
Abstract
Warfarin is the most commonly prescribed anti-coagulant medication. Warfarin’s pharmacokinetics (PK) in its enantiomeric form have been reported to be highly variable. Five population pharmacokinetic model studies for warfarin were identified in this systematic review. This review summarized these studies and reported on various factors affecting warfarin PK. Most studies reported a one-compartment model with first-order absorption and elimination for both S-warfarin and R-warfarin. Warfarin disposition has been reported to be influenced by various factors, including gender, age, genetic variation, body surface area (BSA), concurrent drug, weight, and ethnicity. So, all of these factors must be considered when addressing this pharmacokinetic variability. These models should undergo an external evaluation to confirm their generalizability and to support model-informed dosing in clinical settings.
Introduction
Warfarin is the most commonly used oral anti-coagulant for treating thromboembolic conditions in patients with atrial fibrillation, coronary artery disease, venous thromboembolism, and prosthetic heart valves.1, 2 Warfarin is a racemic mixture of two enantiomers, R and S. S-warfarin has a fivefold higher potency than R-warfarin.3–5 Warfarin works by decreasing the concentration of Vitamin K, which is needed for activating clotting factors. The international normalized ratio (INR) is used to assess the effectiveness of warfarin.6, 7
Warfarin anticoagulation therapy aims to maintain the target INR by using the lowest effective dose of the drug. 8 Warfarin is immediately absorbed from the gastrointestinal tract (GI) and has good bioavailability. The time to reach maximum drug concentration occurs 90 min after oral administration. R-warfarin and S-warfarin have half-lives of 35–58 h and 24–33 h, respectively. They have a high affinity for plasma proteins. These two isomers of warfarin have different pathways for metabolic transformation in the liver. 9
Warfarin is a narrow therapeutic index drug with high interindividual variability (IIV) in the daily dose requirement. 10 This IIV is explained by multiple factors like CYP2C9 and CYP2C19 polymorphisms, dietary vitamin K intake, concurrent medications, and anthropometric factors like age, weight, and body surface area (BSA). 11 Patients differ by 10–50 times in the doses needed to reach and maintain the INR goal .12, 13 The polymorphism in CYP2C9*3 and age were linked to decreased warfarin clearance, which led to smaller dose needs (i.e., enhanced sensitivity to the drug). 11 Patients with CYP2C9 wild-type enzymes have been found to have a greater incidence of bleeding complications.14, 15 According to reports, warfarin toxicity accounts for 10% of all adverse drug reactions resulting in hospitalization. 16
Population pharmacokinetics (PopPK) aims to characterize the observed IIV in drug exposure for a distinctive population sample. The method calculates the population mean (θ) and IIV (ƞ) of pharmacokinetics (PK) parameters, as well as the remaining residual, or unexplained, variability (ε). Covariates identified using the PopPK approach, such as demographics, pathophysiological variables, and genetic polymorphism, can aid in addressing drug PK variability. 17
The objective of this study is to summarize and explore the factors affecting the PK of warfarin from previous PopPK articles.
Methodology
Literature Search
The review was carried out in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines. The review included studies from their inception until November 25, 2022. The search keywords used in the databases were “Warfarin” AND “Population Pharmacokinetics” OR “PopPK” OR “Nonlinear mixed effects modeling” OR “NONMEM.” Supplementary Table S1 illustrates the search methodology applied across the various databases. Microsoft Excel was used to screen the articles for duplicates, identify the articles for review, and extract data.
Study Selection Criteria
Two reviewers (SM and GNKG) conducted an independent systematic search to identify relevant literature. The reviewers utilized the predefined inclusion and exclusion criteria to evaluate the titles, abstracts, and full texts of the publications. A third reviewer (AKP) was consulted if a disagreement was found during the review and search in order to resolve it. The studies that met the following criteria were taken into consideration for the review: (1) the PopPK model using a nonlinear mixed-effects modeling approach; (2) the parametric approach; and (3) a warfarin PopPK model development for the adult population. The studies were excluded if (1) the study drug was not warfarin and (2) editorials, letters, reviews, conference abstracts, book chapters, books, and short communications were not included.
