
Consuming fruits and vegetables, practising moderate, regular exercise, consuming good quality carbohydrates and reducing red/processed meats intake were identified as the most known methods that can be practised to prevent or reduce the risk of developing CRC. A Norwegian study identified that consumption of fruits, vegetables and wholegrain can decrease the risk of CRC. 30
Based on the knowledge of the present study respondents on the types of treatments or medications that they are aware of as CRC treatments, the majority knew of surgery (85.9%) and chemotherapy (74.3%) while only some of them identified cryotherapy (6.8%). Doctors and healthcare professionals were the dominant choice of source of CRC information for respondents in the present study. This finding aligns with findings from studies done in Hungary and Northeast Iran, where general practitioners and specialists (36.2%) and physicians (66%) were considered the most common source of CRC information.31, 32 However, a study in Poland and a study in Saudi Arabia reported the most frequently used source of knowledge of CRC was the Internet with 66.1% and 59.8%, respectively.33, 34 This was contrary to our finding whereby social media (Internet) ranked second with 41.1%.
Most of the respondents in the present study had a neutral attitude towards TCAM being more effective than modern medicine for CRC treatment (31.4%). The studies also reported that modern medicine is more effective than TCAM.35, 36 The effectiveness and safety of TCAM cannot be proven especially when the patients are on other conventional treatments for their comorbidities. It can be used to improve a patient’s quality of life, but it has to be under the supervision of a healthcare professional.37
Further longitudinal, multicentre studies employing a multi-modal educational interventional approach, a combination of health talks, educational brochures, and audiovisual aids can be conducted to better gauge and improve the public’s knowledge, attitude and practice (KAP) towards CRC and TCAM. Results of the present study highlights the importance of educational interventions such as health campaigns or awareness programs which may help to improve the public’s knowledge and attitude towards CRC and TCAM, consequently may influence their practice in this context.
Limitations
On account of financial and time constraints, the present study solely focused on respondents from two Northern states of Malaysia. The study site was a single medical facility (HPP), and the majority of the respondents were from two of the three ethnic groups: Malay and Chinese. A combination of these factors limits the generalizability of the study results. The sampling techniques (convenience and purposive sampling) also limited the chances of recruiting a larger study sample. Furthermore, as with all self-administered questionnaire-based studies, this study is subjected to response bias as we were unable to ensure that the respondents completed the questionnaire without any assistance.
Conclusion
This study indicated that knowledge of CRC was poor for the cohort, while the attitude towards TCAMs was neutral. The average ‘neutral’ response in the attitude domain could indicate that the respondents had minimal understanding of TCAM concerning CRC. Hence, our study demonstrated that the respondents had an inadequate understanding of both CRC and TCAM which may be altered by educational interventions via reliable resources
Abbreviations
Footnotes
Acknowledgments
We would like to thank all the respondents who have participated in this study. We also acknowledge the experts who guided us with the study instrument development and those who helped to share the survey e-poster.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This study was approved by the Medical Research Ethics Committee Ministry of Health, Malaysia (NMRR-20-3255-57235) and the AIMST University Human and Animal Ethics Committee (AUHEC/FOP/05/05/2021).
Funding
The publication of this article was funded by AIMST University (Malaysia).
Informed Consent
An informed consent has been obtained from the participant for this study.