
Abstract
Introduction:
Autoimmune disorders (ADs) affect 8.5% of the population globally. Diverse spectrums of antibodies are produced against nuclear antigens called antinuclear antibodies (ANA), which are detected by an array of laboratory tests such as enzyme-linked immunosorbent assay (ELISA), line immunoassay (LIA) and indirect immunofluorescence assay (IIFA). In this background, this study aimed to compare the diagnostic performance of LIA and IIFA in detecting and characterising ANA in patients presenting with clinical features suggestive of systemic autoimmune disease (SAD).
Methods:
A prospective cross-sectional diagnostic accuracy study was performed among 50 patients with clinically evident SADs, who were tested for ANA using IIFA (reference standard) and LIA.
Results:
The most common age group involved in this study was 20–40 years, with a female preponderance noted. ANA positivity was 48% by IIFA and 22% by LIA. The nuclear speckled pattern was the most frequent IIFA finding. Using IIFA as a reference, LIA showed 45.8% sensitivity, 100% specificity and moderate agreement with IIFA (κ = 0.468). All LIA-positive samples were also IIFA-positive.
Conclusion:
IIFA can be used as a screening test, whereas LIA can be a confirmatory test in patients with positive IIFA tests and also indicated in patients with strong clinical suspicion of autoimmune disease but with negative IIFA tests. This algorithm is economical in countries such as India.
Introduction
Autoimmune disorders (ADs) affect 8.5% of the population globally.[1] It is characterised by tissue injury due to a breach in the regulation of immunotolerance mechanisms and antinuclear antibodies (ANA) can be demonstrated in patients’ serum.[2] In patients with ADs, diverse spectrums of antibodies are produced against nuclear antigens, which are detected by an array of laboratory tests such as enzyme-linked immunosorbent assay (ELISA), line immunoassay (LIA) and indirect immunofluorescence assay (IIFA).[3] Reproducibility is a crucial issue because different methods yield different results. In this background, the aim of this study was to compare the diagnostic performance of LIA and IIFA in detecting and characterising ANA in patients presenting with clinical features suggestive of systemic autoimmune disease (SAD) and to propose an evidence-based testing algorithm for resource-constrained healthcare settings.
Materials and Methods
Study Design and Setting
This prospective cross-sectional diagnostic accuracy study was conducted at the department of microbiology of a tertiary care teaching hospital, between October, 2022 and December, 2023. The study protocol received approval from the Institutional Ethics Committee (protocol ID: 20222441, dated 26 October 2022) and written informed consent was obtained from all the study participants.
Study Participants
Consecutive sampling was employed to include all patients aged ≥18 years attending the rheumatology outpatient department with a clinical diagnosis or strong clinical suspicion of SADs based on American College of Rheumatology (ACR) criteria or Alarcon-Sergovia criteria for mixed connective tissue disorders (MCTDs).
Exclusion criteria included concomitant infection with human immunodeficiency virus (HIV) or hepatitis B virus, active malignancies, pregnancy or refusal to provide informed consent.
Clinical Definitions
Systemic lupus erythematosus (SLE): Diagnosis based on ACR criteria requiring ≥4 of the following 11 criteria: Malar rash, discoid rash, photosensitivity, oral ulcers, non-erosive arthritis, pleuritis or pericarditis, renal disorder (proteinuria >0.5 g/day or cellular casts), neurologic disorder (seizures or psychosis), haematologic disorder (hemolytic anaemia, leukopenia, lymphopenia or thrombocytopenia), immunologic disorder (anti-double-stranded DNA [dsDNA], anti-Smith [Sm] or antiphospholipid antibodies) or positive ANA.
Systemic sclerosis (SSc): Diagnosis based on ACR/EULAR criteria, including skin thickening, digital ulcers, Raynaud’s phenomenon and specific autoantibodies.
Mixed connective tissue disease (MCTD): Diagnosis based on the Alarcon-Segovia criteria requiring anti-U1-ribonucleoprotein (RNP) antibodies plus ≥3 of the following: Raynaud phenomenon, synovitis, myositis, hand oedema or acrosclerosis.
