
Abstract
Objectives:
To determine the incidence and frequency of adverse drug reactions (ADRs) to find out factors, if any contributing to the same, while also exploring the use of amphotericin B deoxycholate as a cheaper and safe alternative to liposomal amphotericin B.
Materials and Methods:
It was a cross-sectional observational study, with a study population of 50 conducted over three months after ethics approval. All adult patients admitted to a tertiary care center, in a metropolitan city of Maharashtra, diagnosed with Rhino-orbito-cerebral mucormycosis, with a history of previous COVID-19 infection and receiving antifungals for the treatment of the same were included in the study. Central Drugs Standard Control Organization (CDSCO) ADR reporting forms were used to collect data.
Results:
Electrolyte disturbances mainly hypokalemia were the most frequently encountered ADR with both Amphotericin formulations (39/50; 20.31%) followed by pain at the injection site (33/50; 17.19%). Nephrotoxicity occurred slightly more frequently with Amphotericin B Deoxycholate (19/29; 65%), compared to Liposomal Amphotericin B (11/19; 57%), while Posaconazole was mainly associated with gastrointestinal (GI) disturbances and hepatotoxicity.
Conclusion:
Amphotericin B Deoxycholate was associated most with ADRs, hypokalemia, and pain at the injection site being the most frequent. However, concerning nephrotoxicity, both Amphotericin formulations showed only a modest difference. Posaconazole was associated with the least number of ADRs and had a favorable safety profile.
Keywords
Introduction
Coronavirus disease 2019 (COVID-19) associated Rhinoorbito-cerebral mucormycosis (ROCM) or COVID-19 associated mucormycosis (CAM) has become an issue of national public health concern in recent times. 1 ROCM has emerged from the sidelines as a major player in the contribution to patient morbidity, mortality, and permanent disability in a matter of months. 2 Amidst the second wave of the COVID-19 pandemic in India, there was a sharp increase in the number of cases of ROCM, reaching epidemic proportions with our center admitting 204 patients of CAM between March to July 2021 as opposed to a prevalence of 1.4% before this period.3, 4 This acute onslaught of mucormycosis has led to an increase in the use of antifungal agents most prominently, Amphotericin B Deoxycholate, Liposomal Amphotericin B, and oral Posaconazole, 5 and therefore a corresponding increase in the incidence of related adverse drug reactions (ADRs) to these agents is unavoidable.6, 7 The sudden increase in the demand also subsequently led to a national shortage of the aforementioned antifungals,8, 9 adding to the overall burden on the patients and health care system in the form of black-marketing, decreased availability of beds, and a shortage of medical staff. 10 Inappropriate use of antifungal agents may result in adverse events, unnecessary exposure, higher costs, and increased microbial resistance. It is important to know more about the ADRs induced by systemic antifungal drugs, as well as about the safety profiles of the different amphotericin B formulations in different clinical practice settings.11–13
This study aimed to determine the incidence and frequency of ADRs and also study the factors contributing to the same, while exploring the use of amphotericin B deoxycholate as a cheaper and safer alternative to liposomal amphotericin B.
Materials and Methods
The study was a cross-sectional observational study, with a sample size of 50 conducted over three months. All adult patients admitted to a tertiary care center, in a metropolitan city of Maharashtra, diagnosed clinically, microbiologically, or radiologically with ROCM, with a history of previous COVID-19 infections, and receiving antifungals for the treatment of the same were included in the study. Pediatric group patients and patients diagnosed with mycoses other than mucor spp. were excluded from the study.
Given that the prevalence of mucormycosis in India before the COVID-19 pandemic was 1.4%, 4 the sample size we were working with was based on the number of cases admitted to the hospital in the stipulated period, and not on previously available population statistics. Owing to the national shortage of antifungals used for the treatment of ROCM 9 patients were given different antifungals as per the availability. Naranjo Algorithm was employed to identify ADRs with the aforementioned antifungals. 14
Central Drugs Standard Control Organization (CDSCO) ADR reporting form was used for data collection. The variables recorded were nature of the reaction, duration of reaction, therapeutic response to the reaction, the dose of the incriminated drug along with general demographic data of each patient and associated comorbidities. Hartwig’s Severity Assessment Scale was used to assess the severity of the ADRs. 15 The data were entered into MS Excel and analyzed using descriptive statistics. The data were also analyzed for possible associations between the ADRs and other factors such as age, sex, comorbidities, and duration using the chi-square test.
