
Abstract
Background:
Endocrine disorders can produce prominent psychiatric symptoms that may mimic primary psychiatric illnesses. When psychiatric manifestations dominate the clinical picture, the underlying endocrine pathology may remain unrecognised, leading to delayed diagnosis and inappropriate treatment. Early identification of hormonal abnormalities is therefore critical in atypical psychiatric presentations.
Methods:
We present a case series of four patients who presented primarily with acute psychiatric syndromes but were subsequently diagnosed with distinct endocrine disorders. Psychiatric diagnoses were established according to Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria. Symptom severity was assessed using standardised rating scales, and patients underwent targeted endocrine investigations based on clinical suspicion.
Results:
The cases included hyperthyroidism presenting with psychotic mania, primary hyperparathyroidism with hypercalcaemia causing acute psychosis, pheochromocytoma mimicking panic disorder and Addison’s disease presenting as severe depressive illness with psychotic features. In all cases, endocrine evaluation revealed the underlying disorder, and targeted endocrine treatment led to marked improvement or complete resolution of psychiatric symptoms. Short-term psychotropic medications were required only in the acute phase.
Conclusions:
Endocrine disorders may masquerade as primary psychiatric conditions across multiple endocrine axes. Incorporating basic endocrine screening in atypical, first-episode or rapidly evolving psychiatric presentations can improve diagnostic accuracy, facilitate timely treatment and prevent unnecessary long-term psychotropic use.
Keywords
Introduction
Endocrine disorders are well recognised for their systemic manifestations, yet their psychiatric presentations are often underappreciated in routine clinical practice. Hormonal disturbances can significantly influence brain function by altering neurotransmitter synthesis, receptor sensitivity, neuronal excitability and cerebral metabolism. As a result, endocrine abnormalities may manifest with a wide range of psychiatric symptoms, including anxiety, mood disturbances, cognitive changes and even frank psychosis. In some cases, psychiatric symptoms dominate the clinical picture and precede the diagnosis of the underlying endocrine illness, leading to diagnostic confusion and potential delays in appropriate treatment.[1,2]
Among endocrine conditions, thyroid dysfunction has one of the most extensively documented associations with psychiatric symptoms. Hyperthyroidism may present with irritability, insomnia, agitation, mania and occasionally psychosis, while hypothyroidism is commonly linked to depressive symptoms, cognitive slowing and apathy. Similarly, disturbances in calcium metabolism, particularly in primary hyperparathyroidism, may lead to neuropsychiatric manifestations such as fatigue, mood instability, confusion and acute psychosis due to the effects of hypercalcaemia on neuronal excitability.[1,3]
Other endocrine disorders may mimic primary psychiatric syndromes in equally striking ways. Catecholamine-secreting tumours such as pheochromocytomas can present with recurrent episodes of intense anxiety, palpitations, tremors and a sense of impending doom that closely resemble panic disorder. Likewise, adrenal insufficiency may manifest with apathy, depressive symptoms or cognitive impairment, occasionally progressing to severe depressive episodes with psychotic features. In such situations, psychiatric symptoms may be the first clinical clue to an underlying endocrine pathology.[2,4]
Recognising endocrine contributions to psychiatric illness is clinically important because many of these presentations are potentially reversible with targeted medical treatment. Failure to identify the underlying hormonal abnormality may lead to prolonged psychiatric morbidity, inappropriate long-term psychotropic use and delayed definitive management of the endocrine disorder.
The present case series describes four patients with distinct endocrine conditions—hyperthyroidism, primary hyperparathyroidism, pheochromocytoma and Addison’s disease—each presenting primarily with acute psychiatric manifestations diagnosed according to Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria. These cases were retrospectively identified from patients presenting over a 6-month period to the emergency and inpatient services of a tertiary care hospital and were evaluated in the psychiatry outpatient setting, as well as when they were admitted.
Psychiatric diagnoses were made by a qualified psychiatrist based on DSM-5 criteria through detailed clinical interviews; formal structured diagnostic interviews were not used. Diagnoses were reviewed and confirmed by the primary consultant in charge of the patients.