Rheumatoid arthritis (RA): Diagnosis based on ACR/EULAR 2010 criteria.
Sjögren’s syndrome (SjS): Diagnosis based on ACR/EULAR 2016 classification criteria.
Socio-demographic details, relevant personal history, details of co-morbid illness, symptomatology and clinical and radiological examination findings were collected in a structured proforma. A brief clinical examination was done, including skin and joints.
Sample Size Calculation
The sample size was calculated using Buderer’s method for diagnostic accuracy studies, assuming an expected sensitivity of 90%, specificity of 85%, disease prevalence of 40%, 95% confidence level and ±10% precision, yielding a minimum required sample size of 50 patients. Post-hoc power analysis confirmed 80% power to detect a 15% difference in sensitivity between IIFA and LIA at α = 0.05.
Index Test and Reference Standard
IIFA was considered the reference standard. LIA was evaluated as the index test.
Blinding
IIFA slides were independently interpreted by two trained microbiologists blinded to clinical data. Discordant recordings were resolved by a senior consultant from the manufacturer. LIA was performed and interpreted by a separate researcher blinded to IIFA results and clinical information.
Laboratory Methods
Five millilitres of venous blood were collected under standard aseptic precautions. Serum was separated by centrifugation and stored at −20 °C until analysis. IIFA and LIA were performed using fluorescent Hep-2000 ANA/Ro and Imtec-ANA-LIA XL kits (Medsource Ozone Biomedicals Pvt. Ltd., New Delhi, India), respectively, in accordance with the manufacturer’s instructions.
IIFA patterns were examined under a fluorescence microscope and categorised as nuclear, cytoplasmic, mitotic or centromere patterns. The ANA titre was determined for each sample. For ANA-LIA, following completion of the assay steps, the final immunoassay strip was placed on the evaluation template supplied with the kit and the presence or absence of specific ANA antibodies was recorded. Quality control procedures were maintained throughout both IIFA and LIA testing.
Statistical Analysis
The data obtained were analysed with IBM SPSS version 29 (2022) (IBM Corp, Armonk, USA). Diagnostic accuracy parameters (sensitivity, specificity, positive predictive value [PPV], negative predictive value [NPV]) with 95% CI were calculated using IIFA as the reference. Agreement was evaluated using Cohen’s kappa statistic. The Student t-test was applied for continuous variables, while the chi-square test was used for categorical variables. The associations between IIFA, LIA and various SADs were studied.
Results
During the 12-month study period, 58 patients with suspected SADs were screened. Eight were excluded due to HIV infection (three), active hepatitis B (two), refusal to participate (two) and insufficient serum sample (one). The final analysis included 50 patients who were screened with IIFA and the results were confirmed using LIA testing with no missing data.
Among them, 38 (76%) were females and 12 (24%) were males. The mean age of the study participants was 38.16 ± 13.09 years, with ages ranging from 16 to 80 years. A higher proportion of females belonged to the 20–40-year age group. Skin (n = 20, 40%) was the most commonly affected site, followed by bone/joint involvement (n = 8, 16%). Sixteen (32%) patients had SLE, followed by SSc in 12 (24%) [Table 1].