Results
A total of 50 patients were recruited for the study, eight of which were female (16%) and 42 were male (84%). The ages of patients enrolled in this study ranged from 18 to 75, with the mean age being 51.8 years (SD ± 11.2). 43 of these patients were diabetic (86%), 20 were hypertensive (40%) and three patients did not have any comorbid conditions (6%).
All patients in the observed population experienced at least one ADR. Out of 50 patients, 29 patients experienced ADRs while on Amphotericin B Deoxycholate, 19 while on Liposomal Amphotericin B, and seven while on Posaconazole. The maximum number of ADRs experienced by a single patient was eight. The patients with multiple ADRs were distributed as follows: 10 with two ADRs (20%), 10 with three ADRs (20%), 17 with four ADRs (34%), 6 with five ADRs (12%), three with six ADRs (6%), one with seven ADRs (2%) and one with eight ADRs (2%).
Table 1 gives a profile of ADRs associated with the use of antifungals.
Profile of Adverse Drug Reactions Associated with Antifungals use, Identified in 50 Patients.
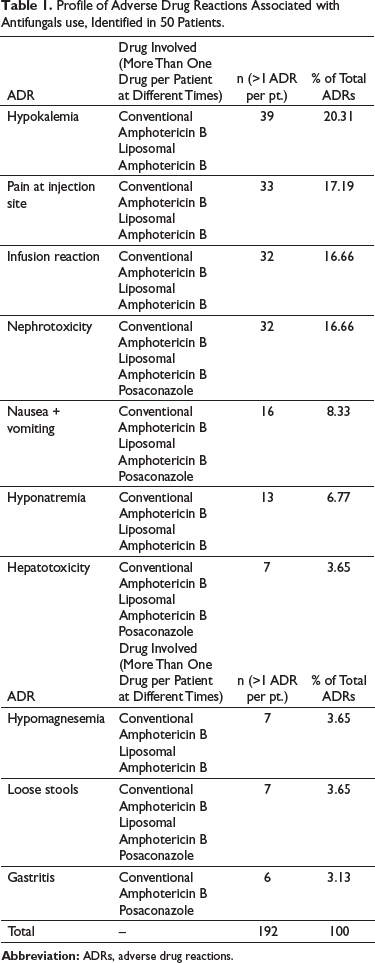
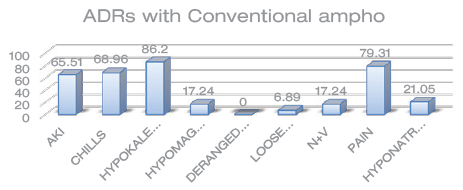
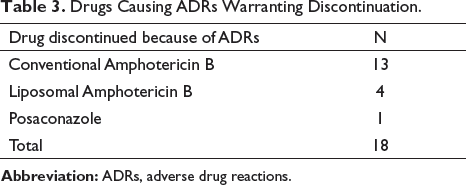
Out of our 50 study subjects, 29 of them experienced ADRs while on Amphotericin B Deoxycholate. It was found to be associated most commonly with hypokalemia (25 out of 29 patients or 86.2%) followed by pain at the injection site (23 out of 29 patients or 79.3%), infusion reactions in the form of chills (20 out of 29 participants), and acute kidney injury (nephrotoxicity; 19 out of 29 participants). In 13 patients, Amphotericin B Deoxycholate was withheld and replaced by liposomal Amphotericin, while 16 patients were continued on the same dose of Amphotericin B.
Potassium supplementation was given prophylactically to all patients receiving Amphotericin B and Liposomal Amphotericin B But the dose and frequency of the same had to be stepped up in all patients experiencing hypokalemia despite routine supplementation. A statistically significant association was found between the incidence of AKI and sex for Amphotericin B Deoxycholate (p = 0.013) with a male preponderance. Other ADRs experienced are given in Figure 1.
ADRs as a Percentage of Patients Who Received Conventional Amphotericin B.