Data Extraction
The authors used a standardized extraction method to extract the data from the whole texts of the chosen papers, and they then cross-checked it. The following information was extracted for each of the articles that were chosen: the publication year, first author, sample size of the study, number and type of samples collected for warfarin modeling, gender, body weight, age, ethnicity, CYP2C9, CYP2C19, and VKORC1 genotypes, structural model, residual variability, PopPK software, PopPK estimates, bioanalytical method, external validation, and variables that significantly affect the PK parameters. The extracted data was evaluated by the fourth author. A PRISMA flowchart was produced using Microsoft Word.
Results
Literature Search
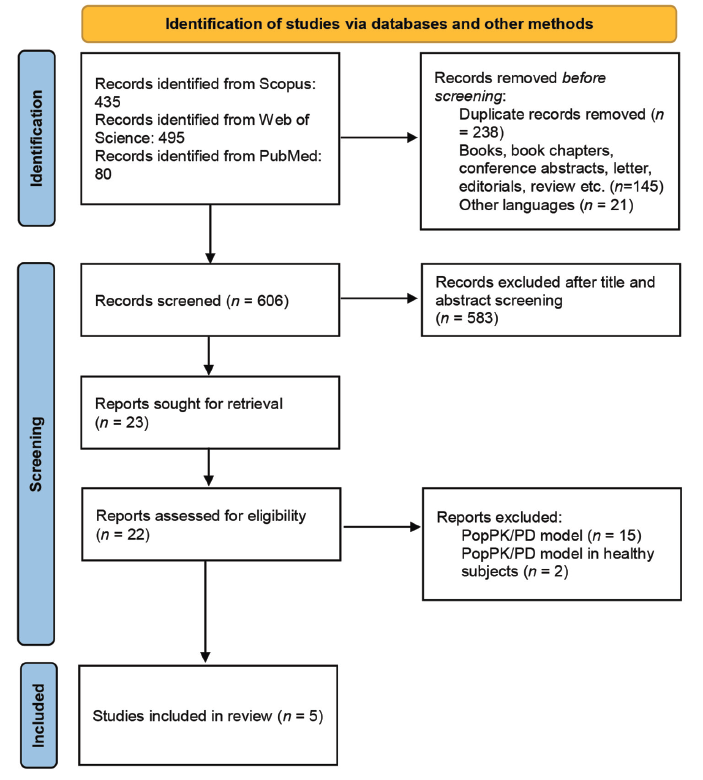
A total of 1010 articles were retrieved from databases. Of the 1010 articles, 80, 435, and 495 were from PubMed, Scopus, and Web of Science, respectively. Two hundred and thirty-eight duplicate articles overall were eliminated. After title and abstract review, 583 articles were eliminated, leaving only 23 for full-text screening. Based on the selection criteria, only five articles were chosen for the review. Out of 23 articles, one could not be retrieved, and 17 were excluded for the following reasons: (1) the population pharmacodynamic (PopPD) model (n = 15) and (2) the PopPK/PD model in healthy subjects (n = 2). The systematic review was left with five articles. The method for selecting PopPK warfarin studies for a systematic review is shown in the PRISMA flow diagram in Figure 1.