Socio-demographic details of the study participants

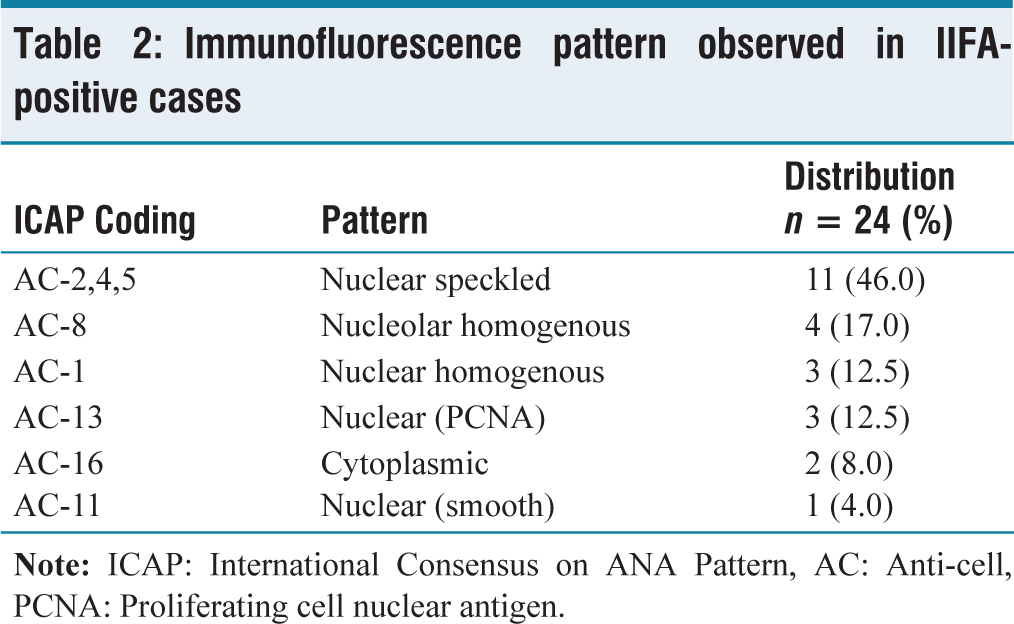
With IIFA, 24 samples (48%) were ANA positive and 26 (52%) were ANA negative. Based on the International Consensus on ANA Patterns, the immunofluorescence patterns identified in this study were nuclear speckled