
Abstract
Objective
To determine intraoperative awareness and estimate the factors associated with intraoperative awareness.
Methods
An observational cross-sectional study was carried out after approval from the institutional ethical committee. The duration of the study is 2 months. After completion of the surgical procedure, anesthesia was reversed, and there was an adequate return of consciousness. The patients were interviewed about their surgery using the modified form of the Brice questionnaire. After the questionnaire was completed, it was analyzed, and patients were categorized into either having definite awareness, possible awareness, or no awareness.
Results
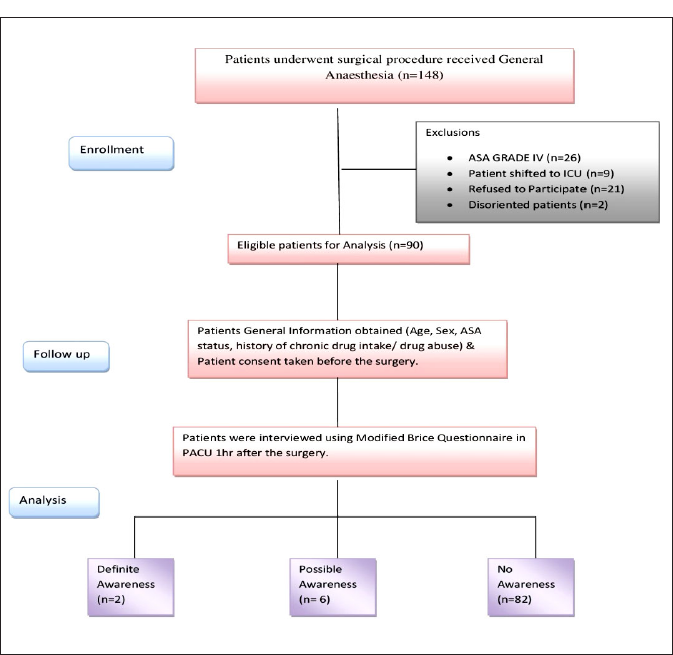
It was observed that out of 90 patients operated on under general anesthesia, eight reported having remembered something under general anesthesia. Out of eight patients, two were found to have definite awareness, and the occurrence of definite awareness was calculated to be 2.22%. Six patients were categorized under possible awareness, and the occurrence of possible awareness was estimated to be 6.6% in our study.
Conclusion
The occurrence of intraoperative awareness was estimated to be 8.8%, including definite and possible awareness under general anesthesia. Finally, we conclude that intraoperative awareness might be due to the inadequate depth of general anesthesia given to the patients. The dose of general anesthetic drugs was not maintained based on its minimum alveolar concentration (MAC).
Introduction
Intraoperative awareness is an unexpected memory of intraoperative events. 1 The types of intraoperative awareness are classified into explicit and implicit memories. Explicit memory is the intraoperative awareness that can be recalled spontaneously or may be provoked by postoperative events or questioning. In contrast, implicit memory is the memory that may be consciously recalled but might affect the person’s behavior later. 2
The causes of intraoperative awareness are not fully established and may be multifactorial. Patients younger in age group, smokers, drug addicts, or long-term use of drugs like opiates and alcohol consumption may increase the individual requirement for general anesthetic drugs. 3
It has been postulated that this patient-specific variability, like dose requirements, may be due to altered gene expression of target receptors. 4 Some preclinical studies have shown that long-term exposure to alcohol or persistent seizures has increased the expression of this memory-blocking receptor.5, 6 The genetic polymorphism of the gamma-aminobutyric acid (GABA) α receptor 5 gene is also an important factor in contributing to intraoperative awareness. 7
The anesthetic dosage that blocks intraoperative awareness is less than the dosage that prevents motor responses to pain.8, 9 The judgment of anesthesiologist about the adequate depth of anesthesia can also be imprecise in the patients. Various modalities have been tried to assess intraoperative awareness in anesthetized patients. These include monitoring blood pressure, heart rate, end-tidal anesthetic concentration, and the bispectral index (BIS). However, none of these modalities has been found to be 100% effective in detecting awareness under anesthesia. 10
The incidence of awareness in developed countries is found to be 0.1%–0.2%.11, 12 In developing countries, the incidence of intraoperative awareness is thought to be somewhat higher. Intraoperative awareness in the Indian population has never been studied. Therefore, we wanted to detect intraoperative awareness in patients who were at high risk of experiencing awareness during surgery in our population.
