
Abstract
Enterocloster clostridioformis, a recently reclassified anaerobic bacillus, is recognised rarely as a human pathogen in bloodstream and intra-abdominal infections. Vascular complications secondary to such anaerobic sepsis in young, immunocompetent patients are exceptionally rare. Here we present a 27-year-old male chronic alcoholic with prolonged fever, gastrointestinal symptoms and imaging evidence of extensive mesenteric venous thrombosis. Blood cultures grew E. clostridioformis. Treatment with targeted carbapenem antibiotics and prolonged anticoagulation led to full recovery. This report underscores the need for early recognition of anaerobic sepsis-related vascular complications and timely management to achieve favourable outcomes, especially in uncommon presentations linked to chronic alcoholism.
Keywords
Introduction
Acute mesenteric ischaemia secondary to bacteraemia, especially in immunocompromised young individuals, often presents diagnostic and therapeutic challenges. Most reported mesenteric vein thrombosis (MVT) cases are seen in the context of prothrombotic disorders or intra-abdominal infections, with classical risk factors including malignancy, cirrhosis or inherited thrombophilia.[1] Enterocloster clostridioformis, earlier called Clostridium clostridioforme, is a gram-positive, obligate anaerobic bacillus residing in the gastrointestinal tract.[2] Only a few clinical reports have documented E. clostridioformis as an etiological agent in bacteraemia, usually in older or immunosuppressed patients and nearly always in the context of mixed infections or predisposing comorbidities.[3]
The uniqueness of this case is that extensive pure-culture E. clostridioformis bacteraemia with consequent mesenteric venous thrombosis in a young chronic alcoholic without other prothrombotic risk factors expands the clinical spectrum of this rare pathogen. Increasing awareness of such rare clinical entities, especially in patients with chronic alcohol consumption and severe intra-abdominal infection, may improve diagnostic accuracy and patient survival.
Case Presentation
A 27-year-old male, chronic alcoholic with no other known comorbidities, presented with 20-day history of non-bilious, non-projectile vomiting, reduced appetite, along with 10 days of high-grade fever with chills and rigours. He reported significant weight loss of 8 kg over two weeks and markedly reduced oral intake. Patient’s personal history was significant for a 10-year history of chronic ethanol consumption, consuming approximately 8-10 units of alcohol(whisky) per week. There was no history of malignancy, chronic steroid use, chemotherapy or immunosuppressant medications.
On admission, he was febrile (101.2 °F), tachycardic (145/min) and hypotensive (80/40 mmHg) with peripheral oxygen saturation (SpO₂) of 96% on room air. He received aggressive fluid resuscitation with intravenous crystalloids (1 L normal saline), following which his BP improved to 90/60 mm Hg with reduced tachycardia to 120/min. Despite fluid resuscitation, he remained hemodynamically unstable and subsequently required vasopressor support with noradrenaline at 2 mL/h. General and systemic examinations were largely unremarkable except for sluggish bowel sounds. Two sets of blood cultures were obtained from different sites and the patient was started on empirical antibiotic therapy with intravenous ceftriaxone 2 g once daily and oral azithromycin 500 mg once daily. Laboratory evaluation revealed anaemia (Hb 9.7 g/dL), leukocytosis (TC 20,830/μL), elevated ESR (69 mm/h), CRP (50 mg/L), normal renal function tests (serum urea 22 mg/dL, serum creatinine 1.01 mg/dL), hypoalbuminemia (2.8 g/dL), raised liver enzymes (SGOT/SGPT 58/54 U/L, GGTP 396 U/L, ALP 247 U/L) and deranged bilirubin (2.48/1.93 mg/dL). Glycated hemoglobin (HbA1c) was 5.7%. Viral markers, including Human Immunodeficiency virus (HIV), Hepatitis B surface antigen (HBSAg) and anti-Hepatitis C virus (HCV), were negative. Ultrasonography (USG) abdomen was done, which showed grade I fatty liver with areas of focal fat sparing, patent intrahepatic and extrahepatic biliary radicles, a partially distended gallbladder with normal wall thickness, but inadequate visualisation of the aorta and inferior vena cava due to overlying bowel gas.