in 11 samples (46%), nucleolar homogeneous in four (17%), nuclear homogeneous in three (12.5%) and nuclear, proliferating cell nuclear antigen (PCNA) in three (12.5%) [Table 2]. In contrast to ANA-IIFA, only 11 (22%) samples were ANA positive with LIA.
Immunofluorescence pattern observed in IIFA-positive cases
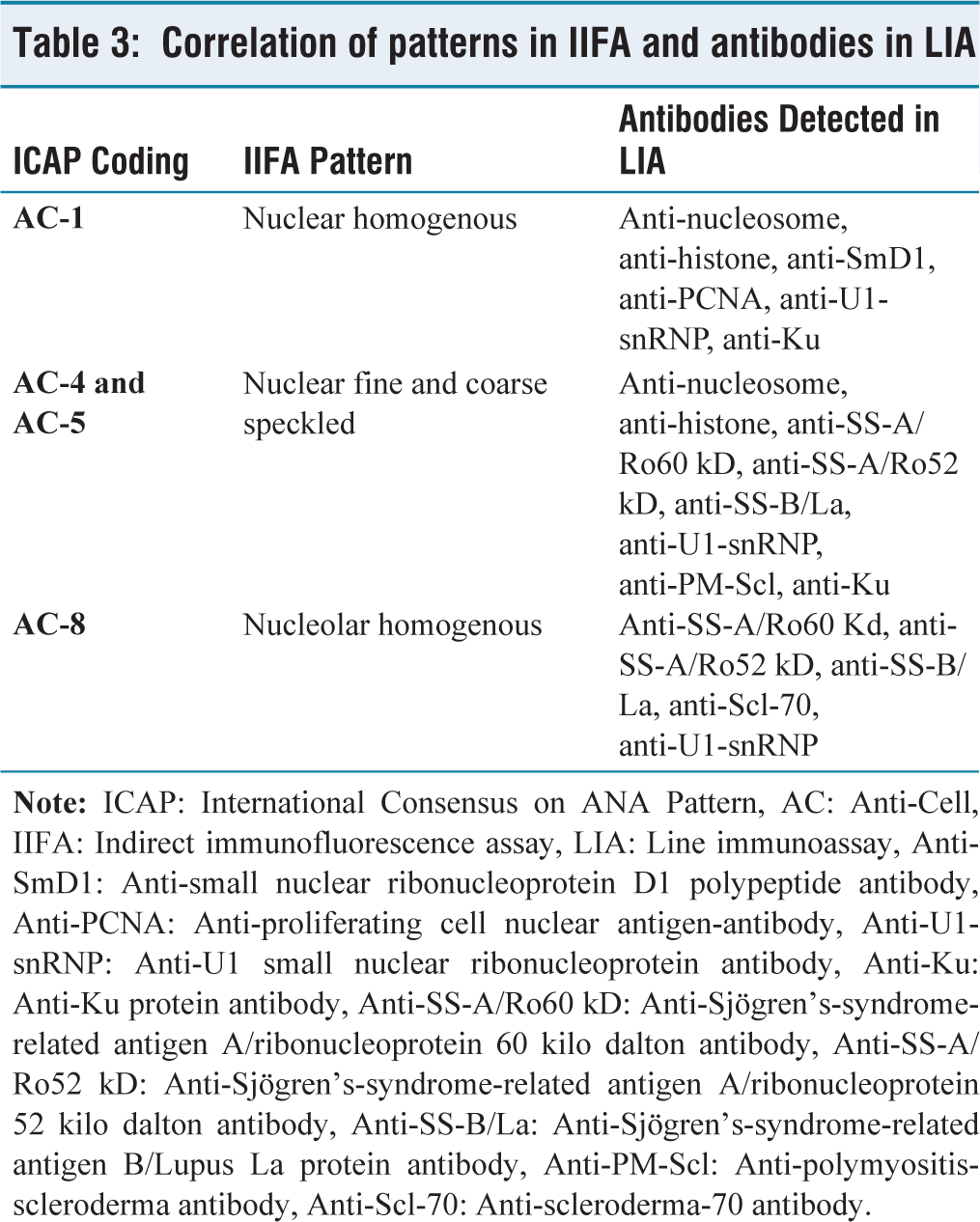
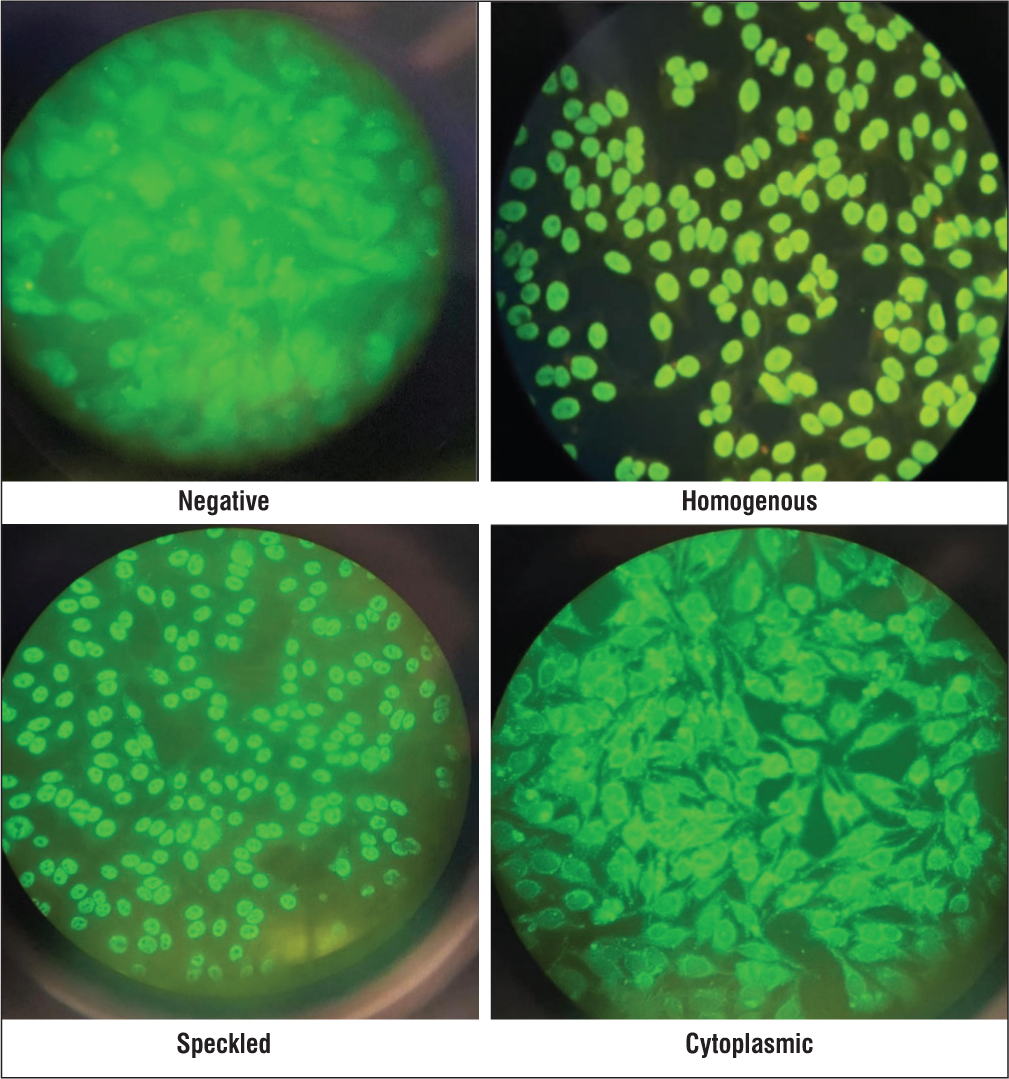
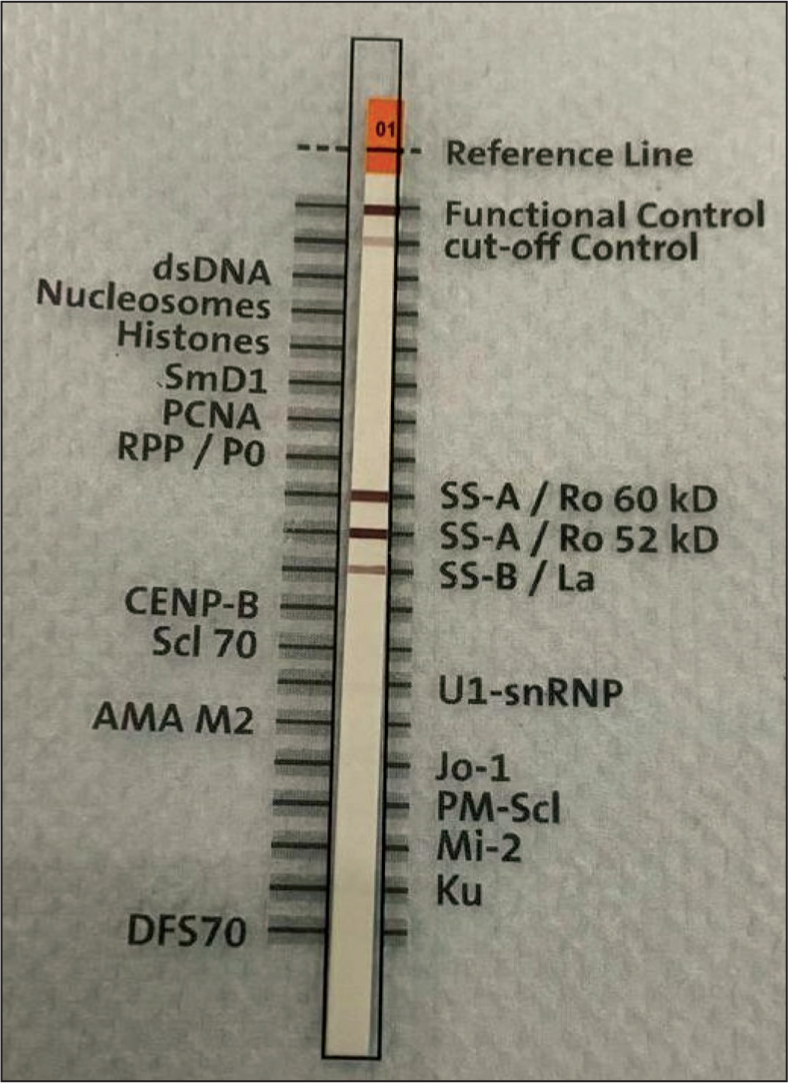
Among the 11 samples that tested positive by both assays, the antibodies detected by LIA and the immunofluorescence patterns by IIFA were described in Table 3 [Figures 1 and 2].
