
Abstract
Objective:
To compare the prophylactic antiemetic efficacy of ondansetron monotherapy with that of the combination of ondansetron and dexamethasone in the prevention on postoperative nausea and vomiting (PONV) in breast surgeries by observing the incidence of PONV, assess the percentage of participants requiring rescue antiemetics, know the side effects of drugs, and analyze the effect of the surgical duration of breast surgeries.
Methods:
The group ondansetron (O) received 0.1 mg/kg IV ondansetron and the other group (ondansetron and dexamethasone combination, OD) received 0.1 mg/kg IV ondansetron and 0.1 mg/kg of dexamethasone. The incidence of PONV in the first 24 h, percentage of population receiving rescue antiemetics, surgical duration, and hemodynamic parameters were noted.
Results:
In the 0 h to 6 h postoperative period, 38.9% of participants of group O had PONV, whereas only 13.9% in group OD had PONV, which was statistically significant (P < .016). About 30.6% of study population in group O and 8.3% in group OD required rescue antiemetics which was statistically significant (P = .017). Surgical duration of more than 120 min had a statistically significant higher incidence of PONV in the O group with a P-value of .048.
Conclusion:
The combination of prophylactic ondansetron with dexamethasone is more efficacious than ondansetron alone for the prevention of PONV in women undergoing breast surgeries.
Introduction
The term postoperative nausea and vomiting (PONV) is typically used to describe nausea and/or vomiting or retching in the first 24 h postoperatively. 1 As a patient-specific concern, it has been reported to increase patient dissatisfaction and postoperative pain thus prolonging the stay in hospital. 2 The incidence of PONV is found to be 20% to 30% in postoperative patients and it increases with high-risk surgeries. 3
Diseases of breast is a global health problem. Surgery is one of the options for the treatment of breast cancers, some benign breast diseases, and cosmetic breast reconstruction. Certain studies have reported that about 47% to 80% of patients undergoing minor breast surgery, mastectomy, and breast reconstruction suffer from PONV. 4 Ambulatory daycare breast surgeries are on the rise and PONV among these women increases the concerns of unanticipated readmissions. The goal of finding appropriate prophylactic antiemetic therapy to prevent PONV in these surgeries becomes prerequisite to reduce its incidence, patient-related distress, and health care costs. 5
Untreated severe PONV can result in dehydration, electrolyte imbalance, wound dehiscence, interference with early nutrition, and very rarely esophageal rupture or aspiration pneumonitis, and delay in achieving discharge criteria.3, 5 Serotonin antagonists, steroids, prokinetics, and combinations of these drugs are used for prophylaxis and treatment of PONV. Various studies are conducted to find the best combination of these drugs to prevent it but we found limited studies in the literature about the prevention of PONV in breast surgeries.
Hence, in our study, we compared the efficacy of prophylactic ondansetron alone with the combination of ondansetron and dexamethasone in the prevention of PONV in breast surgeries. Both these drugs are commonly used, economical and have less frequent side effects. We hypothesized that breast surgeries whether benign or malignant can have significant PONV and it requires a combination of dexamethasone with 5 hydroxytryptamine 3 (5HT3) receptor antagonists for prevention.
In our study, we primarily examine the antiemetic efficacy of prophylactic ondansetron as a single drug versus its combination with dexamethasone in breast surgeries by observing the incidence on PONV. Secondary objectives were to assess the percentage of participants requiring the rescue antiemetics, side effects of drugs, and to analyze the effect of surgical duration of breast surgeries in both groups.
Methods
The study was a double-blind randomized controlled trial carried out at a tertiary health care center after getting approval from the Institutional ethics committee dated 03/26/2019 fromMay 2019 to December 2019. This study adheres to the applicable consolidated standard of reporting trials (CONSORT) guidelines (Figure 1) with CTRI/2019/05/019171.
CONSORT Diagram.

Sample Size
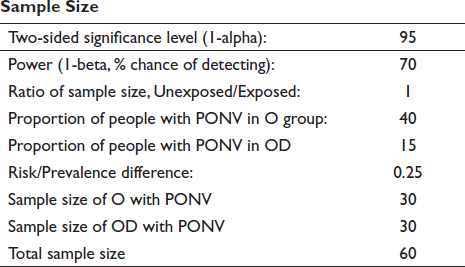
Recruitment was conducted from female patients aged between 20 yr to 70 yr belonging to the American society of Anesthesiologist (ASA) Grade 1 or 2 undergoing breast surgeries (benign, malignant, or reconstruction) under general anesthesia. They were included in the study after obtaining written informed consent. Patients on chronic steroid therapy, pregnant/lactating women, patients with a history of motion sickness, patients on preoperative chemotherapy, patients who received anti-emetics/steroids within 24 h of surgery, patients with uncontrolled diabetes mellitus, intestinal obstruction, hiatus hernia, hepatic and renal diseases, and patients with QT prolongation in ECG were excluded from the study.