Study Population and Sample Size
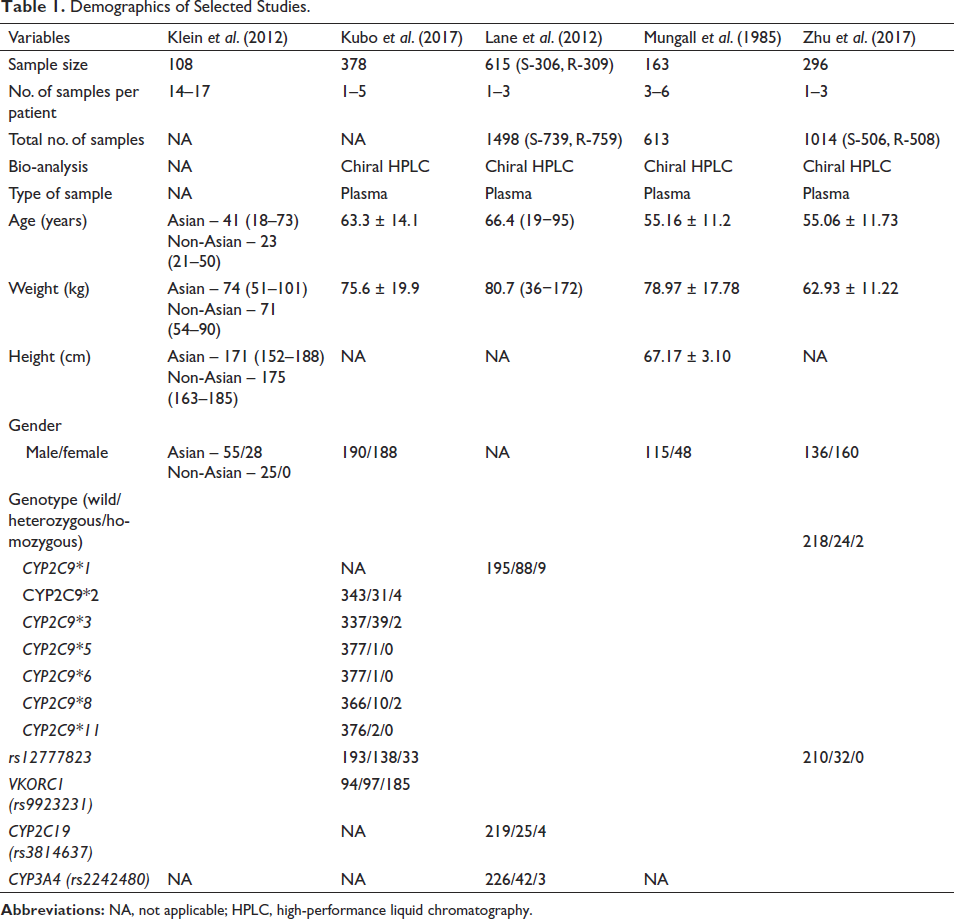
Out of five studies, Klein et al. pooled data from eight drug–drug interaction (DDI) clinical trials conducted on Asian and non-Asian populations. Asians, Italians, Americans, and African Americans represented the population of Kubo et al.’s study. Lane et al., Mungall et al., and Zhu et al.’s studies were conducted on the European, North American, and Chinese populations, respectively. The range of the population sample size was from 108 to 615, as shown in Table 1.
Demographics of Selected Studies.
Sample Collection Procedure
In some studies, patients only provided a few samples, whereas in others, patients provided five or more samples on the same or different days. During the sampling, blood was drawn at random and/or predetermined intervals. In a study by Klein et al., 17 samples were collected at 0, 0.5, 1, 2, 4, 6, 10, 12, 16, 24, 36, 48, 60, 72, 96, 120, and 144 h following the administration of warfarin. Kubo et al. collected at least five samples from the Asian population during the first month after starting warfarin, but in African Americans and whites, the blood sample was collected 11–19 h after the last warfarin dose during the maintenance phase. Lane et al. collected blood samples during the start of warfarin therapy, followed by 1, 8, and 26 weeks of therapy. The sampling time periods in the PopPK studies by Mungall et al. and Zhu et al. were 0–8, 8–12, 12–26, and 24–264 h after the start of warfarin dosing, respectively. Table 1 illustrates that the number of samples per patient and study ranged from 1 to 17 and 613 to 1498.
Bioanalytical Methods
Most studies used chiral high-performance liquid chromatography (HPLC) to measure the plasma concentrations of S-warfarin or S-warfarin and R-warfarin.19–22 Klein et al. 23 did not mention any bioanalysis method or sample type used to estimate warfarin concentration.