Materials and Methods
An observational, cross-sectional study was conducted in a tertiary care teaching hospital after getting approval from the institutional ethical committee (IEC No. 2020/607). The duration of the study is 2 months.
Sample size was calculated using the formula n = 4Pq / L² (+ 10% non-responder error) where P = 6% (prevalence)
13
, q = 100 – 6 = 94 L = precision error 5%.

Patients who have undergone any surgical procedure under general anesthesia between the ages of 18 and 60 years with physical status from American Society of Anesthesiologists (ASA) I to ASA III were included in the study. Patients who were not extubated after surgery and transferred to an intensive care unit or who were not mentally well were excluded from this study. Written informed consent was obtained from all patients in their language before including them in this study.
The technique and drugs used for anesthesia varied according to the patient’s preoperative condition, the surgical procedure planned, and the choice of the anesthesiologist. The induction agent used was either i.v. thiopentone sodium or i.v. propofol, followed by a muscle relaxant, which was either vecuronium or atracurium. After intubation, maintenance of anesthesia was done using 50% oxygen, 50% nitrous oxide, and volatile anesthetic (isoflurane or sevoflurane) agents. During the procedure and throughout the postoperative period, the vital signs (including heart rate, oxygen saturation, electrocardiography, and noninvasive blood pressure) of the patients were monitored, and the concentration of volatile anesthetic was adjusted according to the patient’s vital signs.
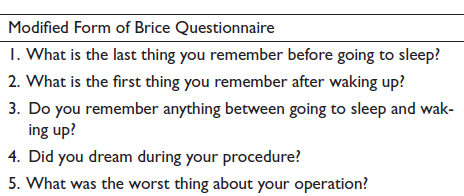
A consultant anesthesiologist who was unaware of the patients being included in this study anesthetized all patients. After the completion of the surgical procedure, anesthesia was reversed, extubated, and shifted to the post-anesthesia care unit (PACU) after the adequate return of consciousness. Approximately 1 h after arrival in PACU, patients were assessed for intraoperative awareness, and questions were asked in their own language. First, general information such as age, sex, ASA status, anesthesia technique used, history of chronic drug intake or substance abuse, and any previous history of awareness were obtained. Then, the patients were interviewed about their surgery with a set of questions. The questionnaire used in this study was a modified form of the Brice questionnaire, 14 which has been used in similar studies designed to assess intraoperative awareness in the past.
After the questionnaire was completed, it was analyzed, and patients were categorized into either having definite awareness, possible awareness, or no awareness. The patients had recalled more than one of the positive responses, and the events recalled by the patients were confirmed by attending personnel present in the operation theater; those patients were categorized under definite awareness. The patients were unable to recall any events, but their memories were related to intraoperative events, which was indicative of awareness. Those patients were categorized under possible awareness. Patients with no reported awareness were categorized under no awareness. 15
Statistical Analysis
Data were organized using a Microsoft Excel® sheet and analyzed using Statistical Package for the Social Sciences® version 23 (SPSS Inc., Chicago, IL, USA) for Windows. The data were expressed as ratios and proportions.
Results
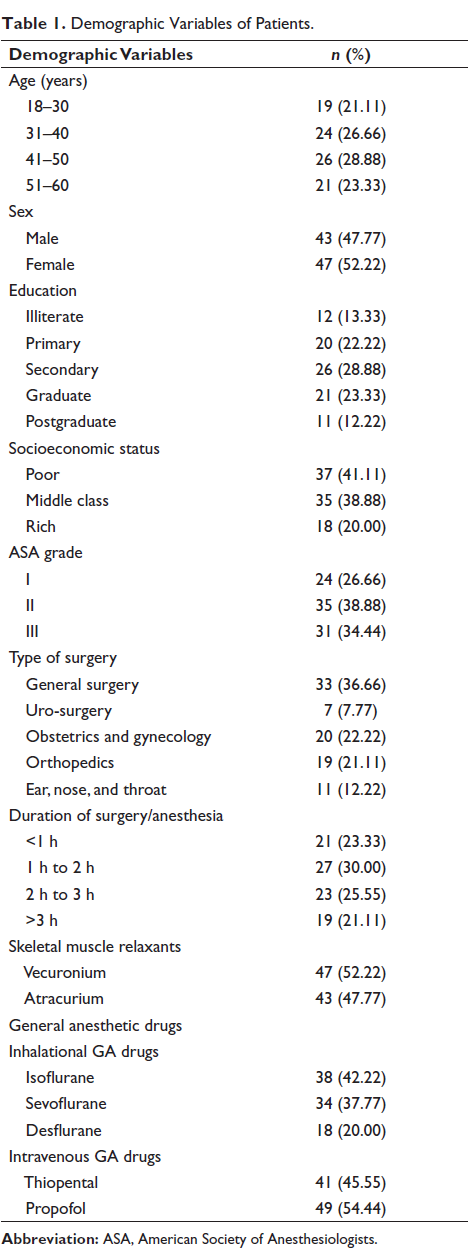
Patients were comparable with respect to age, gender, and ASA distribution (Table 1). There was no disruption of anesthesia or circuit failure in any case.