Through these cases, we aim to highlight the diverse psychiatric presentations of endocrine disorders and emphasise the importance of systematic endocrine screening in atypical, first-episode or rapidly evolving psychiatric syndromes.
Case Descriptions
Case 1: Hyperthyroidism Presenting as Psychotic Mania
A 28-year-old woman with no prior psychiatric history was brought to the emergency service with a 1-week history of markedly reduced sleep, pressured speech, irritability, elevated mood and increased goal-directed activity. Family members reported excessive talkativeness, impulsive spending and suspiciousness. Over the preceding 3 days, she also described hearing voices commenting on her actions. No baseline medical comorbidities, prior psychiatric illness or regular medication use were reported. There was no history of substance use or family history of psychiatric disorders.
On physical examination, she appeared restless and hyperactive. Her pulse rate was 110 beats per minute with a fine tremor of the hands and mild lid lag. Mental status examination revealed expansive mood, flight of ideas, grandiose thoughts and second-person auditory hallucinations. The Young Mania Rating Scale (YMRS) score was 32/60, indicating severe mania, while the Brief Psychiatric Rating Scale (BPRS) score was 54/126, suggesting significant psychotic symptom burden. Rating scales such as YMRS and BPRS are widely used for quantifying manic and psychotic symptom severity in clinical research and practice.[5,6] Neurological examination was unremarkable, and no focal deficits were noted.
Routine laboratory evaluation revealed a markedly suppressed thyroid-stimulating hormone (TSH) level (<0.005 mIU/L) with elevated free T4 (3.2 ng/dL) and free T3 (8.4 pg/mL). TSH-receptor antibodies were positive, and thyroid ultrasonography showed diffuse gland enlargement consistent with Graves’ disease, a common autoimmune cause of hyperthyroidism known to produce neuropsychiatric symptoms ranging from anxiety to psychosis.[1]
Based on the DSM-5, the patient met criteria for bipolar and related disorder due to another medical condition, with manic and psychotic features secondary to thyrotoxicosis.[7] She was initiated on carbimazole and propranolol for endocrine stabilisation, along with low-dose haloperidol for short-term behavioural control. Over 3 weeks, her mood symptoms and hallucinations resolved in parallel with improvement in thyroid hormone levels. Antipsychotic medication was tapered and discontinued once euthyroidism was achieved.
Case 2: Primary Hyperparathyroidism with Acute Psychosis
A 54-year-old male school teacher presented with a 2-week history of rapidly progressive behavioural changes characterised by irritability, persecutory delusions and intermittent visual hallucinations. Family members described fluctuating confusion, suspiciousness toward neighbours and episodes of agitation. On further inquiry, he reported recurrent episodes of renal colic during the previous year, though these had not been fully investigated. He had no prior psychiatric history, no known medical comorbidities apart from episodic renal colic and was not on regular medications. There was no history of substance use or family psychiatric illness.
Mental status examination showed paranoid ideation, perceptual disturbances and impaired attention. The Positive and Negative Syndrome Scale (PANSS) scores were: Positive 28, Negative 12 and General Psychopathology 40, indicating a moderate acute psychotic state. PANSS is a widely used clinical scale for assessing symptom severity in psychotic disorders.[8]
Laboratory investigations revealed hypercalcaemia with serum calcium of 12.8 mg/dL and low serum phosphate (2.1 mg/dL). Intact parathyroid hormone (PTH) level was markedly elevated at 168 pg/mL. Neck ultrasonography identified a solitary parathyroid adenoma. Neuroimaging with a brain MRI showed no structural abnormalities. Neurological examination was non-focal, and other metabolic causes of acute psychosis were excluded through routine laboratory screening.