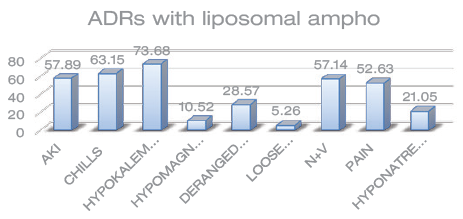
Out of our 50 study subjects, 19 of them experienced ADRs while on Liposomal Amphotericin B. Liposomal Amphotericin B was found to be associated most commonly with hypokalemia (14 out of 19 patients or 73.68%) followed by pain at the injection site (10 out of 19 patients or 52.6%), infusion reactions in the form of chills (12 out of 19 participants) and acute kidney injury (nephrotoxicity) (11 out of 19 participants). In four patients, Liposomal Amphotericin B was withheld and replaced by Posaconazole, while 15 patients were continued on the same. Other ADRs experienced are given in Figure 2.
ADRs as a Percentage of Patients Who Received Liposomal Amphotericin B.
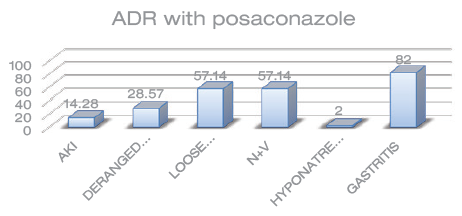
Posaconazole was associated with the least number of ADRs, observed only in seven patients, with gastritis being the most common (six out of seven patients or 82%) followed by nausea and vomiting, and loose stools (57.14% each). Deranged LFTs were found in only 28.57% (two out of seven patients) of participants. The drug was withdrawn in one patient because of deranged LFTs and the dosage was reduced in the other patient for the same reason after consultation with the gastroenterologist. Other ADRs are given in Figure 3.
ADRs as a Percentage of Patients Who Received Posaconazole.
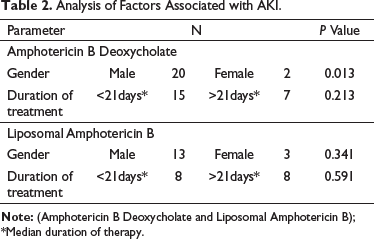
Chi-square tests for association between hypertension and AKI revealed a P-value of 0.148 while the duration of antifungal use with ADRs showed a P-value of 0.213 and 0.591 for Amphotericin B Deoxycholate, and Liposomal Amphotericin B respectively. No statistically significant difference was found between mean creatinine values and age was not found to be associated with an increase in the incidences of AKI in any of the two groups, namely Amphotericin B Deoxycholate and Liposomal Amphotericin B administered groups (p = 0.491) (Table 2).
Analysis of Factors Associated with AKI.
ADRs resulting in discontinuation of the drugs under study are represented in Table 3.
Drugs Causing ADRs Warranting Discontinuation.
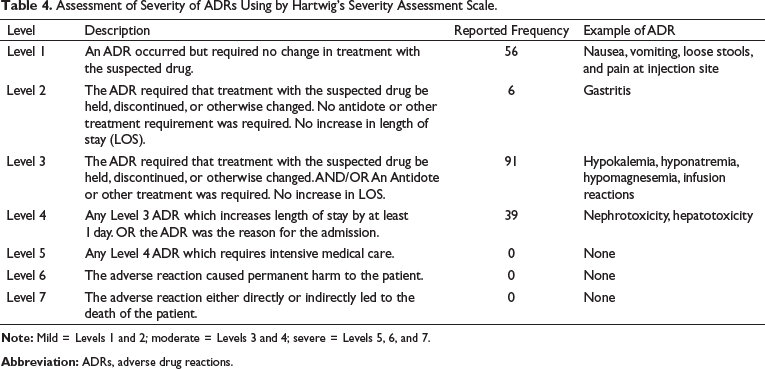
As per Hartwig’s Severity Assessment Scale, 32.3% (62/192) ADRs were mild, 67.7% (130/192) were moderate and none were severe. Details of the same are given in Table 4.
Assessment of Severity of ADRs Using by Hartwig’s Severity Assessment Scale.
Discussion
National and international research on ADRs of antifungals in hospitals are scarce and are restricted to oncology and hematology settings and hematopoietic stem cell transplant units. 16 The ADR profile under study is based on current knowledge about the safety of antifungal agents and the prevalence of adverse reactions related to Amphotericin B Deoxycholate, Liposomal Amphotericin B, and Posaconazole. 19
Electrolyte abnormalities, most notably hypokalemia, were the single most common ADR observed, occurring in 80% to 85% of study subjects. However, the routine supplementation given to our patients resulted in only six instances of severe hypokalemia (serum potassium < 2.5mEq/L) out of a total of 39 instances of hypokalemia. Hypomagnesemia (serum magnesium <1.3mEq/L), while less common, accounted for an overall 14% and may have been a contributing factor for hypokalemia.