Correlation of patterns in IIFA and antibodies in LIA
Indirect Immunofluorescence patterns noted in the study
Line Immunoassay strip positive for Systemic Sclerosis
An unpaired Student t-test was done to analyse the association of age groups and ANA-IIFA seropositivity. The mean age of the ANA-IIFA-positive group was 38.71 ± 12.46, while that of the ANA-IIFA-negative group was 37.65 ± 13.87. The P value was found to be 0.779. With the chi-square test, the P value for the association between ANA-IIFA positivity and gender was .411. As both these values are greater than .05, they are not statistically significant [Table 1].
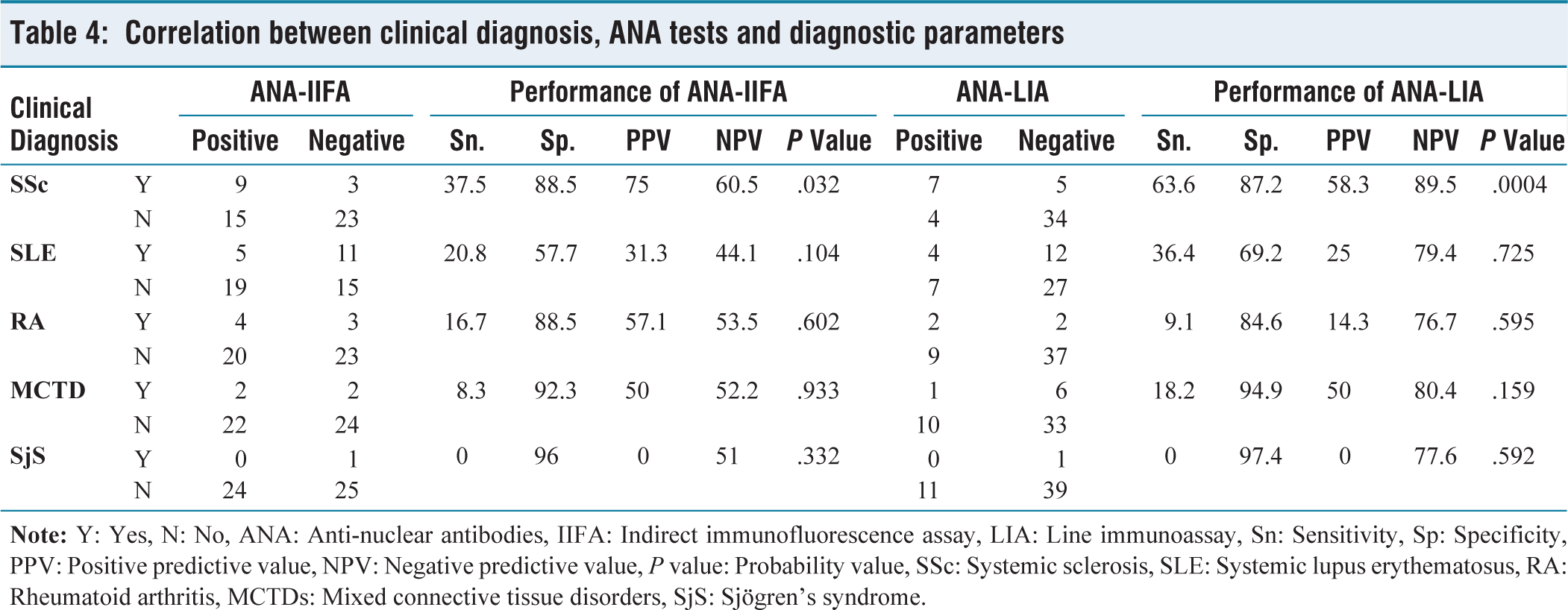
The chi-square test found the P values for ANA-IIFA positivity and ANA-LIA positivity were .032 and .0004, respectively, for SSc, while for the other diseases were more than.5 [Table 4].
