
Abstract
Diabetic ketoacidosis (DKA) is a medical emergency caused by the lack of insulin. Metabolic acidosis, hyperglycemia, and ketoacidosis are its defining features. Insulin deficiency can cause DKA either in the presence or absence of a triggering event causing a chain of pathophysiological changes. Normalizing volume status, hyperglycemia, electrolytes, and ketoacidosis are the objectives of DKA treatment. While hospital pharmacists are involved in managing DKA, community or ambulatory care pharmacists can help to prevent DKA. Depending on the particular field of practice, a pharmacist’s engagement in DKA may involve a number of factors. Inpatient pharmacists are in a good position to help with the acute care of DKA. Because they can recognize patients who are at risk for DKA due to factors including medication nonadherence or insulin pump failure, pharmacists in the community or ambulatory-care environment play a crucial role in its prevention. When a patient finds it challenging to navigate prescription plan coverage or a lack of coverage, community pharmacists can help them obtain insulin. Regardless of the professional environment, patient education is essential. Every pharmacist has the ability to give DKA patients thorough medication education that emphasizes the value of adhering to their drug schedule, addresses any obstacles that may occur, and teaches patients how to correctly monitor their blood glucose levels. Studies showed that pharmacists’ medication counseling and treatment monitoring could improve adherence to insulin medication. The aim of this review is to provide evidence that pharmacists can contribute to optimizing medication adherence and decrease the incidence of DKA.
Keywords
Abbreviations
CDTM: Collaborative Drug Therapy Management
DKA Diabetic ketoacidosis
IM: Intramuscular
IV: Intravenous
PDC: Proportion of days covered
SC: Subcutaneous
Introduction
Diabetic ketoacidosis (DKA) is a serious diabetic complication indicated by ketonemia, hyperglycemia, and metabolic acidosis. Elevation of counter-regulatory hormones (glucagon, cortisol, catecholamines, and growth hormone) are the result of an absolute or relative decrease in the amount of circulating insulin. 1 Increased gluconeogenesis, glycogenolysis, and decreased peripheral glucose uptake all contribute to the development of hyperglycemia in DKA. Adipose tissue releases free fatty acids into the bloodstream, which the liver then oxidizes into ketone bodies, causing ketonemia and acidosis. 2 Infection, newly diagnosed diabetes, noncompliance with medication, and inadequate insulin administration are some of the frequent triggering causes of DKA. Globally, in the health-care field, hyperglycemic crises has become a major challenge associated with high rate of mortality. Hyperglycemic crises continue to be a frequent reason for visits to the emergency room, despite recent declines in death rates. About 207,000 people in the United States sought treatment for a hyperglycemic emergency in 2014, and in 2017 there were 2,20,340 admissions. 3 Epidemiologically, this trend was similar in England, Finland, Kuwait, Canada, and Germany with the highest rate in United Arab Emirate and Saudi Arabia.4-6 Although this disease is very common, there is still disagreement over how to treat it. It is believed that bolus insulin delivery shortens the time it takes for DKA to resolve and lowers the overall amount of insulin required. 3
DKA is related to the higher rates of morbidity and mortality, particularly in young people with type-1 diabetes. For type-1 diabetics under the age of 24 years, it is the main cause of death. An estimated 27% to 37% of DKA patients had recently been diagnosed with diabetes, typically type 1. In people with type-2 diabetes, infection, trauma, or surgery may increase the chance of developing DKA. Generally, the underlying disease or comorbidity is connected with DKA mortality. 7
Ketoacidosis, metabolic acidosis, and severe hyperglycemia may be indicative of DKA. However, DKA can manifest in different ways, either as mild euglycemia to severe hyperglycemia, and could be associated with dehydration and coma. Based on a patient’s clinical characteristics, each patient’s treatment plan is highly personalized. 1
The Canadian Diabetes Association, the American Diabetes Association, and the British Diabetes Societies, among others, all have clinical practice guidelines for the management of DKA. These guidelines aim to enhance the quality of medical-plan outcomes and evaluate the gaps between clinical practice and evidence-based perceptions. Furthermore, these guidelines make the clinical decisions more accurate by outlining the fundamental research findings.
