
Abstract
Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) has spread rapidly and diffused to more than 180 countries at varying severities. This pandemic has accounted for increased mortality and morbidity in developed as well as developing nations. The WHO has announced that there is a persistent need for the evaluation of the COVID-19 vaccine effectiveness (VE) against major outcomes, which include severe diseases, symptomatic COVID-19, and mortalities related to COVID-19. Therefore, mass vaccination programs using vaccines of high effectiveness are among the strategies that have been used by governments worldwide to impede the COVID-19 pandemic transmission. In this regard, massive efforts were made by governments, scientists, biomedical researchers, and healthcare professionals leading to the successful development of various vaccines to bring this pandemic under control. This editorial aims to shed light on the epidemiological status of COVID-19 variants, namely, Delta, Omicron, and Deltacron variants as well as discuss the effectiveness of the currently available COVID-19 vaccines.
Introduction
As the new coronavirus continuously evolves, a persistent spread of infectious mutations has been observed, and by the end of 2019, new mutations of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) were discovered at different geographic locations. The difficulties associated with controlling of the virus at such a large-scale epidemic have led to massive virus replication and increased the chance of adaptive mutations. 1 New variants of coronavirus have proliferated and caused concerns about the adaptability, disease changes, and transmission of the virus. The World Health Organization (WHO) has provided a classification for the new variants to fall into three main categories: variants of interest (VOI), variants of concern (VOC), and variants under monitoring (VUM). 2 The emergence of these new variants has caused various effects on diagnostic, therapeutic, and public health strategies. 3
SARS-CoV-2 has spread rapidly and diffused to more than 180 countries at varying severities within 3 months. 4 This pandemic has accounted for increased mortality and morbidity in developed as well as developing nations.5–7 Massive efforts have been made to understand the genomic structure of the coronavirus, and efficient vaccines have been developed. 8 However, the new daily cases of coronavirus despite administering COVID-19 vaccines are still being recorded due to the lowered immunization coverage resulting from the adaptive mutations in the SARS-CoV-2 genome which altered the virus’s pathogenicity, infectivity, and virulence. 9 More than 4000 mutations were recognized in the spike protein of SARS-CoV-2 since 2019; however, only a few number of these mutations were capable of altering the immune characteristics of the virus. The variants that have shown the greatest impact on the virus function appeared initially in the United Kingdom, South Africa, India, and Brazil. 10
The WHO has announced that there is a persistent need for the evaluation of the COVID-19 vaccine effectiveness (VE) against major outcomes, which include severe diseases, symptomatic COVID-19, and mortalities related to COVID-19. 11 Statistically, the VE against non-specified or wild-type SARS-CoV-2 infections strains were 47–66% for the inactivated viral vaccine, 12 62–71% for the viral vector vaccines, 13 and 91–93% for mRNA vaccines. 14 Recently, increased concerns regarding the lower VE against the delta variant have arisen compared to non-delta variants (53–66% vs. 75–91%).15–17 However, the VE of BNT162b2 vaccine against the delta variant infection has been shown to be considerably high in the first month (93%) and decrease to 53% four months later. 18 In this regard, massive efforts were made by governments, scientists, biomedical researchers, and health care professionals as a result of which various vaccines have been finalized and have been developed to bring this pandemic under control. 2 This editorial aims to shed light on the epidemiological status of COVID-19 variants, namely, Delta, Omicron, and Deltacron variants as well as discuss the effectiveness of the currently available COVID-19 vaccines.
Epidemiological Update on COVID-19 Variants
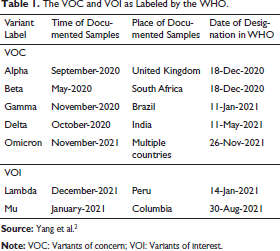
A collaborative work between the WHO and national authorities, researchers, and institutions provides weekly assessments for the SARS-CoV-2 variants and their ability to alter the disease’s characteristics and transmission, or their impact on the VE, diagnostic, therapeutic, or public health and social measures (PHSM) that are applied for controlling the disease spread. 19 Table 1 summarizes the VOC and the variants of interest as labeled by the WHO. 2
The VOC and VOI as Labeled by the WHO.