Hypercalcaemia is well known to produce neuropsychiatric symptoms, including confusion, mood changes, cognitive dysfunction and psychosis due to altered neuronal membrane potentials and neurotransmission.[2]
According to DSM-5 diagnostic criteria, the presentation was consistent with psychotic disorder due to another medical condition, specifically hypercalcaemia secondary to primary hyperparathyroidism.[7] The patient received intravenous hydration and bisphosphonate therapy to correct hypercalcaemia and subsequently underwent surgical parathyroidectomy. Psychotic symptoms subsided rapidly within 1 week following normalisation of calcium levels, and antipsychotic medication was discontinued before discharge.
Case 3: Pheochromocytoma Mimicking Panic Disorder
A 38-year-old woman was referred from cardiology for evaluation of recurrent episodes initially diagnosed as panic attacks. For 2 months, she had experienced sudden episodes of palpitations, tremors, sweating and an intense fear of impending death. Each episode lasted approximately 10-15 min and occurred several times per week. During some attacks, home blood pressure recordings exceeded 200/110 mmHg, raising concern for a secondary medical cause. There was no prior psychiatric history, no significant medical comorbidity and no substance use. There was a family history of depressive disorder in the elder sister.
During psychiatric assessment, she described anticipatory anxiety related to these episodes but did not meet criteria for primary panic disorder. Her Hamilton Anxiety Rating Scale (HAM-A) score was 29/56, indicating severe anxiety symptoms. HAM-A is a standard clinician-rated instrument widely used for assessing the severity of anxiety states.[9]
Further investigation revealed markedly elevated 24-h urinary metanephrines (2,300 µg/day) and increased plasma free metanephrine levels. MRI of the abdomen demonstrated a 4.2-cm right adrenal mass, consistent with pheochromocytoma. Neurological examination was normal, and alternative cardiac and metabolic causes were ruled out during prior evaluations.
Catecholamine-secreting tumours can produce paroxysmal sympathetic activation characterised by tachycardia, sweating, tremor and intense fear, which may closely resemble panic attacks.[3]
According to DSM-5, the clinical presentation was classified as anxiety disorder due to another medical condition, secondary to catecholamine excess.[7] The patient was started on alpha-adrenergic blockade with phenoxybenzamine, followed by elective laparoscopic adrenalectomy. Post-surgery, the paroxysmal anxiety episodes resolved completely, and no further panic-like attacks were reported during 3 months of follow-up.
Case 4: Addison’s Disease with Psychotic Depression
A 66-year-old retired clerk presented with a 3-month history of progressive low mood, anhedonia, fatigue and significant weight loss (approximately 6 kg). Family members reported social withdrawal, decreased appetite and pervasive pessimism. Over the preceding 2 weeks, he developed nihilistic delusions, repeatedly stating that he was ‘already dead’ and that his organs had stopped functioning. There was no prior psychiatric illness, no substance use and no family history of mood or psychotic disorders.
On examination, he appeared frail with noticeable hyperpigmentation of the buccal mucosa and palmar creases. Mental status examination showed psychomotor retardation, depressed mood and nihilistic delusions. The 17-item Hamilton Depression Rating Scale (HAM-D) score was 26/52, indicating severe depressive illness. HAM-D remains one of the most widely used instruments for assessing depressive symptom severity in clinical and research settings.[10]
Laboratory evaluation revealed hyponatraemia (128 mmol/L), hyperkalaemia (5.8 mmol/L) and low fasting glucose levels (60 mg/dL). Morning serum cortisol was markedly reduced (2.1 µg/dL), while adrenocorticotropic hormone (ACTH) was elevated at 320 pg/mL. A short Synacthen stimulation test confirmed primary adrenal insufficiency. Neurological examination revealed no focal deficits, and other metabolic or neurological causes of late-onset depression were excluded.
Adrenal insufficiency has been associated with mood disturbances, apathy, cognitive impairment and occasionally severe depression with psychotic features due to disruption of hypothalamic-pituitary-adrenal axis regulation.[4]
Based on DSM-5 criteria, the condition was diagnosed as major depressive disorder with psychotic features due to another medical condition, namely Addison’s disease.[7] The patient was started on oral hydrocortisone replacement therapy, which led to gradual improvement in mood, energy levels and resolution of psychotic symptoms within 3 weeks.