These recommendations differ in certain ways, which could lead to inconsistencies in how clinicians manage DKA. 6 The success of such clinical guidelines is associated with the pharmacists’ support as they play key role in this regard. While hospital pharmacists are involved in managing DKA, community or ambulatory care pharmacists can help to prevent DKA. 8
Causes of Diabetic Ketoacidosis
DKA is brought on by insufficient insulin and an endocrine system reaction that raises catecholamines, cortisol, glucagon, and growth hormone. 7 Hyperglycemia is caused by the release of regulatory hormones that are stimulated by an absence of insulin or other triggering factors. Hyperglycemia is caused by increase in gluconeogenesis and glycogenolysis and lack of glucose utilization. Diuresis brought on by hyperglycemia further contributes to dehydration, unstable electrolytes, and renal failure. Lipase breaks down adipose tissue for energy since the body cannot utilize glucose, part of which is converted into ketones and causes ketoacidosis. 8
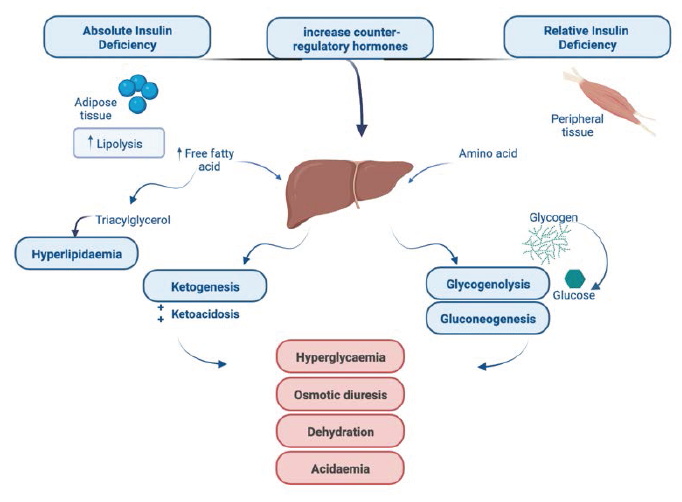
More precisely, hyperglycemia with ketosis occurs in DKA as a result of markedly lower insulin levels and elevation in counter-regulatory hormones (catecholamines, cortisol, glucagon, and growth hormones). Figure 1 illustrates how increased hepatic gluconeogenesis and glycogenolysis together with a reduction in glucose absorption into peripheral tissues lead to hyperglycemia. Free fatty acids and the hormonal imbalance also contribute to resistance to any leftover insulin. Osmotic diuresis, which is brought on by the rise in blood glucose levels, results in considerable electrolyte and water loss.1, 9
Treatment of Diabetic Ketoacidosis
Adherence to national or institutional guidelines improve the treatment outcomes. According to American Diabetes Association, DKA is a medical condition that required instant critical care. The goal of DKA therapy intended to normalize hyperglycemia, electrolytes, ketoacidosis, and fluid volume status. It is essential to identify and take care of any additional possible triggering variables; the proper implementation of such treatments is associated with pharmacists’ support.