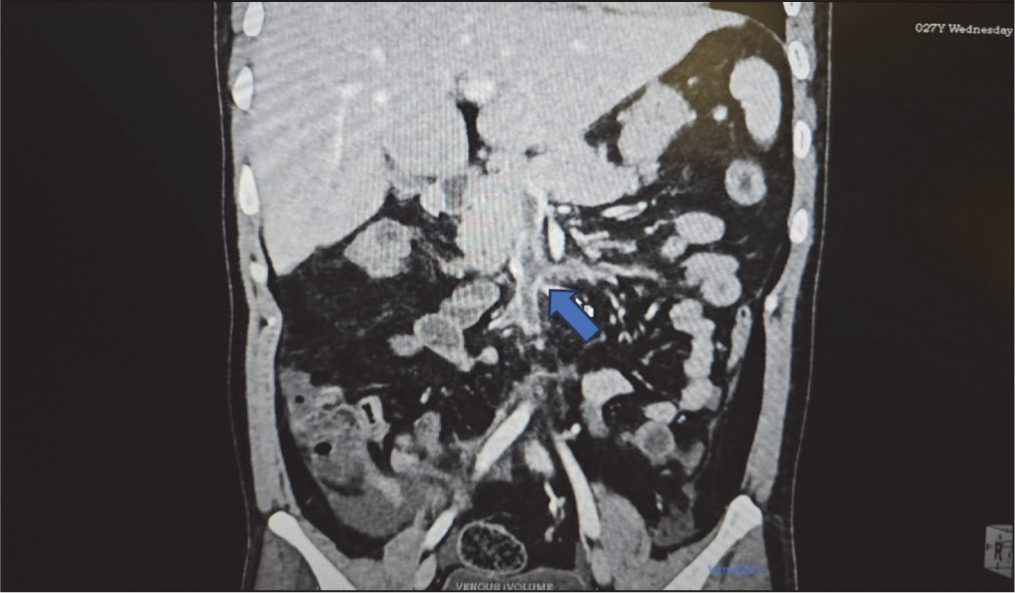
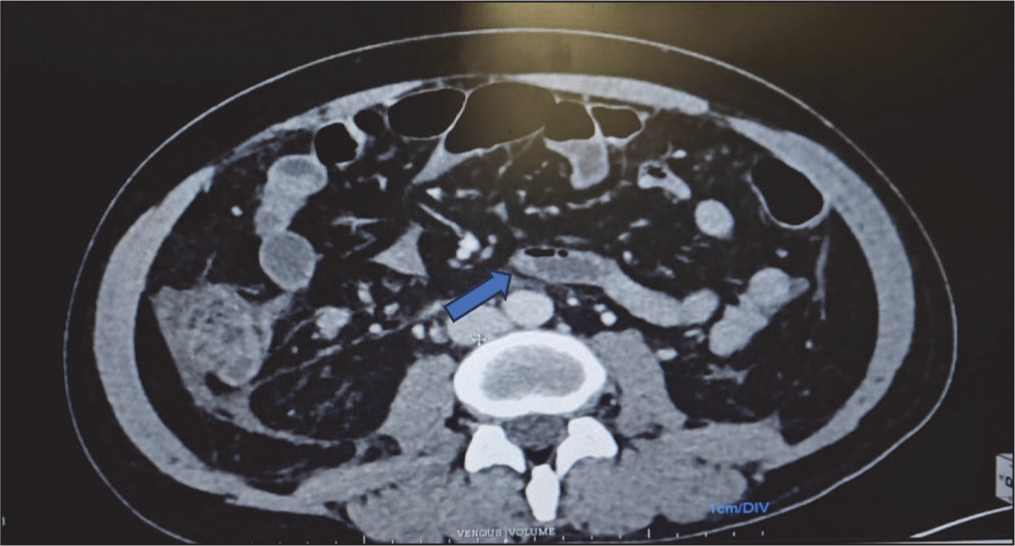
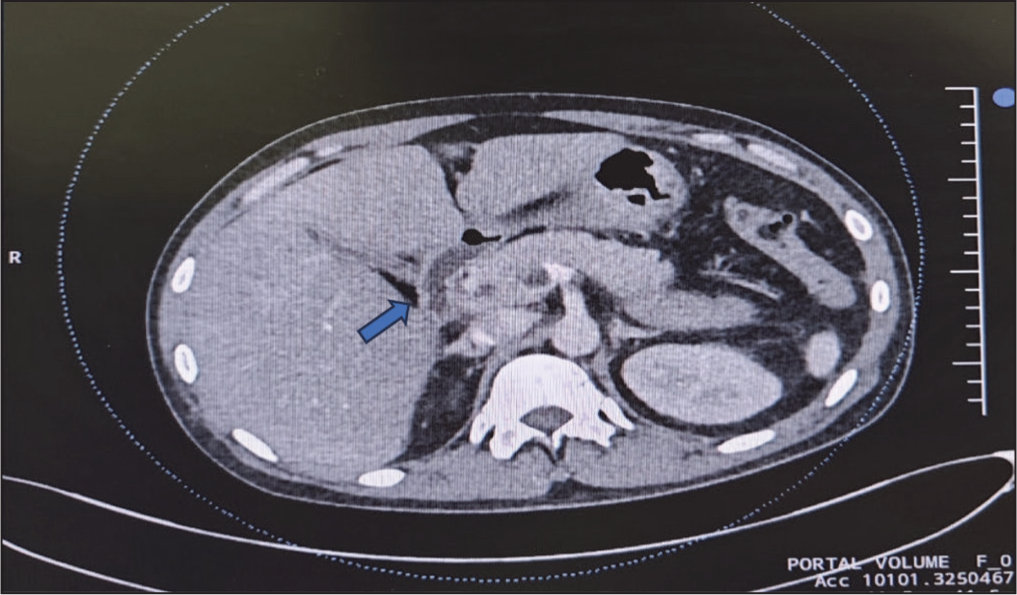
Despite two days of initial management with intravenous ceftriaxone 2 g and oral azithromycin 500 mg, supplemented with aggressive fluid resuscitation with 1 L NS, the patient developed persistent fever spikes (38.5°C-39.2°C) and worsening hemodynamic instability in the form of hypotension BP <80/60 mm Hg. Hence was escalated to intravenous meropenem 1 g three times daily on day three of admission. A Contrast enhanced computed tomography (CECT) abdomen was also done, which revealed extensive mesenteric venous thrombosis involving tributaries of the superior mesenteric vein [Figure 1], ileocolic vein, entire superior mesenteric vein, spleno-mesenteric confluence and partial portal vein thrombosis [Figure 2], with bowel wall oedema suggestive of venous ischaemia [Figure 3]. The patient was started on a low activated partial thromboplastin time (aPTT) protocol heparin infusion with an initial bolus of 5,000 units IV, followed by continuous infusion at 800–1,000 units per hour, adjusted to maintain aPTT at 1.5–2.5 times the upper limit of normal. Blood cultures were followed daily and initially, it was reported as gram-negative bacilli, raising the suspicion of enteric fever. However, on subsequent days, it was reported as gram-positive bacilli. Hypercoagulability workup, including antiphospholipid antibodies (lupus anticoagulant, antiphosphatidyl serine, anti-beta 2 glycoprotein, anticardiolipin antibodies), factor V Leiden-prothrombin gene mutation and vasculitis package, was negative. He showed significant improvement in hemodynamics once antibiotics were changed from ceftriaxone to meropenem. There was a resolution of