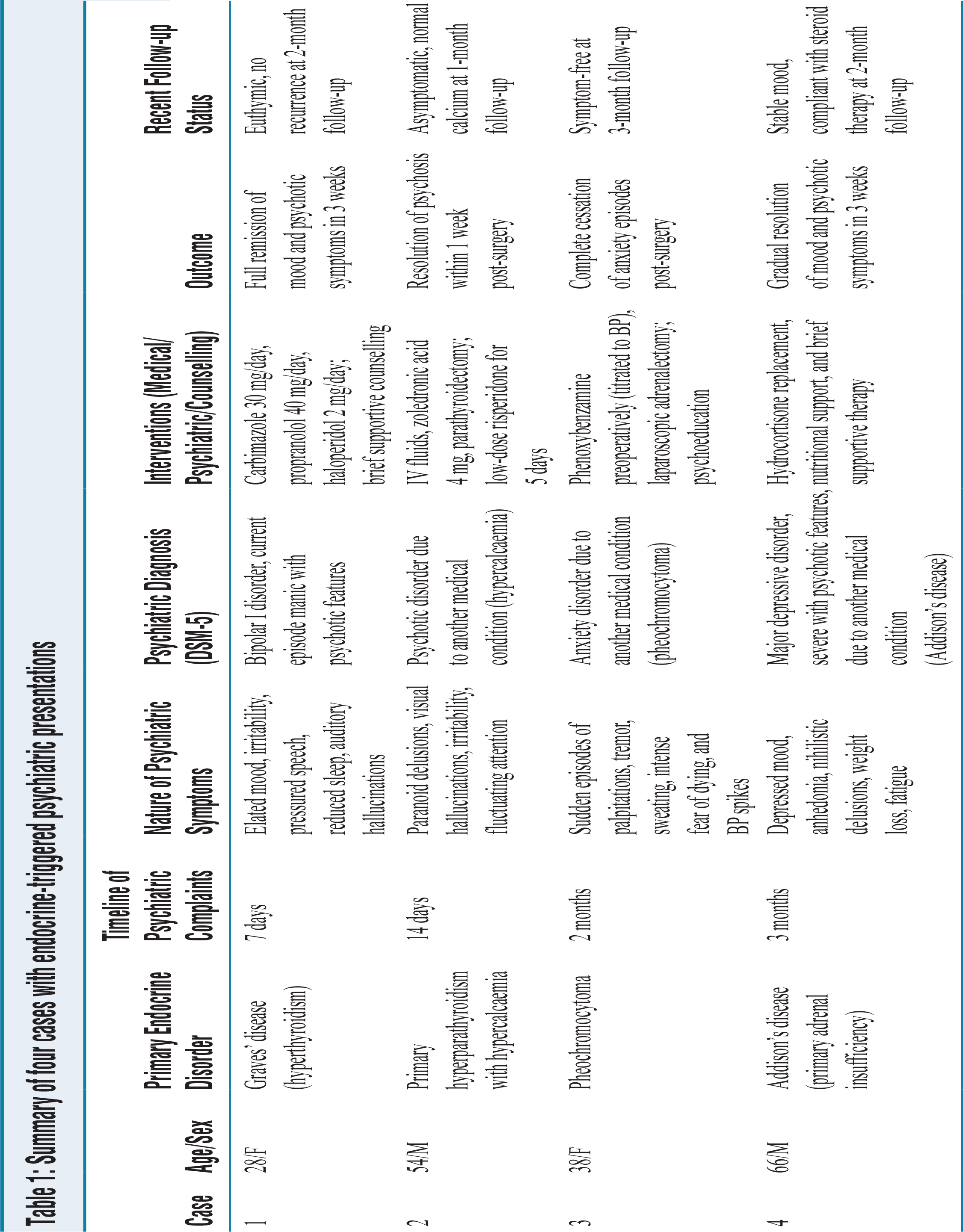
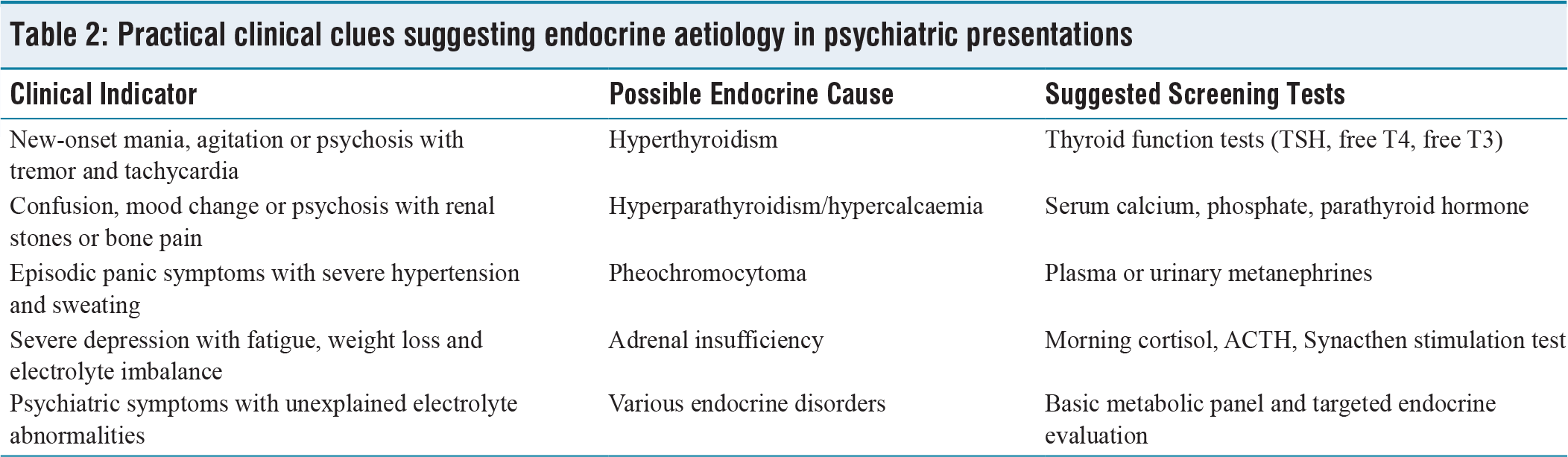
Table 1 summarises the clinical characteristics and treatment outcomes of the four cases presented here. Table 2 outlines practical clinical indicators that may suggest an endocrine aetiology in psychiatric presentations and provides guidance regarding appropriate screening investigations.
Summary of four cases with endocrine-triggered psychiatric presentations
Practical clinical clues suggesting endocrine aetiology in psychiatric presentations
Written informed consent for clinical reporting and publication was obtained from each patient and their primary caregiver.