COVID-19 Delta Variant
The Delta variant or the lineage B.1.617 has been recently discovered. 10 Initially, this variant was detected in October 2020 in Maharashtra, India, with more than 400,000 new cases recorded and about 4,000 deaths per day. 20 The rapid outbreak of the Delta variant has emphasized this variant’s high transmissibility and has been later on labeled by the WHO as a VOC. 21 Infections that pose a higher growth rate and increased contagiousness indicate an alteration in the virus’ epidemiological characteristics. 22 In a study that has been carried out in China, the epidemiological profile, as well as the dynamics of the delta virus’ transmission, were assessed and measured in 68 infected patients. Results of the same study have reported a generation time (GT) of 2.9 days between the primary and the secondary cases, which when compared to previous variants, is considered shorter. 23 In other recent studies it has been reported that the viral load has been 1,000 times more in people infected with the Delta variant when compared to those infected with prior coronavirus versions. This indicates a relevance to the increased virus’ transmissibility rather than the pathogenicity. 24 Epidemiological investigation has shown that the incubation period of the Delta variant was 2-3 days, which is relatively shorter as compared to the wild-type strain with an incubation period of 3-7 days.25–27 Other epidemiological studies which have been carried out in Guangzhou showed that Delta variant infection could spread in a very short time even in cases where patients did not share the same space. 28 These data suggest that the spreading of the Delta variant may also happen via aerosol, which leads to enhanced interpersonal transmissibility. 10 Several studies have shown that patients infected with the Delta variant are twice more likely to require hospitalization when compared to the ancestral strain of the virus. However, the fatality–case ratio with the Delta variant has been shown to be less (1.7%) than the main strain (3%). 29 As of now, this variant has been reported as the largest circulating virus, which has shown a predominance in 135 countries, with the highest cases number reported in Iran and the United Kingdom. 10
COVID-19 Omicron Variant
Initially, the Omicron variant was detected in Africa; however, from the data that have been given, the exact origin is not yet confirmed. As of March 31, 2022, cases of this variant have been reported in 188 countries and has already become globally dominant, with 99.7% submitted sequences from February to March 2022. 30 There are four main sublineages that emerged from this variant, namely, BA.1, BA.1.1, BA.2, and BA.3, with the BA.1, BA.1.1, and BA.2 being the most circulating. 31 An epidemiological study that has been recently carried out in Denmark suggested that the effective reproduction number (Re) of the BA.2 sublineage was 1.26 times higher than that of the BA.1; however, a recent estimation for the Re of 0.75 was also reported. 32 The European Centre for Disease Prevention and Control stated that the Omicron variant could have a higher transmissibility than the Delta variant. The collective evidence shows that this variant has a higher infectivity rate and more potential to cause reinfection when compared to the predecessors; however, the data provided are insufficient and are yet to quantify the overall impact of this variant.33, 34 Recently, evidence from South Africa suggested that no peculiar symptoms have been associated with the omicron variant, and some individuals were asymptomatic and others showed mild symptoms only. 34 Seven of every 10 cases among the early reported cases with the Omicron variant were symptomatic and the age range was shown to be between 20 and 49. 35 Patients who had preexisting conditions, in addition to other patients who had acute respiratory attacks, were among the cases that were hospitalized. 36 Omicron variant has weakened the connotation between the number of cases and mortality. As proposed by UK-based evidence, the Omicron case rate has accounted for a daily percentage of 35%; however, the mortality rate has shown a continuous decline as opposed to the patterns that have been previously observed in the first pandemic wave. 33 Additionally, data have shown that every 3 in 10 infected individuals were fully vaccinated, suggesting that this variant can evade the immune response. 37 Neutralization studies and studies on the risk of reinfection have shown a greater prevalence of Omicron variant in comparison to the Delta variant; however, extensive effort is needed to provide an estimation for the GT of the Omicron variant when compared to other variants and get a better understanding on whether this variant has properties that render it more transmissible. 4
COVID-19 Deltacron Variant