Insulin Therapy
Insulin administration is fundamental in DKA management in order to stimulate glucose consumption, and decrease glycogenolysis, gluconeogenesis, and ketogenesis. Prior to starting insulin therapy, volume resuscitation is crucial since insulin may make dehydration worse. Minimum level of potassium has to be 3.3 mEq/L before starting insulin therapy. 11 Insulin increases glucose consumption by peripheral tissues by reducing gluconeogenesis, glycogenolysis, and ketogenesis. Regular insulin can be given as an initial IV bolus of 0.1 unit/kg then starting a continuous infusion at a rate of 0.1 unit/kg/hour or 0.14 unit/kg/hour. Then after the first hour of this infusion, if the plasma glucose levels have not decreased by 10%, another bolus of insulin (0.1 units/kg or 0.14 units/kg, respectively) may be administered before continuing the infusion at the prior pace. The insulin rate may be reduced by half or by 0.02–0.05 unit/kg/hour, after plasma glucose reaches 200–250 mg/dL. To avoid hypoglycemia dextrose should also be added to the maintenance intravenous fluids. 12
For patients with DKA, administering insulin intravenously is preferable. Fisher and colleagues examined the administration of low-dose insulin treatment via the IV, IM, and SC routes in a randomized, prospective experiment. A 1:1:1 strategy was used to randomize 45 patients. 13 When compared to the IM and SC methods, IV insulin showed a brisker drop in hyperglycemia and ketonemia within the first two hours of treatment. Eight hours after treatment, the three groups displayed comparable reactions. 13 Further research has been done using insulin administered via the SC route to treat DKA. In an intensive care unit, insulin aspart and insulin lispro SC every one to two hours are equally as secure and efficient when compared to continuous insulin infusion. The recommended dosage is 0.2 units/kg at first, then 0.1 units/kg every hour, or 0.3 units/kg at first, then 0.2 units/kg every two hours, until the blood glucose level is less than 250 mg/dL. In order to treat the DKA, insulin dosage should now be reduced to 0.05–0.1 unit/kg every 1–2 hour. The duration of hospitalization, rate of hypoglycemia, and time to DKA resolution were comparable across the two groups. 14 Additionally, it has been proven that SC rapid-appearing insulin analogues are efficacious and fairly priced for treating simple mild-to-moderate DKA.15, 16
After the DKA has subsided, patients who can eat can start taking long-acting insulin and premeal rapid-acting insulin to control their blood sugar levels. A continuous infusion of insulin should be given for at least one hour following SC insulin administration in order to ensure that plasma insulin levels are appropriately controlled. 1
Fluid Replacement
DKA patients regularly suffer from hyperosmolar intracellular dehydration. Immediate rehydration without insulin therapy can correct electrolytes imbalance and retrieve body fluid and tissue perfusion; this would help control glycemia and acid-base balance. Rehydration enhances low-dose insulin therapy. Fluid loss in DKA might be between 6 and 9 L. About half of the total volume has to be replenished within the first 8–12 hours, then the remaining volume should follow within 24–36 hours. For optimum outcome, crystalloids in 1–1.5 L of sodium chloride solution (0.9% solution) given throughout the first hour (15–20 mL/kg/hour). 12 In a prospective, randomized research undertaken by Caputo et al., 27 patients were divided into two groups treated with 0.9% saline solution;14 of them have it at rate of 1,000 mL/hour, and 13 at a rate of 500 mL/hour. 17 Between the two groups, there were no discernible changes in metabolic problems or rates of mortality. 17 Fluid replacement needs to happen as soon as feasible because doing so can reduce fluid administration times and increase efficiency.
Then, the rate of hydration should be determined by the following factors: electrolytes, urine output, hemodynamic status, and hydration status. When the plasma glucose falls below 200 mg/dL, 5% dextrose should be added to the replacement fluids to prevent hypoglycemia. Insulin therapy should be continued at a slower rate until the ketonemia is resolved. 12 Care should be taken while hydrating patients who have fluid retention, such as those with chronic kidney disease or heart failure. 1 The amount of urine produced is crucial for monitoring these patients.
Electrolytes
DKA is frequently accompanied by total serum electrolyte deficiency, which includes sodium, chloride, and potassium, and require immediate intervention to avoids cardiac/respiratory complications and weakness of muscle.