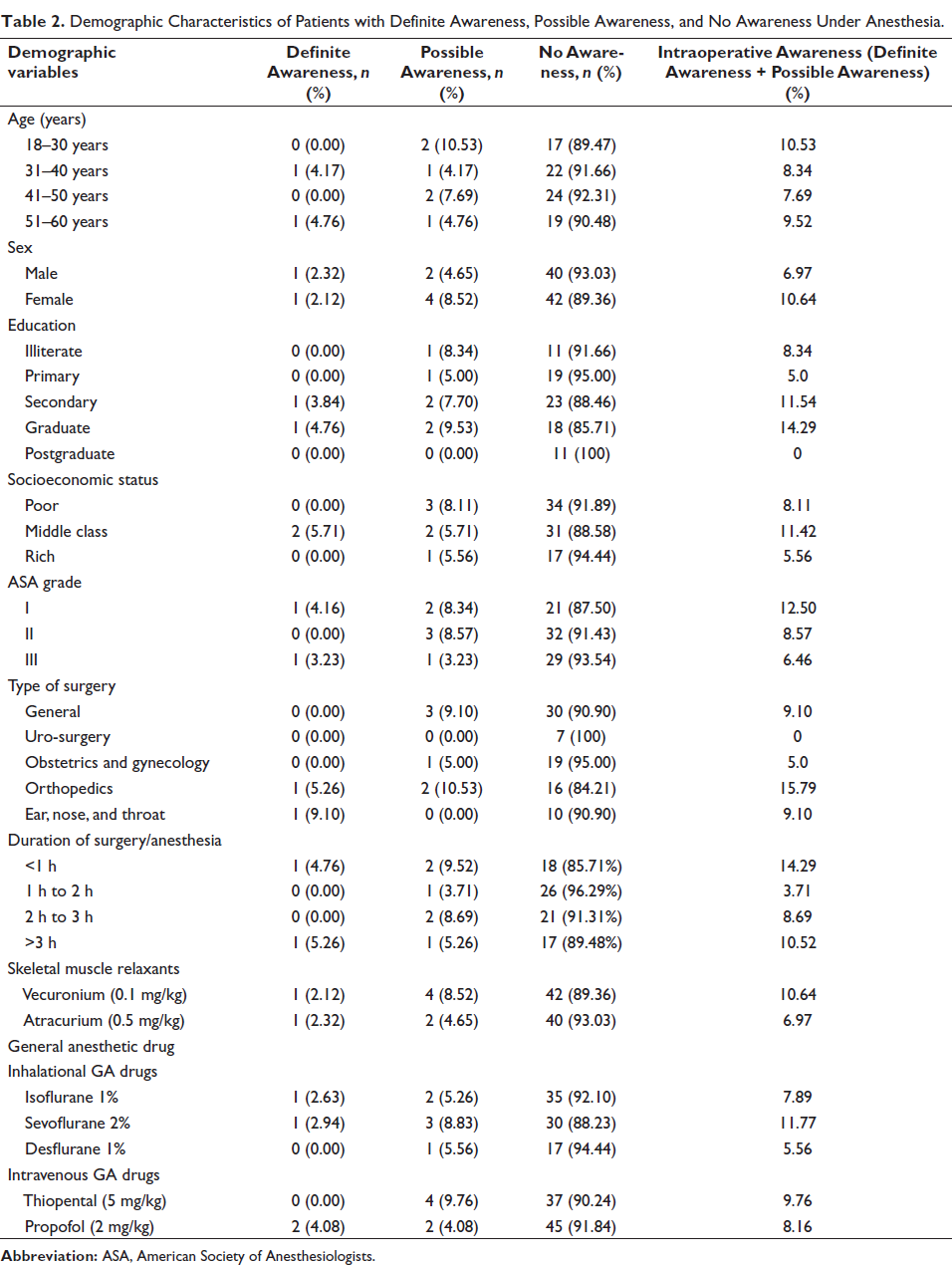
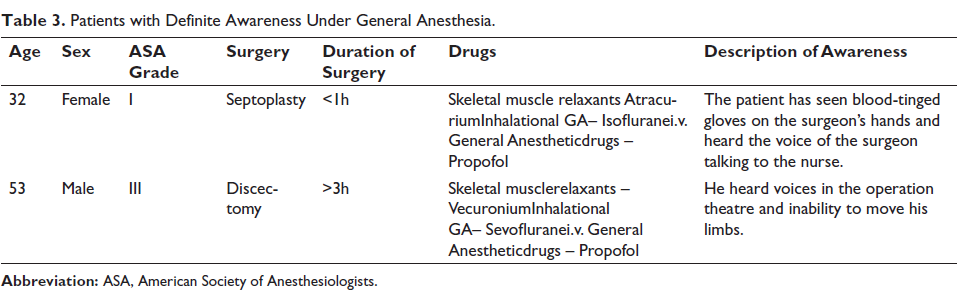
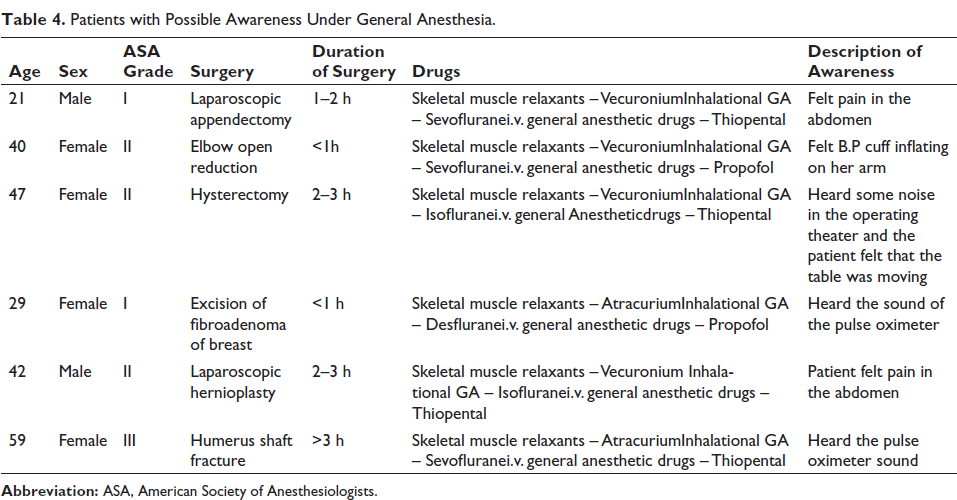
From Table 2, it is observed that out of a total of 90 patients, 90 operated under general anesthesia. Eight patients reported to have remembered something under general anesthesia. Out of eight patients, two patients (Table 3) were found to have definite awareness in our study, and the occurrence of definite awareness was calculated to be 2.22% in our study. Six patients (Table 4) were categorized under possible awareness, and the occurrence of possible awareness was calculated to be 6.6% in our study.
Demographic Variables of Patients.
Demographic Characteristics of Patients with Definite Awareness, Possible Awareness, and No Awareness Under Anesthesia.
Patients with Definite Awareness Under General Anesthesia.
Patients with Possible Awareness Under General Anesthesia.
Discussion
The positive responses that indicate intraoperative awareness are the actual memories of discussions and noises in the operating theater, tactile sensations, and feelings of muscle paralysis, pain, or distress that may be recalled later in the postoperative period. 11 In our study, we have categorized intraoperative awareness with recall under general anesthesia into definite awareness, possible awareness, and no awareness. If the patient had recalled more than one of the above positive responses, it was categorized under definite awareness, and if the patient had recalled one of the above positive responses or was unable to recall an event definitely. Still, there was an indication of awareness, and the patient was categorized under possible awareness. Patients with no reported awareness were categorized under no awareness.