Population Pharmacokinetics Modeling
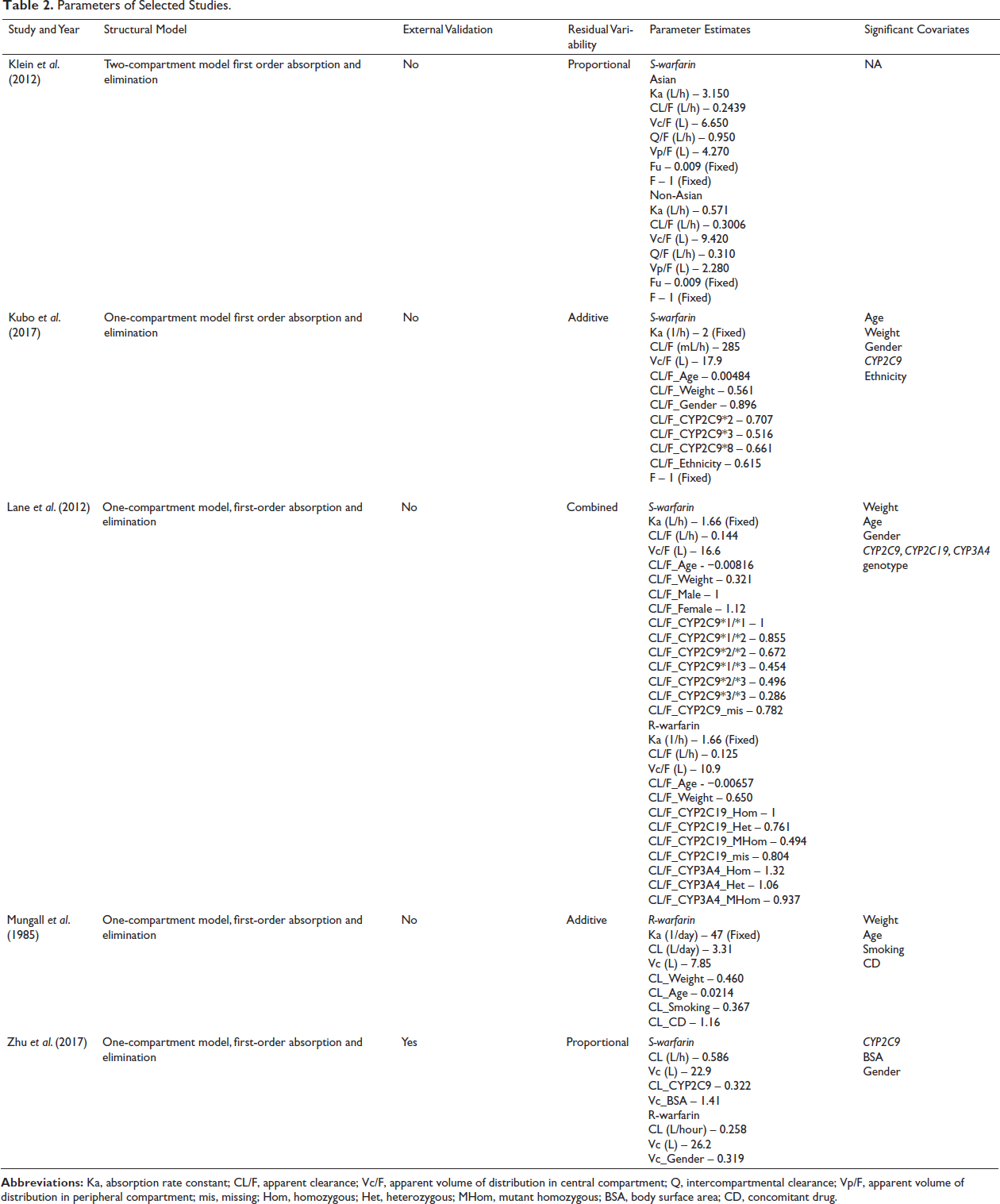
All the studies utilized NONMEM for PopPK modeling. In four PopPK studies, a one-compartment model of first-order absorption and elimination was used to explain the structural model for S-warfarin. On the other hand, the study by Klein et al. 23 developed two distinct models for the Asian and non-Asian populations using a two-compartment model of first-order absorption and elimination. Lane et al. 20 and Zhu et al. 22 developed the PopPK model for both S-warfarin and R-warfarin. The absorption rate of S-warfarin ranged from 0.571 to 3.150 per hour. For S-warfarin and R-warfarin, the apparent clearance and apparent volume of distribution (Vd) in the central compartment are 0.13–0.586 L/h and 0.125–0.0258 L/h, respectively, and 6.65–22.9 L and 10.9–26.2 L, as illustrated in Table 2. In the selected studies, the residual error was explained by various models, including additive, proportional, and combined models.
Parameters of Selected Studies.