The participant and the observer were blinded. A designated consultant from the anesthesia team, not involved in the study, loaded the drugs in two identical 5 mL syringes and placed in sealed envelopes. Measurement was done according to computer-generated block randomization. The drugs were diluted with normal saline to make up a volume of 5 mL in each syringe. In the ondansetron group, the second syringe had only normal saline. Both syringes were labeled as “clinical study drugs.”
Standardized anesthesia protocol was followed. Nil per oral guidelines was observed. Premedication with tablet Ranitidine 150 mg was given and antiemetic was avoided. Intravenous (IV) line 18/20 G was secured and IV fluid Ringer Lactate 500 mL was started. Standard ASA monitoring was done with noninvasive blood pressure, pulse oximeter, electrocardiogram, capnography, and skin temperature probe.
After preoxygenation, IV fentanyl 2 µg/kg was given followed by the study drug based on randomization. Participants in group O received 0.1 mg/kg IV ondansetron and participants in group OD received 0.1 mg/kg IV ondansetron and 0.1 mg/kg of dexamethasone. Both drugs were given during induction of anesthesia to standardize blinding and as most breast surgeries were anticipated for a total duration of 3 h to 4 h. Induction of anesthesia was done with IV propofol 2 mg/kg and tracheal intubation was facilitated with 0.5 mg/kg of atracurium. Anesthesia was maintained with air: oxygen (50:50) and isoflurane to maintain minimum alveolar concentration 1 and titrated doses of atracurium. Additional analgesics, IV morphine 0.1 mg/kg and acetaminophen 15 mg/kg were given intraoperatively. Postoperatively all patients were given IV acetaminophen 15 mg/kg every 6 h. Patients were extubated after surgery and vitals were monitored during the postoperative period.
All nurses in Post Anesthesia Care Unit and wards were educated regarding the assessment of PONV scores and administration of rescue antiemetics and were instructed to alert the primary investigator for any further information. The study instrument was the patient pro forma which had details of the patient’s age, weight, heart rate, and blood pressure measured every 5 min during surgery. PONV score was evaluated on a four-point scale: 0 = None, 1 = Nausea, 2 = Nausea with Retching, 3 = Vomiting. 7
All cases were followed up postoperatively at three intervals of 0 h to 6 h, 6 h to 12 h, and 12 h to 24 h for PONV. Rescue antiemetics were given when nausea did not subside for 15 min or the patients had a PONV score of 2 or 3 and it consisted of IV O 0.05 mg/kg initially and was followed by IV metoclopramide 0.15 mg/kg if there was no improvement.
The primary outcome of antiemetic efficacy was measured by the incidence of PONV in both groups. Secondary objectives were analyzed by the percentage of patients requiring anti-emetics, any side effects, and effect of surgical duration of breast surgeries in each group on PONV.
The data were entered in Microsoft Excel (2013). Statistical analysis was done using Statistical Package for social sciences software version 16. Descriptive statistics for all the demographics will be represented as Mean +/- standard deviation if continuous variable, number, and percentages if categorical variable. The proportion of participants with PONV was compared between the two groups using the Chi-square test. The continuous variable was compared between the groups using an independent t-test. A P-value of < .05 was considered statistically significant.
Results
Demographic profile in relation to the mean age (years) of subjects in group O was 43.53 ± 15.57 and in group OD was 48.61 ± 14.77 and the mean weight (kg) of the patients was 65.33 ± 11.50 in the O group and 63.16 ± 11.76 in the OD group. The age and weight of patients in both groups were not statistically significant (Table 1). Baseline hemodynamic parameters were statistically insignificant in both groups.
Demographic Profile of Study Groups

It was observed that the incidence of PONV was 38.9% (14/36) in and 13.9% (5/36) in OD within 6 h postsurgery which was statistically significant (P < .016). The PONV at 6 h to 12 h postsurgery in O group was 11.1% (4/36) as against 2.8% (1/36) in the OD. Even though the incidence of PONV was greater in the O group it was not statistically significant (P < .179; Table 2). The PONV scores at 12 h to 24 h were zero in both the groups. Distribution of PONV scores in each group is given in (Table 3), (Table 4). The percentage of patients requiring rescue antiemetic’s in group O was 30.6% (11/36) and in the case of group OD was 8.3% (3/36) which was statistically significant (P < .017; Table 5).