Correlation between clinical diagnosis, ANA tests and diagnostic parameters
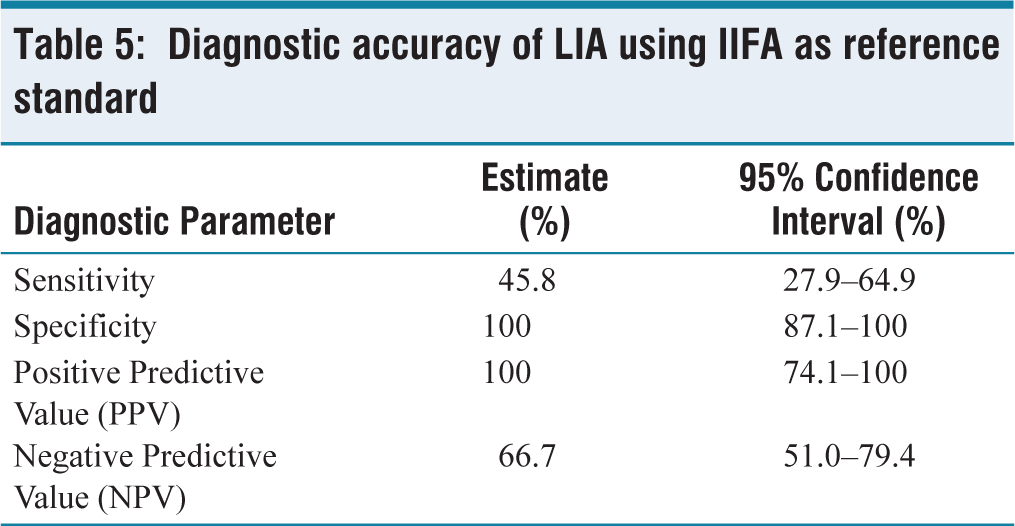
In this study, using IIFA as a reference standard, the diagnostic performance of LIA was systematically evaluated. LIA demonstrated high specificity (100%) with comparatively lower sensitivity (45.8%), indicating its strength as a confirmatory rather than a screening assay. The high specificity and PPV (100%) indicate that all LIA-positive results were true positives when compared with IIFA [Table 5].
Diagnostic accuracy of LIA using IIFA as reference standard
Agreement between IIFA and LIA was assessed to determine inter-method concordance. Overall agreement was observed in 74% of cases. Cohen’s kappa coefficient was 0.468, indicating moderate agreement beyond chance. All samples that were positive by LIA were also positive by IIFA, whereas discordant results were limited to cases that were IIFA-positive but LIA-negative.
Discussion
SLE, SjS, SSc and MCTD are the conditions directly linked to ANAs and referred to as ANA-associated rheumatic disorders (AARDs). The diagnostic criteria for AARDs include specific antibodies against double-stranded DNA (dsDNA) and the Sm antigen for SLE, Ro60 and SS-B/La for SjS, Scl-70 and RNA polymerase III for SSc and U1 RNP for MCTD.[4]
Although the AD cases are on the rise, SAD is still frequently misdiagnosed and untreated in underdeveloped nations. These patients present with nebulous symptoms, leaving doctors in a clinical puzzle. Recognition of SAD is frequently challenging and subject to many variables, including significant medical history, clinical examination and testing for specific autoantibodies in patients’ serum.[1]
One of the main tests for diagnosing clinically suspected SAD is the ANA test; however, a considerable proportion of patients with neoplasia, chronic liver disorders and active infections such as malaria and tuberculosis, as well as healthy people, may test positive for ANA, particularly at low levels.[1]
As AD patients alone exhibit elevated ANA titres, it serves as a diagnostic and prognostic indicator. Therefore, it is crucial for the diagnosis to identify these antibodies using techniques with high precision and accuracy.[5]
Although it affects people of all ages, genders and races, some people are more likely to develop this condition.[1] In this study, female preponderance was noted, which was similar to the study by Kaur et al.[1] Gunnarsson et al.[6] and Kumar et al.[7]
The most common age group involved in this study was 20–40 years, which is in concordance with other similar studies by Angel et al.[8] ADs most frequently affect women between the ages of 20 and 50 due to endocrinological changes brought on by puberty, pregnancy and menopause. Women are more vulnerable to ADs as a result of the endocrinological changes, which take place at various stages of their lives and impact the immune system through unfavourable interactions between both the adaptive and innate immune response, fluctuating hormone levels and the release of pro- and anti-inflammatory cytokines.[9]
The most common pattern obtained in this study was nuclear speckled 11 (46%), which is similar to the other studies by Kumar et al.[7] and Petchiappan et al.[10] yet in another study by Sebastian et al.[11] reported that the homogeneous pattern was the most common ANA pattern
In the current study, 32% of the study participants were diagnosed with SLE, which is concordant with a study by Angel et al.[8] Frequently found autoantibodies in SLE were anti-U1-snRNP and anti-Ku antibodies, three (19%), followed by anti-histone two (13%). Though anti-dsDNA autoantibodies are highly specific for SLE, in the present study, anti-dsDNA was not detected in any samples. Anti-dsDNA antibodies have more than 95% specificity for SLE but are found in only about 60% to 70% of SLE patients; therefore, a negative anti-dsDNA does not rule out the diagnosis of SLE.[12]