Influence of Various Genotypes on S-warfarin and R-warfarin Disposition
According to three studies, single-nucleotide polymorphisms (SNPs) in the CYP2C9 gene have significantly reduced S-warfarin clearance.19, 20, 22 It has been reported that the allelic variants of CYP2C9*2, CYP2C9*8, and CYP2C9*3 contributed to a 29%, 34%, and 48% reduction in S-warfarin clearance, respectively. 19 Another study found that having the CYP2C9*3/*3 genotype resulted in a 71% decrease in S-warfarin clearance. R-warfarin clearance is influenced by CYP2C19 and CYP3A4 genotypes. Patients with CYP2C19 heterozygote and variant homozygote reduced R-warfarin clearance by 24% and 51%, respectively. However, the R-warfarin clearance of patients with the CYP3A4 heterozygote genotype increased by 32%. 20
Influence of Anthropometric and other Factors on PK Parameters of S- and R-warfarin
S-warfarin clearance increased with body weight; it was 12% higher in men, and it decreased as age progressed. Except for gender, the same covariate relationship was found in the R-warfarin clearance. 20 R-warfarin clearance has been found to increase slightly in smokers. 21 According to Kubo et al., African American ethnicity and gender resulted in lower S-warfarin clearance rates of 39% and 10%, respectively. 19
External Validation
Zhu et al. only performed external validation on the PopPK model that they developed. The final model was used in this study to predict S- and R-warfarin concentrations for an evaluation dataset of 42 patients and compared them to the actual concentrations. The mean prediction error (MPE) and root mean square error (RMSE) were used to assess the precision and bias of this PopPK model. The MPE and RMSE were −0.20 and 0.24, respectively. According to the external validation, the model underestimated doses greater than 4 mg and overestimated doses less than 2 mg. 22
Simulation
In the study by Klein et al., the simulation was carried out by categorizing according to ethnicity to determine whether the model could be used to simulate accurate data. In addition, it was used to determine the bare minimum of participants and ideal PK sampling intervals required for a two-by-two cross-over warfarin DDI trial to achieve 80% power and a 5% type I error rate. 23 With various combinations of CYP2C9*1/*1 allelic variants and VKORC1 genotypes for three different populations, Kubo et al. carried out the simulation using the pharmacogenetic European Pharmacogenetics of Anti-Coagulant Therapy and International Warfarin Pharmacogenetics Consortium algorithms. The simulation demonstrated that, in all populations, the average steady-state concentration of S-warfarin in individuals with CYP2C9*1/*1 may vary depending on the VKORC1 genotype (the AA genotype required a lower dose than the GG genotype to maintain the therapeutic INR). 19
Discussion
To the best of our knowledge, this is the first review that provides an overview of the information describing the previously published PopPK model for warfarin. When starting warfarin for the first time, major bleeding incidents and thromboembolism are more common and present a difficult therapeutic phase. As a result, effective drug initiation protocols that anticipate and make adjustments for IIV have a significant potential to enhance warfarin anticoagulation therapy.24–27
Many studies show that CYP2C9*2,*3,*8, and CYP2C19 genotypes influence the PK of S-warfarin and R-warfarin metabolites, respectively. These parameters are affected by a variety of additional variables, such as age, gender, BSA, weight, renal function, ethnicity, smoking, and concurrent medications.19, 20, 22, 24
The IIV on apparent clearance of S-warfarin ranged from 16.9% to 41.8%, while R-warfarin ranged from 21% to 43%. The IIV on the apparent Vd for S-warfarin ranged from 35.8% to 53.2%, but it ranged from 21.6% to 44% for R-warfarin. Most studies did not estimate the absorption rate constant (Ka), so they fixed it using an intermediate value or published literature. However, only the study by Klein et al. 23 estimated the Ka, which was 3.15 (h−1) for the Asian population and 0.571 (h−1) for the non-Asian population.