Discussion
The present case series illustrates how endocrine disorders can produce psychiatric syndromes that closely resemble primary psychiatric illnesses. In all four patients, psychiatric symptoms were the principal reason for seeking medical attention, and the underlying endocrine pathology was detected only after systematic medical evaluation. Such presentations highlight the intimate interaction between the endocrine system and brain function, a relationship increasingly recognised within the framework of psychoneuroendocrinology.[2,11] Hormones regulate neurotransmitter synthesis, synaptic plasticity, neuronal metabolism and stress-response pathways, thereby exerting a profound influence on mood, cognition and behaviour.[12]
Although the exact prevalence of endocrine disorders presenting primarily with psychiatric symptoms in routine psychiatric practice is not well established, available literature suggests that such presentations are uncommon but clinically significant and are likely under-recognised in acute and first-episode settings.[13] Recent reviews have highlighted that thyroid, parathyroid, adrenal and other endocrine abnormalities may contribute to mood, anxiety, cognitive and psychotic syndromes encountered in psychiatric practice.[13] Contemporary guidance on first-episode psychosis also supports a broad medical evaluation, including thyroid function tests, serum electrolytes and other targeted investigations, particularly when symptoms are atypical, abrupt in onset or accompanied by systemic features.[14,15]
One of the most well-established endocrine-psychiatric links involves thyroid dysfunction. Thyroid hormones influence multiple neurotransmitter systems, including serotonin, dopamine and norepinephrine pathways, which are central to the regulation of mood and cognition.[16] Excess thyroid hormone increases adrenergic sensitivity and neuronal excitability, producing symptoms such as anxiety, insomnia, irritability and emotional lability.[16] In severe cases, particularly in untreated hyperthyroidism or thyroid storm, the neurochemical overstimulation may precipitate manic or psychotic states, a phenomenon sometimes described as thyrotoxic psychosis, highlighted earlier by Taha et al.[17] A recent review highlights the bidirectional link between thyroid functioning and neuropsychiatric status, with special vulnerabilities in patients with schizophrenia and bipolar disorder.[18] In the first case, the patient presented with classic manic and psychotic features but also displayed subtle physical signs such as tremor and tachycardia, which prompted endocrine evaluation. Rapid clinical improvement following antithyroid therapy reinforces the importance of identifying the underlying hormonal disturbance rather than treating the presentation as a primary bipolar disorder.
The second case demonstrates another important endocrine mechanism: hypercalcaemia-related neuropsychiatric dysfunction. Primary hyperparathyroidism can cause neuropsychiatric symptoms ranging from mild cognitive impairment and mood changes to delirium and psychosis.[3] Elevated serum calcium affects neuronal membrane stability and interferes with neurotransmitter release, particularly acetylcholine and glutamate, leading to disturbances in cortical and limbic circuits.[19] The classic teaching that hyperparathyroidism produces stones, bones, abdominal groans and psychiatric overtones reflects the well-recognised association between calcium imbalance and mental symptoms.[3] Importantly, psychiatric manifestations may be the presenting feature and resolution of symptoms often occurs rapidly once calcium levels normalise following parathyroidectomy.[19] This was clearly observed in our patient, whose psychotic symptoms resolved within days after surgical treatment.
The case of pheochromocytoma highlights a different diagnostic challenge in psychiatry. Catecholamine-secreting tumours produce episodic surges of epinephrine and norepinephrine, leading to tachycardia, hypertension, sweating, tremor and intense anxiety.[20] These physiological responses closely resemble panic attacks, making misdiagnosis possible when cardiovascular or endocrine evaluation is not performed. Catecholamine excess activates the amygdala and hypothalamic-pituitary-adrenal axis, generating a neurobiological state of heightened fear and arousal similar to that observed in anxiety disorders—often leading to psychiatric emergencies.[21] A distinguishing feature, however, is the presence of paroxysmal hypertension and biochemical evidence of excess catecholamine metabolites such as metanephrines. Early recognition is crucial because untreated pheochromocytoma can lead to life-threatening cardiovascular complications. In our case, appropriate biochemical screening and imaging allowed definitive surgical treatment, after which the panic-like episodes completely resolved.
The fourth case illustrates the psychiatric consequences of adrenal insufficiency, particularly the effects of cortisol deficiency on mood and cognition. Cortisol plays a key role in maintaining metabolic stability and modulating stress responses within the brain. Reduced cortisol levels impair hippocampal function, disrupt monoaminergic neurotransmission and alter circadian regulation of mood and energy.[4] Neuropsychiatric manifestations of Addison’s disease may include apathy, depression, cognitive slowing, irritability and, in rare cases, psychotic symptoms.[4] Historical descriptions even referred to severe psychiatric presentations in adrenal insufficiency as Addisonian psychosis.[22] In the present case, the patient’s depressive symptoms and nihilistic delusions improved rapidly after glucocorticoid replacement, supporting the causal role of endocrine dysfunction in the psychiatric presentation.