Incidence of PONV

PONV Scores at 0 h to 6 h

PONV Scores at 6 h to 12h

Percentage of Study Group Requiring Rescue Antiemetics

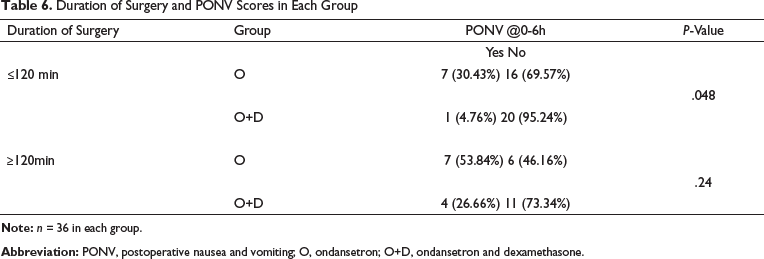
The number of patients who had nausea and vomiting in the 0 h to 6 h postoperative period with surgical duration <120 min was statistically significant with a P-value of .048 with higher incidence in O group. PONV incidence in relation to surgical duration of more than 120 min in both groups postoperative was statistically not significant with a P-value (.24; Table 6).
Duration of Surgery and PONV Scores in Each Group
There were no adverse events in either group.
Discussion
PONV has remained a major concern following the recovery of patients from anesthesia. There has been a steady increase in the number of breast surgeries, which can be attributed to the increase in the awareness of benign breast diseases and carcinomas with increased diagnostic modality. Breast surgeries in female patients are one of the unexplored causes of PONV. Apfel scoring considers four risk factors: female gender, nonsmoking status, previous history of PONV and use of postoperative opioids. Risk of PONV increases with the presence of more than one factor. 8 The literature available on the incidence and prevention of PONV in breast surgeries is scarce.
Breast cancer is the most common cancer in women in India and accounts for 14% of all cancers in women.9, 10 Literature reveals that about 47% to 80% of patients undergoing the various types of breast surgeries suffer from PONV.4, 11
The primary objective of the study was to compare the efficacy of prophylactic ondansetron 0.1 mg/kg as monotherapy versus a combination therapy of ondansetron 0.1 mg/kg with dexamethasone 0.1 mg/kg in preventing PONV in breast surgeries.
Ondansetron, a selective 5HT3 receptor antagonist, has been proven to be effective in the prevention and treatment of nausea and vomiting and has been in clinical use since 1988. The recommended dose is 0.1 mg/kg to 0.15 mg/kg and effective blood levels are attained 30 min to 60 min after administration. The elimination half-life of O is approximately 3.5 h to 4 h in adults. 12 Failure rates are seen with ondansetron monotherapy thus guidelines suggest a multimodal/risk-based approach to be followed.
Multicenter studies have demonstrated that intravenously administered O 4 mg is effective in preventing and treating PONV. This is confirmed in the 2014 consensus guidelines in the management of PONV by Gan et al. 8 Although 4 mg of O is proven to prevent PONV when given at the end of the surgery, we opted to give 0.1 mg/kg of O to be given at induction of anesthesia, to standardize the administration of drugs. 12
De Oliveira et al. 13 compared two doses of 0.1 mg/kg and 0.05 mg/kg of dexamethasone and showed that with a higher dose there was a lesser requirement of opioids, decreased incidence of nausea, and muscle pain and thereby decreasing the time for discharge readiness. Most of the available literature suggests the use of a single dose of dexamethasone in the perioperative period as this does not seem to increase the risks of wound infection.14, 15 An editorial published in 2013 has suggested that a single 4 mg to 8 mg dose of Dexamethasone was considered safe after considering the risks as well as the benefits. 15 Dexamethasone is known to increase blood sugar levels 16 but it reduces the need for rescue antiemetics and also provides analgesia, allows better ambulation, and reduces hospital stay without many adverse outcomes.17, 18 Respiratory function tests were better in patients who received dexamethasone and were undergoing breast conservation surgeries. 18 The exact mechanism of action is not known but it is thought to inhibit central/peripheral production of 5HT and by inhibition of synthesis of prostaglandins. 12
The demographic and hemodynamic parameters between the two groups such as age, weight, heart rate, systolic, and diastolic blood pressure were comparable.