Although IIFA is considered the gold standard test, containing 100–150 antigens, it is labour-intensive and requires technical expertise and expensive equipment, such as fluorescence microscopes, which may not be available in resource-limited areas.[3,13] Although the presence of ANA is demonstrated by positive fluorescence staining, the specific type of autoantibodies cannot be accurately identified. While interpreting IIFA, three important factors are considered, which include the pattern of fluorescence, substrate and the titre of a positive test. A negative IIFA excludes the possibility of active connective tissue disease.[5]
LIAs are very simple to use as screening assays where up to 17 distinct autoantibodies can be distinguished with a single assay by spotting antigens in lines on a simple nitrocellulose membrane.[3]
In the present study, the sensitivity of LIA was 46%, which is lower than that of Kumar et al.[7] Jeon et al.[14] and with a sensitivity of 61% and 66.1%, respectively. The low sensitivity in the current study suggests that ANA-LIA is better at confirming the disease when the screening test is positive, rather than identifying all true positive cases. This may lead to false negativity if LIA is used as a screening tool.
ELISA or IIFA can be used as a screening test, depending on the specimen load and LIA can be a confirmatory test. Numerous detection methods, such as flow cytometry and nanotechnology, are constantly emerging which are used in diagnostics and treatment monitoring.[2]
The limitations of the study include a single-centre study. The sample size was limited due to the expense associated with the LIA test. Due to financial constraints, dsDNA antibodies were not tested using the chemiluminescent assay, which has high specificity.
Conclusion
In the present study, ANA positivity using IIFA and LIA was 48% and 22%, respectively. IIFA, by employing biochip wells, delivers quick and efficient results for ANA detection, which can be used as a screening test due to its ability to detect multiple autoantibodies simultaneously. Its fluorescent pattern can forecast the presence of certain antibodies in the serum. LIA can be used as a confirmatory test in patients with positive IIFA and is also indicated in patients with a strong clinical suspicion of AD but a negative IIFA. This algorithm is economical in countries such as India.
Footnotes
Acknowledgements
We thank all the laboratory technicians for sample processing and testing. No contributor has been omitted.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
20222441, dated 26 October 2022.
Informed consent
Written informed consent was obtained from all the study participants.
Credit author statement
Dr Jamal Badruddin Akbar Salim: Investigation, conceptualisation, methodology, writing-original draft.
Dr Gowri Subbiah: Conceptualisation, supervision, writing-review and editing.
Dr Poongodi Santhana Kumarasamy: Conceptualisation, data curation, formal analysis, writing-review and editing.
Dr Indira Ananthapadmanabasamy: Investigation, validation, writing-review and editing.
Data availability statement
The data have not been published or presented anywhere else.
Use of artificial intelligence
The authors used Grammarly to improve grammar, spelling and overall readability. After using this tool, the authors reviewed and edited the content as needed and took full responsibility for the final content of the publication.