Taken together, these cases emphasise that endocrine disorders can present with fully reversible psychiatric syndromes when identified and treated appropriately. While the temporal association between endocrine correction and symptom resolution suggests a causal link, we acknowledge that improvement may also have been influenced by short-term psychotropic use, spontaneous remission or non-specific treatment effects.
However, such diagnoses are frequently overlooked, particularly in emergency psychiatry settings where the immediate focus may be on behavioural control rather than comprehensive medical evaluation. Studies suggest that a significant proportion of first-episode psychiatric presentations may have underlying medical contributors, including endocrine disturbances.[11] Failure to recognise these conditions may result in unnecessary long-term psychotropic treatment and delayed management of potentially serious systemic illness.
Alternative differential diagnoses, including autoimmune encephalitis, central nervous system infections, steroid-induced psychiatric symptoms, metabolic encephalopathy, substance-induced disorders and delirium due to electrolyte imbalance, were considered and excluded based on clinical evaluation, laboratory findings and neuroimaging where indicated.
Follow-up duration in our cases was limited and variable; however, no relapse of psychiatric symptoms was observed during the available follow-up period after correction of the endocrine abnormalities.
From a clinical perspective, several features should prompt clinicians to consider an endocrine cause for psychiatric symptoms. These include first-episode psychiatric illness in midlife or late life, abrupt symptom onset without prior psychiatric history, atypical symptom combinations, fluctuating consciousness or cognition and the presence of unexplained physical signs such as weight changes, electrolyte abnormalities, hypertension or pigmentation changes.[11,23] Laboratory investigations such as thyroid function tests, serum calcium, electrolyte levels and morning cortisol are relatively inexpensive and can provide critical diagnostic clues.
The implications for clinical practice extend beyond individual cases. Psychiatric training and clinical guidelines increasingly emphasise the need for integrated medical evaluation in psychiatric settings, particularly for acute or atypical presentations. Liaison psychiatry services play a crucial role in facilitating collaboration between psychiatrists, endocrinologists and primary care physicians. Early detection of endocrine causes not only improves patient outcomes but also reduces healthcare costs by preventing misdiagnosis and prolonged treatment with unnecessary medications.
Limitations
Like any other case series, this has several limitations. The sample size is small, and cases were collected retrospectively, which may limit generalisability. Follow-up duration was short and variable across cases. A causal relationship between endocrine abnormalities and psychiatric symptoms cannot be definitively established. Additionally, standardised psychiatric reassessment following endocrine treatment was not uniformly performed.
Conclusion
Endocrine disorders can manifest with striking psychiatric syndromes that closely resemble primary psychiatric illnesses. As demonstrated in this case series, conditions such as hyperthyroidism, hyperparathyroidism, pheochromocytoma and adrenal insufficiency may initially present with mood disturbances, anxiety states or psychotic symptoms, sometimes in the absence of obvious systemic signs. Importantly, psychiatric manifestations related to endocrine dysfunction are often reversible when the underlying hormonal abnormality is identified and treated promptly.
These observations highlight the importance of maintaining a high index of suspicion for medical causes in atypical, first-episode or rapidly evolving psychiatric presentations. Incorporating basic endocrine screening—such as thyroid function tests, serum calcium levels and cortisol measurements—into routine psychiatric evaluation can facilitate early diagnosis, prevent misclassification of psychiatric disorders and avoid unnecessary long-term psychotropic treatment. Close collaboration between psychiatry, endocrinology and primary care remains essential for comprehensive patient care and improved clinical outcomes.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Appropriate consent has been obtained from the participants. Case reports are exempt from ethics approval under institutional policy.
Informed consent
Informed consent was obtained from all participants
Credit author statement
Debanjan Banerjee: Conceptualization, data curation, formal analysis, methodology, validation, writing - original draft.
Jayanta Sharma, Sandip Mandal, Aritra Konar, Suvadip Chakrabarti: Conceptualization, data curation, formal analysis, validation, supervision, writing - review and editing.
Data availability statement
On request.
Use of artificial intelligence
No AI tool has been used while writing this manuscript.