Awareness under anesthesia, however, could be avoided if an adequate depth of anesthesia is maintained during surgery. Monitoring by an experienced anesthesiologist using hemodynamic variables (such as heart rate and blood pressure), lacrimation has been done traditionally to maintain adequate depth of anesthesia. Although effective, awareness can still occur without any variation in vital parameters. Similarly, BIS monitoring has been used to maintain an adequate depth of anesthesia. It measures the specific electrical activity of the brain with electrodes placed on the patient’s forehead and generates a numerical value that ranges from 0 to 100. A BIS value of 40–60 has been associated with a low probability of awareness under anesthesia.16, 17
The dose selection of general anesthetic drugs should be based on the patient’s requirements. Compared to adult patients, there is a 25% increase in minimum alveolar concentration (MAC) for volatile general anesthetic agents in children and a 25% reduction in elderly patients. Similar to the MAC concept, there is a minimum inhibitory concentration (MIC) for intravenous drugs, which has greater variability. 18
Various factors associated with resistance to general anesthetic drugs include hyperthyroidism, pyrexia, anxiety, obesity, young age, alcohol, smoking, use of recreational drugs (e.g., amphetamines, opioids, and cocaine), chronic use of sedatives like temazepam, and repeated exposure to general anesthetic drugs. 19 The factors that cause a reduction in MAC include pregnancy, hypothyroidism, hypocapnia, hypotension, increased atmospheric pressure, hypothermia, and old age. Increased atmospheric pressure does not alter brain sensitivity to general anesthetic agents but increases the inspired and brain partial pressures for a given inspired concentration of general anesthetic drugs. The depth of anesthesia is directly related to the partial pressure in the brain.
In our study, patients were given 2% of sevoflurane, 1% of isoflurane, or 1% of desflurane, regardless of their weight. The MAC valve of inhalational general anesthetic agents was not measured due to the poor availability of equipment in our institute. At the same time, induction agents and skeletal muscle relaxants were given according to the patient’s weight. The current study shows that, compared to desflurane, the drugs sevoflurane and isoflurane have a higher magnitude of intraoperative awareness. Further studies with more patients might be required to estimate the variation of inhalational general anesthetic drugs that influences intraoperative awareness.
Our study shows a higher magnitude of intraoperative awareness than other recent studies in western countries. Our study data showed that intraoperative awareness is more common in younger patients and ASA grade 1 patients. This might be due to the faster metabolism of the drug. The occurrence is common in females. Based on the duration of surgery/anesthesia, shorter durations, that is, <1 h, and longer durations of anesthesia, that is, >3 h, showed an increased magnitude of intraoperative awareness, which might be due to the inadequate depth of general anesthesia maintained during the surgery. Among the inhalational general anesthetic drugs, sevoflurane has a higher magnitude of intraoperative awareness, which might be due to its lower blood:gas partition coefficient.
Our study showed that an inadequate dose of inhalational general anesthetic agents was used, which was not appropriate for the patient’s weight, or that anesthesia was not maintained according to the MAC values. This was the only significantly associated factor for the occurrence of intraoperative awareness with recall under general anesthesia. Hence, further studies with more patients might be required to estimate the incidence and factors associated with intraoperative awareness under general anesthesia with greater accuracy.
Conclusion
The current study revealed a very high magnitude of intraoperative awareness with recall under general anesthesia compared to other studies. Hearing voices and pain were the two common intraoperative events recalled by patients who had intraoperative awareness with recall under general anesthesia. The occurrence of intraoperative awareness was estimated to be 8.8%, which includes both definite and possible awareness under general anesthesia. Finally, we conclude that intraoperative awareness might be due to the inadequate depth of general anesthesia given to the patients. The dose of general anesthetic drugs was not maintained based on its MAC.
Consort Flow Diagram Depiction of the Study.
Footnotes
Abbreviations
AAGA, accidental awareness during general anesthesia; ECG, electrocardiogram; GABA, gamma-aminobutyric acid; BIS, bispectral Index; PACU, post-anesthesia care unit; ASA, American Society of Anesthesiologists; MAC, minimum alveolar concentration; MIC, minimum inhibitory concentration; TIVA, total i.v. anesthesia.
Acknowledgments
The authors would like to thank the Faculties of Anaesthesia Department and Pharmacology Department, SSSMC&RI.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from Institutional Ethics Committee (IEC NO. 2020/607).
Funding
The authors received financial support for the research, authorship and/or publication of this article: STS ICMR (STS ICMR 2020. PROJECT ID: 2020-10300).