the fever and improved clinical status. Hence, he was discharged with once-a-day intravenous ertapenem 1 g and twice daily subcutaneous enoxaparin 60 mg. During the follow-up visit, blood culture was reported as Enterocloster clostridioformis, thus ruling out enteric fever. Antimicrobial susceptibility testing showed E. clostridioformis resistant to penicillin G (>8 μg/mL), ampicillin, cefoxitin and clindamycin, but susceptible to meropenem (0.5 μg/mL), ertapenem (0.25 μg/mL), metronidazole (2 μg/mL) and piperacillin-tazobactam. According to the sensitivity pattern, antibiotics were changed to oral metronidazole 500 mg thrice daily for two weeks and anticoagulation was administered with oral rivaroxaban 15 mg twice daily for six months.
Coronal section showing superior mesenteric vein and portal vein thrombosis
Transverse section showing extensive MVT with bowel congestion
Transverse section showing partial portal vein thrombosis
Telemedicine consultation showed symptomatic improvement with antibiotics and blood thinners, but the patient declined repeat blood cultures and follow-up CECT; hence, we could document only clinical recovery. Objective radiological follow-up, ideally with duplex ultrasound/CECT at 6–8 weeks and 3–6 months, to confirm recanalisation and complete laboratory documentation of sustained recovery could not be obtained due to poor follow-up adherence.
Discussion
MVT in young adults remains uncommon; when present, underlying risk factors are usually identified, such as inherited thrombophilia, intra-abdominal infections or malignancy.[1] Our case underscores an unusual scenario of Extensive MVT complicating pure-culture E. clostridioformis sepsis in a young, otherwise healthy alcoholic adult, without hypercoagulability.