In DKA and other hyperglycemic crises, potassium levels are typically low. When insulin binds to its receptor on skeletal muscle, potassium is moved intracellularly into muscle cells. Hypokalemia will occur in about two-thirds of patients receiving treatment for DKA. 18 In patient with normal renal function, whenever serum potassium level drops below 5.3 mEq/L, potassium replacement should begin. Potassium supplements of 20–30 mEq may be added to each liter of liquids. The first hour of insulin therapy may call for extra potassium in patients with severe hypokalemia. Potassium supplements can be given as potassium phosphate, since potassium chloride can cause hyperchloremic acidosis. Insulin therapy should be postponed until the potassium levels return to normal if there is substantial hypokalemia (3.5 mEq/L). Arrhythmias in hypokalemic patients should be closely watched. 19
Bicarbonate use is debatable because there aren’t adequate trials. The use of bicarbonate therapy in 21 people with DKA has been studied by Morris and colleagues. 20 They found that the rate of rise in pH, serum bicarbonate levels in the blood or cerebrospinal fluid, or the fall in glucose or ketonemia did not benefit from bicarbonate therapy. The DKA resolution rates of the two groups were comparable. 20 At this time, there is no research to back up the use of bicarbonate in DKA patients with pH levels below 6.9. It is advised that the clinical condition of the patient be taken into consideration while deciding whether to utilize bicarbonate.21, 22 Patients who have severe acidosis and a pH less than 6.9 may receive 100 mmol of sodium bicarbonate in 400 mL of sterile water along with 20 mEq of potassium chloride at a rate of 200 mL/hour for two hours, or until the venous pH is higher than 7.0. Until the pH is greater than 7.0, this can be done every two hours. Bicarbonate may also be used to treat patients whose bicarbonate levels are less than 10 or whose partial pressure of carbon dioxide (PCO2) is less than 12, both of which can cause pH degradation. 12
The majority of people with DKA are not advised to take phosphate supplements currently. Usually, patients with DKA see a 1 mmol/kg drop in phosphate. Replenishment of phosphate has not demonstrated any extra advantages for clinical outcomes and may cause hypocalcemia. Phosphate supplementation may be advantageous for patients who could experience cardiac, muscular weakness, or rhabdomyolysis as a result of hypophosphatemia. Potassium phosphate concentrations of 20–30 mEq/L may be added to replacement fluids.23, 24
Role of Pharmacist
According to the American Society of Health-System Pharmacists, diabetes care can be significantly enhanced by pharmacists by screening patients at excessive risk for diabetes, monitoring their health status, encouraging them to take care of themselves, referring patients to alternative providers as necessary, and monitoring progress. Offering diabetes management services calls for marketing know-how, communication prowess, as well as a time, effort, and resource investment. Pharmacists who complete diabetes management training may experience career satisfaction and financial compensation.
Pharmacists should focus on patients at high risk, those with a family history of the condition, women with a history of gestational diabetes, and mothers who had babies that weighed more than nine pounds in order to help identify patients with diabetes through screening. Immediately after diagnosis, at a second stage when a patient evaluation may be done, and at a third stage when patients can get continuing education to reinforce concepts and give them a motivational boost, patient education should be offered. The pharmacist’s capability to refer patients to alternative members of the diabetes care team is one amongst their most important responsibilities. 25 Although the pharmacist’s role in managing diabetes is not clearly defined, it may involve checking doctors’ visits and tests to gauge long-term glycemic control. It is advised that diabetic educators get certified. For this procedure to be successful, the applicant must have at least 1,000 hours of expertise managing diabetes patients’ illness states. The implementation of diabetes management services necessitates a commitment of time, energy, and resources, and may call for staff training and adjustments to work schedules. 26
Studies showing the value of pharmacists in the treatment of diabetes, as well as their proficiency in medication management, underline the significance of these professionals as members of interdisciplinary teams. 27 In particular, pharmacists who are board-certified pharmacotherapy experts, certified diabetes educators, or board-certified in advanced diabetes care may have a significant impact on patient outcomes when working under collaborative practice agreements. Smith et al. fervently supported the inclusion of pharmacists in models of team-based health-care delivery and suggested enhancing their function in the provision of primary care services. The authors came to the conclusion that diabetes, which is a disease state that is frequently encountered, and its monitoring and control might very well fit into this primary care service delivery model. 28
Adverse Drug Monitoring
The necessity for an interdisciplinary, shared obligation among pharmacists and doctors to enhance patient medication outcomes and control the cost-effectiveness of drug therapy regimens has become more obvious due to the complexity of current medication plans and the increasing accentuate on patient medication safety. For instance, in the United States of America, more than 75% of the states have legislated or amended state pharmacy practice laws to include a pharmacist’s involvement in the administration of a patient’s prescription therapy. 28
In collaborative drug-therapy management (CDTM), trained pharmacists (with the necessary clinical training and practice experience) collaborate with one or more doctors to conduct patient assessments, order drug-related laboratory tests, administer medications, and choose, start, monitor, and modify therapy regimens. The requirements for pharmacist education and training, practice locations, and state regulations all have a substantial impact on CDTM agreements. The cooperating health-care practitioners must ultimately decide on the precise pharmacist requirements and the range of CDTM responsibilities, taking into account patient demands, associated pharmacological therapies, and care setting variables. 29
Pharmacists can provide “continuity of care” by tracking patients’ care during physician visits. The use of their scientific knowledge to reveal and control diabetes treatment plans, and teaching patients about their medical conditions, lifestyle, and adherence issues. This is supported by a growing body of literature. 30
For better diabetic medication management, pharmacists can be a crucial resource working in an interdisciplinary pattern. This is in line with the medical home care, which encourages collaboration among health-care professionals in order to plan patient-centered care. By concentrating on medication management, pharmacists can improve patient outcomes, lower total health-care system costs, and give patients and consumers the tools they need to take charge of their own health.