The combination of O with Dexamethasone was used in our study based on dexamethasone reduces emesis after major gastrointestinal surgery (DREAMS) trials which highlighted the use of dexamethasone for the management of PONV. 19 Fifty-three trials studied proved the efficacy of O in reducing PONV was 20% at best. Therefore, although O is the treating drug of choice newer drugs or combined therapy with other drugs needs exploration.
Drugs were given prophylactically with 0.1 mg/kg of Dexamethasone and 0.1 mg/kg of O before induction of anesthesia in our study. The onset time of dexamethasone is 2 h and most of the patients experience PONV at 0 h to 2 h after the surgery and the mean duration of surgeries in our study was around 2 h.
The assessment of PONV was done at defined periods such as 0 h to 6 h, 6 h to 12 h, and 12 h to 24 h. During the first 6 h the incidence of PONV in the O group was 38.9% and in the OD group was 13.9% which was statistically significant with a P-value of <.016. We observed that a higher incidence of PONV was in this initial 6 h of the postoperative period, as there was no significant difference seen in both groups in postoperative period after 6 h. The risk of PONV decreased in the 12 h to 24 h period.
Our results were comparable with the study conducted by Souvik Maitra et al. who concluded in their study that the incidence of PONV at 4 h to 6 h was significantly lower when dexamethasone was used instead of ondansetron and that incidence of nausea is similar at 24 h. 20 Adding dexamethasone as a second antiemetic can aid recovery from anesthesia with its antiemetic efficacy.
Khalid Ahsan et al. found that patients receiving ondansetron alone had an incidence of PONV of 28% as compared to patients receiving ondansetron and dexamethasone where the incidence of PONV was 12% which was statistically significant with a P-value of <.046. 21 Thomas and N Jones also found that a combination of dexamethasone and ondansetron was more efficacious as prophylaxis for PONV. 22 Combination therapy with dexamethasone was proved effective to reduce PONV even in patients receiving neuraxial anesthesia. 23 Chiu C et al. observed that within patients undergoing total mastectomy, the incidence of PONV was reduced with enhanced recovery after surgery pathway which incorporated ondansetron, dexamethasone, and regional nerve blocks. 24
Dexamethasone monotherapy was found ineffective against PONV by Chatterjee et al. in patients undergoing laparoscopic cholecystectomies. 25
None of the patients in this study in either group experienced nausea or vomiting from 12 h to 24 h. PONV scores at 6 h to 12 h and 12 h to 24 h were comparable between the two groups. The findings were similar to the study findings of Apfel CC et al. where they observed a higher incidence of PONV in the first 6 h postsurgery. 26
The secondary objective of this study was to assess the percentage of the study population requiring rescue antiemetics. In our study, we found that the percentage of patients requiring rescue antiemetic in the O group was 30.6% and in the OD group was 8.3%, which was statistically significant with a P-value of < .017. This corresponded to the incidence of PONV. The results were comparable to a study conducted by Elhakim et al. who concluded that the need for rescue antiemetic was less in OD group compared to the placebo group and Ogroup. 27
We observed that the incidence of PONV at 0 h to 6 h in breast surgeries with duration <120 min, the O group had statistically significant numbers in comparison to the OD group with a P-value of .048. Whereas, there was no statistically significant difference between both groups in surgeries with the duration of >120 min. With an increase in the duration of the surgeries, there was an increase in the incidence of PONV in OD group but it remained the same in O group. These results are in accordance with the study conducted by Chatterjee et al. 28 Surgeries lasting more than one-hour duration are considered an additional risk factor for PONV. 29
No adverse events related to the study drug in either of the groups were observed.
Our study included female patients undergoing all types of breast surgeries and was not restricted to major surgeries. So, this could have resulted in unequal distribution of cases in relation to surgical duration. However, this was unavoidable in view of randomization. Both groups received drugs at maximal recommended dosages based on body weight and were administered preemptively before the surgical stimulation.
There were certain other limitations of our study. We did not include dexamethasone monotherapy as a separate group, which could have added insight to the study. Administration of ondansetron at the end of surgery could have affected the incidence of PONV at 0 h to 6 h. Measuring blood sugars and duration of analgesia and analgesic requirements could have further supported the proven benefits of dexamethasone.
Conclusion
The female population undergoing breast surgery irrespective of primary disease are prone to PONV and appropriate prophylaxis for prevention of PONV is essential. We concluded that combination therapy with ondansetron and dexamethasone is more efficacious in preventing PONV following breast surgeries, especially in the first six hours of the postoperative period. Additionally, we found that the duration of breast surgery can significantly increase the incidence of PONV despite the dual antiemetic combination.
Footnotes
Acknowledgment
We thank the departments of surgery and community health department for their support in doing this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.