Patients infected with Enterocloster clostridioformis bacteraemia often have associated conditions such as advanced age, diabetes or malignancy and accurate diagnosis relies on advanced identification methods such as Matrix assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF) MS.[2]
Anaerobic bacteraemia, especially with rare or reclassified organisms, is frequently linked to high morbidity and mortality, especially when empirical antibiotic coverage is inadequate or delayed.[2] Enterocloster clostridioformis exhibits broad resistance patterns, including penicillin, beta-lactam/beta-lactamase inhibitor combinations. Carbapenems and metronidazole consistently demonstrate effective antimicrobial activity against this organism, supporting their use as primary treatment options.[2]
Gram stain variability in anaerobes, including Enterocloster clostridioformis, occurs due to oxygen-induced disruption of the bacterial cell wall, leading gram-positive organisms to sometimes appear gram-negative or gram-variable on microscopy. Studies highlight that this day-to-day gram stain variability should alert the physician that they are dealing with anaerobes and prompt the addition of carbapenem, as in this case, which will result in appropriate clinical outcomes.[3]
Enterocloster clostridioformis bacteraemia is predominantly associated with polymicrobial infections, often occurring alongside other anaerobes such as Dialister micraerophilus, as reported by Kitagawa et al. in a female with pelvic abscess.[4]
Comparatively, reports of major vascular complications attributable to systemic infection are exceedingly few. Mesenteric or splenic vein thrombosis complicating typhoid (Salmonella Typhi and Paratyphi) fever has been described in a paediatric case and in young adults, highlighting how severe abdominal sepsis of enteric origin can precipitate intra-abdominal vascular events.[5,6] Veronese et al. reported a case of both superior mesenteric vein and splenic vein thrombosis secondary to typhoid fever, which was effectively treated with antimicrobial therapy with metronidazole and albendazole and antithrombotic therapy with aspirin.[5]
While Zahid et al. reported a case of isolated splenic vein thrombosis and splenic infarct in an otherwise healthy boy with severe enteric fever, which was managed with antibiotics (injection ceftriaxone, oral azithromycin, oral metronidazole) and supportive care.[7]
Similarly, acute arterial thrombosis, including embolic phenomena, has been documented with hypervirulent Klebsiella pneumoniae pneumonia as reported by Bao et al.[8]
Alcoholism itself is a recognised risk factor for both gut mucosal barrier dysfunction and microbiome shifts, including the emergence of novel acetaldehyde-producing Enterocloster species.[9] The isolation of Enterocloster alcoholdehydrogenati from the intestines of an alcoholic, as reported by Oikawa et al. highlights the pathogenic potential and adaptation of the genus in altered host environments.[9] In our case, chronic ethanol exposure may have facilitated not just bacteraemia but also a prothrombotic milieu.
Antimicrobial therapy followed Infectious diseases society of America (IDSA) anaerobic infection guidelines with early meropenem escalation (1 g IV Three times daily [TDS]) for persistent septic shock and gram stain variability, transitioning to oral metronidazole per susceptibility (total six weeks), consistent with Surviving Sepsis Campaign recommendations for intra-abdominal source control.[10] Anticoagulation adhered to American Society of Hematology (ASH) 2023 splanchnic vein thrombosis guidelines using initial IV unfractionated heparin (target aPTT 1.5–2.5× normal) followed by rivaroxaban for a six-month duration, preventing thrombus propagation despite active infection.[11]
Conclusion
This case of Enterocloster clostridioformis bacteraemia causing extensive mesenteric venous thrombosis highlights that vascular causes must be considered in young patients presenting with abdominal pain and systemic features without a clear aetiology. Gram stain variability from gram-positive to gram-negative mandates early empirical carbapenem coverage alongside anaerobic cultures. A high index of suspicion with early CECT imaging is essential for timely diagnosis, while anticoagulation combined with targeted antibiotics forms the cornerstone of therapy. Systematic evaluation for underlying prothrombotic states remains crucial, even in the context of sepsis-induced coagulopathy from rare anaerobic pathogens.
Supplemental material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
To the Research Department, Apollo Hospitals, Chennai.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Institutional ethics committee approval was not required for this case report.
Patient consent
Patient consent was not required.
Credit author statement
AC: Participated in data acquisition, literature search, investigations, data analysis and manuscript preparation.
MM, SV, PB: Participated in conceptualisation, investigation and supervision.
All authors have reviewed and approved the manuscript.
Data availability
Data presenting the study’s findings are available from the corresponding author.
Use of artificial intelligence
No artificial intelligence tools were used for patient data generation or clinical decision making; they were used only for language editing.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.