Pain at the injection site was the second most common ADR in this study accounting for 33 out of 50 patients (17.19%) closely followed by infusion reactions in 32 out of 50 patients (68.96% with Amphotericin B Deoxycholate and 63.15% with Liposomal Amphotericin B), as opposed to being the most common ADR in other studies.16, 17–19 A possible explanation for the same could be that all patients in our study were premedicated with Hydrocortisone and Pheniramine before Amphotericin administration resulting in a decrease in its incidence.
Nephrotoxicity is a factor limiting the use of Amphotericin B, which is associated with substantial morbidity, mortality, and elevated health care costs.13, 14, 16–20 During the infusion of Amphotericin B, there is vasoconstriction of the renal afferent arterioles, resulting in a decrease in the renal blood flow and the glomerular filtration rate. Kidney cells are highly exposed to Amphotericin B, which explains the high nephrotoxicity of this drug. The high costs of lipid formulations limit access to these drugs, which are generally used as a treatment option for patients with nephrotoxicity resulting from the use of Amphotericin B Deoxycholate or previous renal dysfunction. 21 However, it is possible that the renal safety of this drug could be overestimated, as this study observed only a modest difference when compared to conventional Amphotericin B. Further studies will be needed to better demonstrate the comparable renal safety profile of both drugs.
Hepatotoxicity was seen primarily with Posaconazole and Liposomal Amphotericin B in the form of transaminitis. Posaconazole-related hepatotoxicity was easily countered by dose reduction. While mildly hepatotoxic, Posaconazole has a better liver safety profile when compared to other triazoles. 22
A statistically significant association between AKI and sex was found in the Amphotericin B Deoxycholate group with a male preponderance, however, this data may be skewed as study participants were predominantly male. Duration of treatment was not found to have increased the incidence of AKI, with AKI occurring more frequently and early (within 21 days) in the treatment course for both Amphotericin B Deoxycholate and Liposomal Amphotericin B (Table 2).
Strategies for ADR prevention in patients using antifungals include multidisciplinary actions to optimize their use. Stewardship programs are necessary for the rational use of antifungals and patient safety, in addition to reducing drug resistance and improving the control of health care-associated infections. The definition of treatment protocols based on scientific evidence is also an impact strategy that contributes to reduced costs.23–25 Evidence-based clinical guidelines are essential for the incorporation of therapeutic drug monitoring into clinical practice. 18
The design of this study was a hindrance in demonstrating causal relationships between the associated factors and ADR occurrence. Because of the national shortage of antifungal agents, 8 a steady stream of supply was never available and patients received these antifungals as per their availability, which resulted in drug-free intervals between consignments. This may have led to an underestimation of the extent of ADRs that patients would have experienced were they to have gotten a continuous supply. The study was conducted at a single center, which restricts the generalizability of the results.
The above findings contribute to the understanding of the factors associated with the occurrence of ADRs caused by antifungals and to the promotion of safe and rational antifungal use.
Conclusion
Amphotericin B Deoxycholate was associated most frequently with ADRs, hypokalemia, pain at the site of injection, and infusion reactions being the most frequent. However, concerning nephrotoxicity, it is closely followed by Liposomal Amphotericin B, showing an insignificant difference in the safety profile of Amphotericin B Deoxycholate versus the more expensive Liposomal Amphotericin B. This should be considered before prescribing Liposomal Amphotericin B to patients to avoid nephrotoxicity. Infusion reactions can be significantly reduced with the preadministration of hydrocortisone and pheniramine. Hypertension is not associated with an increase in the incidence of ADRs, nor is the duration of antifungal therapy. Posaconazole is associated with the least number of ADRs and has a favorable safety profile.
Studies involving larger populations will be required to better elucidate the less frequent ADRs. Randomized control trials will be required to establish guidelines regarding the duration of therapy with antifungals which, are currently, ill-defined.
Footnotes
Acknowledgment
We are thankful to all those people who are directly or indirectly responsible for the completion of this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.