Medication Adherence and Noncompliance
The good influence of pharmacists on medication adherence has been extensively documented, and diabetes and DKA management is no exception. Medication knowledge, device training, adherence calls, and pillbox filling are all examples of interventions for medication adherence. In one study, the effect of the pharmacist was assessed using telephonic interventions and PDC-measured medication adherence. PDC, a widely used adherence indicator, examines the percentage of days a patient is covered in relation to the prescription dispense date and supply. A pharmacist contacted patients with less than 80% PDC and monitored them for three months. Following the intervention in three months duration, 69% of patients taking antihypertensives and 64% of patients taking oral diabetes medications were capable to reach a PDC of more than 80%. 31
Medication adherence can also be affected by education after returning from a hospital stay to an outpatient setting. In a randomized controlled trial, discharge education resulted in better PDC of 55.2% versus 34.8% (P = .002) and better adherence to follow-up visits (60.5% vs 43.9%; P = .01) in patients with an HbA1c > 8% who filled their diabetes medication at a pharmacy within the health-care system. 32 This exemplifies the significant influence pharmacists can have on the timing of release, particularly in a health-care system that oversees all aspects of the patient’s treatment.
In another research, the pharmacist personally called patients whose prescriptions for oral diabetic medication were at least six days past due. The pharmacist made personal calls to patients to learn about their main problems, filled their medications, and then carried out an intervention. The researchers discovered that difficulties taking drugs (27.1%), remembering the dose (24.6%), and forgetting to ask for a refill were the three most often reported patient adherence issues (26.3%). The pharmacist used interventions like medication education (35.6%), glucometer education (28%), and implementation of strategies to support adherence (40.7%). The intervention group had a much higher ratio of medication possession as compared to the standard of care. 33
Patients’ Reliance on Pharmacists
By working with the doctor, pharmacists can improve medication management as a member of the diabetes care team. Pharmacists can now integrate their role within the diabetes care team to offer a comprehensive approach to diabetes treatment thanks to the shift from product-focused retail to patient-focused service provider. According to a recent systematic review, several pharmacy services—including counselling, leaflets, medication reviews, patient group talks, and phone calls—have been developed to help patients with diabetes to better manage their medications. It has been demonstrated that these different services significantly improve medication compliance and glycemic target attainment. 34
Depending on the particular field of practice, a pharmacist’s engagement in DKA may involve a number of factors. Inpatient pharmacists are in a good position to help with the acute care of DKA. When a patient finds it challenging to navigate a prescription plan, or if coverage is lacking, community pharmacists can help them obtain insulin. Regardless of the professional environment, patient education is essential. Every pharmacist can give DKA patients thorough medication instructions, emphasizing the value of adhering to their drug schedule, addressing potential obstacles, and demonstrating how to monitor blood glucose levels correctly. 8
Conclusion
Studies showed that pharmacist’s medication counseling and treatment monitoring could improve adherence to insulin medication. Despite the provision of therapies, DKA manipulate stays suboptimal because of low adherence and numerous patient-associated factors. DKA control relies upon numerous factors, consisting of medicine adherence, right insulin dose intake, DKA education, and understanding the exacerbate of DKA symptoms.
In fact, pharmacist-led interventions improve diabetes control has been proven.
Footnotes
Acknowledgment
The author is immensely grateful to Dr Bayan S. Algarni—Consultant Internal Medicine/Endocrinology and Diabetes at King Faisal Hospital—for the insightful discussions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
Not applicable
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable