
Abstract
Objective:
To assess the patterns and predictors of pharmacotherapy and QOL in DFS patients in an Indian tertiary care hospital.
Methods:
A cross-sectional study was conducted among inpatients with DFS. Data on sociodemographic and clinical factors, pharmacotherapy, clinical outcomes, and QOL were analyzed using the chi-squared test, independent sample t-test, and binary logistic regression.
Results:
We screened 3284 inpatients and included consecutive 87 (2.7%) DFS patients. The mean age was 56.08 ± 11.05 years, with a male preponderance (75.8%). Mean HbA1c was 9.9 ± 2.483. About 75% of patients received insulin, and polypharmacy was noticed in 82.7%. About 67.8% of DFS patients had other vascular complications of diabetes, with diabetic retinopathy being the most common in 89%. Amputations were noticed in 32.1% of patients. Overall, poor QOL was seen in 79.3% of patients. The mean scores for different domains were as follows: physical, 41.51 ± 14.15; psychological, 42.90 ± 11.16; social relationships, 43.06 ± 19.36; and environment, 47.17 ± 13. The presence of complications from diabetes was a significant predictor of the utilization of antihypertensives (OR: 2.92, CI [1.09, 7.79], P = 0.03) and poor QOL (OR: 4.54, CI [0.965, 21.41], P = 0.05).
Conclusion:
DFS patients in this study were found to be younger with poor glycemic control and other vascular complications of diabetes. The presence of other complications of diabetes in DFS patients was found to be a predictor of pharmacotherapy and poor QOL.
Introduction
Diabetic foot syndrome (DFS) is a serious and economically demanding complication of type 2 diabetes mellitus (type 2 DM). 1 The proportion of hospitalized patients affected with DFS is around 7% of the global inpatient population. 2 Patients who have type 2 DM are 15 times more likely to undergo amputations, and about 85% of nontraumatic amputations are because of DM.3, 4 Hypertension (35%), visual problems (62%), and ischemic heart disease (7%) were the common comorbidities reported in DFS patients. 5
Pharmacotherapy plays an important role to prevent amputations, microvascular, and macrovascular complications. It commonly includes glycemic control, antimicrobial therapy, control of hypertension, dyslipidemia, atherosclerotic heart disease, obesity, and renal insufficiency. 6
DFS patients were reported to have an overall poorer quality of life (QOL) than the population norm.7, 8 Diabetic foot ulcers affect patients emotionally, physically, and economically. DFS can result in lower mobility, increased falls, higher dependence on others, loss of employment, lower income, higher risk of amputation, repeated medical check-ups, and higher living costs. 9
DFS is a highly preventable complication of type 2 DM. A comprehensive study on the characteristics of the disease, risk factors to develop further complications, predictors of pharmacotherapy, and QOL among these patients can suggest interventions for better patient care and patient well-being. The objectives of this study were to assess the patterns and predictors of pharmacotherapy and QOL of patients with DFS.
Materials and Methods
Study Design: Prospective Cross-Sectional Study
Setting: All adult consenting consecutive inpatients with DFS admitted under the endocrinology and surgical departments in St John’s Medical College Hospital, Bangalore, from March 2017 to March 2018 were screened after obtaining written informed consent (IEC No. 46/2017). The unconscious, terminally ill, and daycare patients were excluded.
Sample Size: According to literature, the proportion of inpatients affected with type-2-DM-related foot disease is around 7% of the population. Taking the proportion as 7% and assuming a precision of 5% and 90% CI, the sample size is estimated to be 72. With missing data estimated to be 20%, the estimated total sample size was 87. 2
Data Collection Instrument: The designed case record form was a self-administered-/interviewer-assisted type divided into two sections. The first section included the patients’ sociodemographic information, clinical profiles, complications, and drug data. The second section was the World Health Organization (WHO)-BREF questionnaire. The WHO-BREF questionnaire consists of 26 items: First, two items evaluate the overall QOL and satisfaction with health with poor QOL defined as those with two or less points on the individual’s overall QOL item 10 ; the rest of the 24 items were clustered into 5 domains (physical health, perception/psychological, social relations, and environment).
Statistical Analysis
Clinical Characteristics: Analyzed using descriptive statistics.
Patterns and Predictors of Pharmacotherapy: Patterns of drug distribution were described using percentages. Factors affecting pharmacotherapy of five relevant (most used among our study participants) drug classes, i.e., insulin, antihypertensives, antiplatelets, statins, and antibiotics, were analyzed.
Predictors of QOL: The QOL data were analyzed using mean, which were then compared with the population norm. Factors affecting the overall perceived QOL were assessed by grouping the study participants into those with good QOL and poor QOL as per the first two items’ scores as mentioned earlier.
Data were analyzed using chi-squared tests and independent sample t-test. Binary logistic regression was done with variables found significant in the univariate analysis. A P value < 0.05 was considered significant for all tests. Statistical analysis was performed using the commercially available SPSS Version 25.0 (IBM Corp. 2017. Armonk, NY).
Results
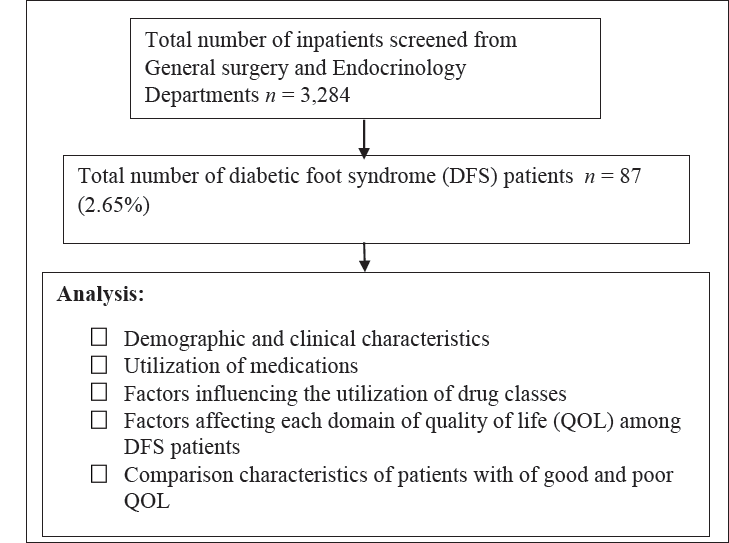
We screened 3284 consecutive hospitalized patients during the study period and included 87 (2.7%) patients with DFS. The data flow of study population is depicted in Figure 1.
Data Flow and Analysis of the Study Population.
Demographic and Clinical Characteristics
The mean age of the population was 56.08 ± 11.05 years. Sixty six (76%) patients were male. The mean HbA1C was 9.9 ± 2.483. The median of serum creatinine was 0.93 (IQR: 0.43–2.81). The median/IQR for cholesterol, LDL, and TG was 141 (IQR: 115–225), 85 (IQR: 43–223), and 210 (IQR: 82–298), respectively. Hypertension was prevalent in 26 (30%).
Complications of type 2 DM other than DFS were seen in 59 (67.8%) patients, and the most prevalent complication was diabetic retinopathy (DR; 89.6%).
Patterns and Predictors of Pharmacotherapy
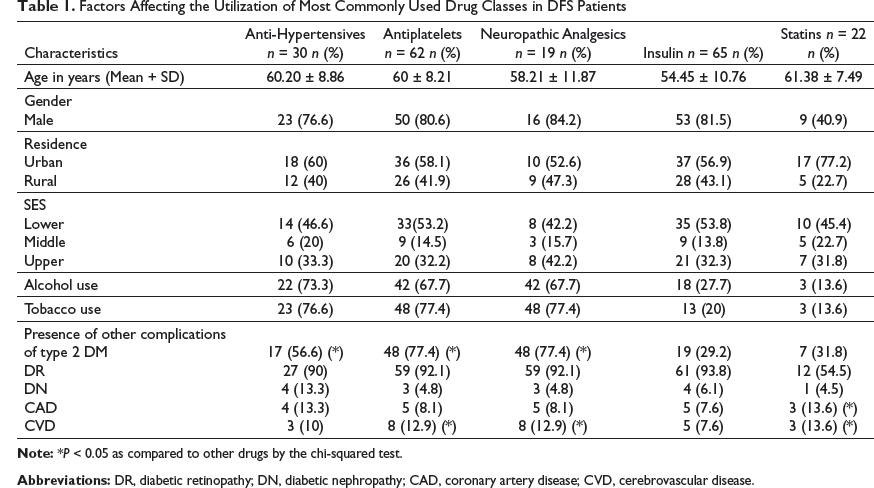
The mean number of drugs utilized per patient was 6.62 ± 2.01. Polypharmacy (>5 drugs) was noted in 82.7%. Insulin was the most commonly prescribed drug—65 (74.7%). Antihypertensives were prescribed in 30 (34.4%), with angiotensin converting enzyme (ACE) inhibitors or angiotensin receptor blocker (ARBs) in 11 (12.6%), statins in 17 (19.5%), neuropathic analgesics in 19 (21.8%), oral hypoglycemic drugs (OHAs) in 15 (17.2%), and antibiotics in 62 (71.2%).
Factors Affecting the Utilization of Most Commonly Used Drug Classes in DFS Patients
Quality of Life
QOL was analyzed using the WHO-BREFQOL scoring system. The mean scores for different domains adjusted to 100 were as follows: physical, 41.51 ± 14.15; perception, 42.90 ± 11.16; social relationship, 43.06 ± 19.36; and environment, 47.17 ± 13.45.
Factors Affecting Different Domains of QOL (WHO-BREF) in DFS Patients (n = 87)
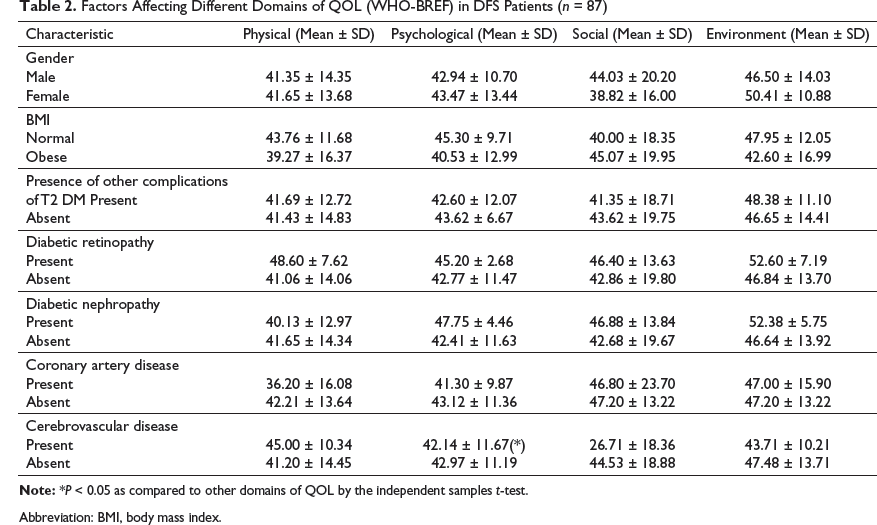
Abbreviation: BMI, body mass index.
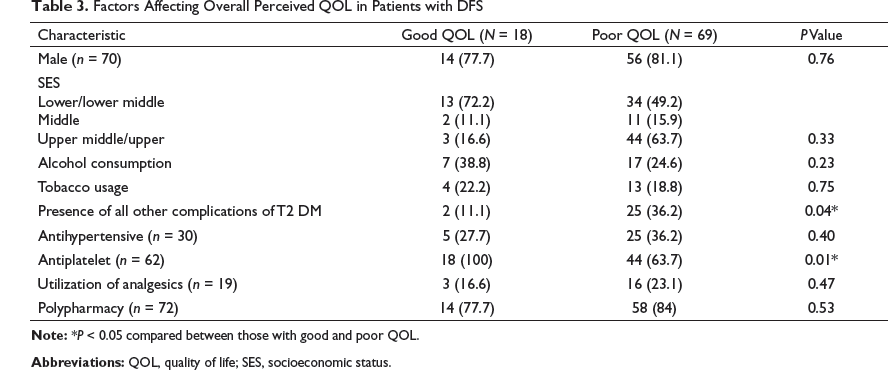
Factors Affecting Overall Perceived QOL in Patients with DFS
Amputations were seen in 28 (32.1%). Twenty seven were distal amputations–disarticulations/transmetatarsal amputations, and one was a below knee amputation.
Discussion
In this study, we assessed the demographic and clinical characteristics, patterns and predictors of pharmacotherapy, and predictors of QOL among patients admitted with DFS.
A male preponderance was noticed in the study that correlates with that observed in similar studies conducted in India and abroad.5, 7, 11 Age of the patients in our study correlated with previous studies from India. 5 This highlights the need for screening and primary prevention of type 2 DM and its complications among adult Indians at the earliest.
Majority of the participants had been diagnosed with type 2 DM for more than 10 years, which was similar to previous studies.10, 11, 12 The mean HbA1C was 9.851 ± 2.483. This finding indicated poor glycemic control among DFS patients and the need for more awareness among these patients.
Our data showed that about 68% of patients had complications of type 2 DM other than DFS, with DR being the most common complication. Although this was similar to another study from India, it was higher than that seen in similar European studies.5, 7 A high incidence of other vascular complications in type 2 DM was noticed in previous studies as well. 13
The average number of drugs was 6.62 ± 2.01, and polypharmacy was seen in about 82.7%. A previous study demonstrated that type 2 DM had a high prevalence of polypharmacy with evidence-based guidelines influencing polypharmacy. 14 The most common drug used was insulin, which was correlated with previous studies. Antiplatelets, antihypertensives, neuropathic analgesics, and statins were the other commonly used drug classes. Our data showed underutilization of statins in the study population, which was similar to previous studies. The dismal usage has been attributed in prior studies to the increased cost of the drug and poor follow-up. 15
Our data also showed that DFS patients with the presence of coronary artery disease and CVD had higher utilization of antiplatelets and statins. Antiplatelets and antihypertensives are usually prescribed for secondary prevention of cardiovascular disease among those with vascular complications. 13
Our study showed the presence of amputation in 32.1% of DFS patients. This was consistent with the previous studies. 16
Our study also revealed a poor QOL in all four domains of the WHO-BREFQOL scoring system, with the lowest in the domain of physical health: 41.51 ± 14.15 (population norm, 55.17 ± 12.50). 17 The presence of CVD was associated with poor psychological or perceptional QOL. Previous studies have demonstrated increased all-cause mortality among patients with depression or poor mental health and stroke (adjusted HR, 1.93; 95% CI [1.28, 2.92]), highlighting the need to take appropriate steps to detect and manage the poor psychological QOL in these high-risk patients. 18
A majority had a poor overall perceived QOL. The presence of complications was a predictor of poor overall QOL. A previous study by Mousab Al Ayed et al. alluded this to longer periods of hospitalization and overall morbidity. 19
This study provides valuable insight into the pharmacotherapy, associated complications, QOL, and outcome of patients with DFS in India. The presence of vascular complications of type 2 diabetes was found to influence pharmacotherapy and QOL in patients with DFS.
Conclusion
DFS patients had poor glycemic control, other complications of diabetes, and poor QOL. The presence of other complications of diabetes is found to be a predictor of pharmacotherapy and poor QOL. The earlier age of onset of DFS suggests the need for increased awareness and screening for complications among young adults. A poor psychological QOL suggests a need for psychological support.
Footnotes
Acknowledgment
The authors would like to thank Dr Subramaniyam, Professor and Head of General Surgery, and Mrs Sumithra, Biostatistician, for their help.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.