It has been stated by virologists that many SARS-CoV-2 genomes that have the Delta and the Omicron variants have been discovered by a research team at the University of Cyprus in Nicosia (Figure 1). 38 In France, 33 cases of the delta variant, 8 cases in Denmark, 1 case in Germany, and 1 case in the Netherlands were recorded in an update given on March 10, 2021. 39 The Deltacron has not been labeled as a VOC due to the limited number of infection cases that have been confirmed. 40 In a study that has been carried out in France, data have revealed that three genomes that have been taken in the time between January and February 2021 have been phylogenetically related to the Delta 21J/AY.4-Omicron 21K/BA.1 hybrid genomes that were previously discovered in Denmark, northern France, and the Netherlands. 41 The Deltacron was labeled by the WHO as a VUM on March 9, 2021, which indicated that it may show a future risk; however, this assumption is lacking any evidence. 42 Remarkably, Pfizer has recently proclaimed that the fourth dose of its authorized vaccine will provide better protection against the variants that are currently confirmed as well as future variants. 43 In conclusion, it is of great importance to monitor this recombinant’s behavior throughout molecular surveillance, specifically, during times of high viral circulation, for better detection of coinfections and recombinations. 44 Moreover, it is also crucial that further clinical cases that involve coinfections be analyzed for a better understanding of this recombination’s influence on the replication of the virus, its mode of transmission, the severity of the infection, and the ability of the virus to escape the neutralizing antibodies demonstrated by either vaccines or previous infections. 45
The Emergence of Deltacron COVID-19 Variant. 38

The Effectiveness of COVID-19 Vaccines
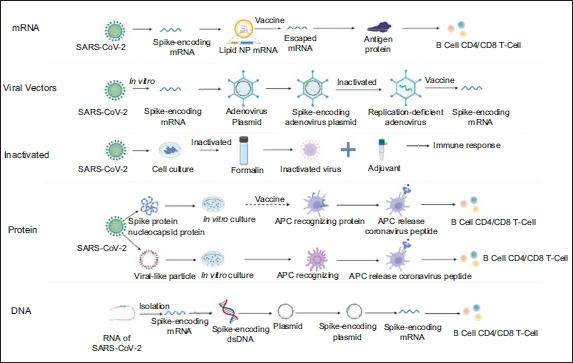
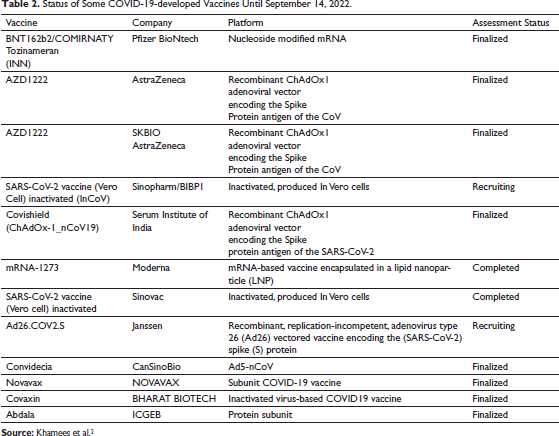
Since the first reported COVID-19 case, unprecedented efforts on a global scale have been given for designing, manufacturing, and testing several vaccines. Collectively, five vaccine types have been authorized to be used clinically, namely, mRNA vaccine, replicating and non-replicating viral vectors vaccine, inactivated virus vaccine, protein vaccine, and DNA vaccine, as shown in Figure 2. 46 Additionally, in the pursuit of having effective control over the spreading of this epidemic, other vaccine types are still under evaluation, such as the live attenuated vaccines.46–48 Recent clinical experimental studies have shown that each vaccine type has its distinctive immune mechanism, pros and cons, and efficacy and effectiveness (Table 2). 49
Coronavirus Vaccine Platforms. 46
Status of Some COVID-19-developed Vaccines Until September 14, 2022.
In Phase III clinical trials, high VE has been observed against SARS-CoV-2 infection, for instance, 70.4% VE has been reported for Oxford-AstraZeneca, 13 95% for Pfizer-BioNTech, 14 94.1% for Moderna, 50 and 50.7% for CoronaVac. 51 The vaccines produced by Pfizer-BioNTech and Moderna were authorized worldwide for clinical use in December 2020, which as a result had a crucial role in the control of the pandemic spread. 52 It is worth mentioning that the mRNA vaccines were shown to exert a high efficacy against the first major mutation of the original strain (D614G). 53 Also, they are effective in reducing hospitalization rate and mortality.54–56 As for viral vector vaccines, Ad26.COV2.S and AZD1222 have shown extremely high prevention on Delta variant’s hospitalization, and they also have demonstrated neutralizing antibody (NAbTs) of more strength against all the strains when compared to mRNA vaccines. 57 In conclusion, the decision of selecting a vaccine type should be made in accordance with the regional epidemiological situation. 46 Lately, mass vaccination programs using vaccines of high effectiveness are among the strategies that have been used by governments worldwide to hinder the transmission of the COVID-19 pandemic. Concerns have appeared regarding the lower effectiveness against Delta variant when compared to those against the other variants, such as the alpha, beta, and the non-specified variants (53–66% vs. 75–91%), 15 while the VE of BNT162b2 vaccine against the delta variant has been shown to be higher in the first month (93%), and declines after 4 months to 53%. 58 The WHO has stated that it is urgently needed to provide an evaluation for the COVID-19 VE for many major outcomes, which include symptomatic COVID-19, severe diseases, and mortalities related to COVID-19.
Summary
To detect the emerging COVID-19 variants, extensive surveillance of both genetic and antigenic alterations in the population of the virus is required, along with widespread experiments that aim to elucidate the phenotypic implications of these variants. Given the current settings, it is of critical importance to comprehend the influence of a number of risk factors including vaccine ineffectiveness, vaccination rate, restrictions on the infection dynamics and waning immunity, as well as the individuals who will never receive the vaccine. Various models have been recently developed to introduce new vaccination strategies.59–63 However, it is worth mentioning that even after developing COVID-19 vaccines, the uncertainty relies at determining the effect of SARS-CoV-2 strains mutations on these vaccines’ effectiveness. Efforts on a global scale are given to attempt to eradicate the COVID-19 pandemic and to develop effective COVID-19 vaccine candidates. Recent clinical trials are showing promising results; however, extensive research is still necessary to determine the safety and efficacy of these vaccines. Finally, developing and introducing a novel vaccine for clinical use is a process that requires multiple stages and a relatively long time. Additionally, producing and distributing a massive number of doses of these vaccines are expected to be problematic.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
Not applicable.
Funding
This work was supported by the Durban University of Technology and the National Research Foundation, South Africa (Grant numbers 129173 and 129330).
Informed Consent
Not applicable.