S-warfarin and R-warfarin clearance increased with body weight and decreased with age. 19 This result was in accordance with the previously published studies.28–31 Kubo et al. found that every 10 years of age increase from 65.7 to 75.7 years resulted in a 5% decrease in S-warfarin clearance, and every 10 kg weight reduction from 73 to 63 kg resulted in an 8% decrease. Whites and Asians showed increased S-warfarin clearance in a similar pattern, which may be related to their heavier body weights. 20
Gender had an impact on the clearance of S-warfarin and R-warfarin,19–22with females having a 22% lower clearance than males and needing lower doses for equivalent anticoagulation potency and efficacy. 32 There is still some disagreement in this report about the role of gender in S-warfarin PK.33–35 Another study found that gender has an impact on the Vd of R-warfarin, with women having a 31.9% lower Vd than men. 22
The clearance of S-warfarin has been significantly impacted by ethnicity. In a study by Kubo et al. 19 it was discovered that African Americans had a 39% lower clearance of S-warfarin. It has been noted that concomitant drugs, like enzyme inducers, can alter S-warfarin clearance by altering hepatic metabolism.21, 36, 37
According to the Mungall et al. 21 study, smoking has an impact on warfarin clearance. This result is consistent with the findings of Natisuwan et al., which state that smoking increases warfarin clearance.38, 39 According to Zhu et al., 22 BSA had an impact on the Vd of S-warfarin, but Kirking et al. found no correlation between BSA and warfarin concentration 40 .
Several studies have found that simulation-based drug dosing for patients based on their characteristics increases effectiveness while decreasing toxicity when compared to traditional dosing.41–43 Model interpretation is aided by pharmacometric simulation. Predicting drug effects under various unobserved circumstances is an important additional function of simulation. When making a simulation-based decision, it is desirable to take into account interindividual variation, a true biological reality, as opposed to the more popular deterministic simulation, which is based only on predefined effect parameters and ignores random effects. 44
Limitations
In some studies, the PopPK model was developed using clinical data from other studies. As a result, there can be bias in the modeling data that is not evident in the selected articles. The review was limited to English-language studies and left out studies in other languages. The review describes the different PopPK models, but it does not account for how to use the model’s generalizability to make well-informed dosing decisions for these populations in clinical practice.
Future Directions
The generalizability of the published models in clinical settings can be evaluated using meta-analysis, a statistical technique that combines data from numerous PopPK/PD studies of the warfarin drug. This provides important insights into the drug’s PK and pharmacodynamics across a variety of patient populations.
Conclusion
According to this review, the CYP2C9 and CYP2C19 genotypes affect S- and R-warfarin PK, respectively. However, these parameters are affected by anthropometric traits and mutations in other genes encoding the enzymes for warfarin metabolism. The pharmacokinetic parameters of warfarin metabolites were explained by a one-compartment structural model in the majority of studies. External validation of all these models will lead to the identification of an integrated or generalizable model suitable for model-based, informed warfarin therapy.
Abbreviations
BSA: Body surface area; INR: International normalized ratio; Tmax: Time to reach maximum drug concentration; IIV: Interindividual variability; PopPK: Population pharmacokinetic; PK: Pharmacokinetics; PRISMA: Preferred reporting items for systematic review and meta-analyses; PopPD: Population pharmacodynamic; DDI: Drug-drug interactions; NONMEM: Non-linear mixed effects modeling; SNPs: Single nucleotide polymorphisms; MPE: Mean prediction error; RMSE: Root mean square error; EU-PACT: European pharmacogenetics of anti-coagulant therapy; IWPC: International warfarin pharmacogenetics consortium; KA: Absorption rate constant; Vd: Volume of distribution.
Authors’ Contributions
Conceptualization: S.M. and G.N.K.G.; Methodology: S.M. and G.N.K.G.; Data Curation: S.M., G.N.K.G., and A.K.P.; Formal Analysis: A.K.P. and S.D.R.; Writing—original draft: S.M. ; Writing—review and editing: J S.M., G.N.K.G., S.D.R. and A.K.P.; Supervision: G.N.K.G. All authors have read and agreed to the published version of the manuscript.
Supplementary Material
Supplemental material for this article is available online.
Supplemental Material for Various Factors Influencing the Enantiomers of Warfarin Pharmacokinetics: A Systematic Review of Population Pharmacokinetics by Sirajudeen Mahaboob, G.N.K. Ganesh, K.P. Arun and S.D. Rajendran, in Journal of Pharmacology and Pharmacotherapeutics