
Abstract
Osteochondromas are one of the commonest benign bone neoplasms, and are typically asymptomatic and non-progressive. They can, however, cause several complications, the most important being malignant transformation into peripheral chondrosarcoma, particularly in patients with hereditary multiple exostoses. Other known complications include either osseous or cosmetic deformities, fracture, vascular compromise, neurologic sequelae from adjacent nerve compression, overlying adventitial bursa formation, pain and rarely pressure erosion of adjacent bones. Synostosis (fusion) of the distal portion of an osteochondroma to its native bone is a rare complication, not described in the existing literature. A case of osteochondroma fusion to the native bone is described in a 17-year-old patient, who was diagnosed with an osteochondroma of the right distal femur 4 years prior and now presented with pain and an enlarging mass in the region. Radiographs and MRI revealed a pedunculated osteochondroma, with its distal portion fused to the native femur, resulting in an unusual ‘mug handle’ like appearance. Due to the clinical symptoms, the osteochondroma was surgically excised. Pathology revealed no evidence of malignancy, and the patient made an uneventful recovery.
Keywords
Introduction
Osteochondromas constitute approximately 20%–50% of benign primary bone tumours and account for almost 10%–15% of all primary bone lesions. They can either be solitary or multifocal, the latter usually seen in a genetic condition known as hereditary multifocal exostoses (HME).[1] Solitary osteochondromas can also arise following Salter-Harris fractures, surgery and radiotherapy, and can also occur due to certain genetic mutations.[1] The vast majority of osteochondromas are asymptomatic.
Several complications can arise in relation to osteochondromas, and these include either osseous or cosmetic deformities, fracture, vascular compromise, neurological sequelae from compression of adjacent nerves, overlying adventitial bursa formation, and, importantly, malignant transformation into peripheral chondrosarcoma.[2] Additionally, mechanical pressure erosion of adjacent bones as well as synostosis of adjacent osteochondromas has been described.[3] However, the synostosis of a pedunculated osteochondroma to its native bone has not been described in the existing literature as a recognised complication. Furthermore, a retrospective review of 1,000 cases of pedunculated osteochondromas imaged over 10 years at our tertiary sarcoma centre did not reveal any cases with this complication. As such, this would be the first reported case of this entity.
We describe a case of a 17-year-old patient with a known pedunculated osteochondroma of the right distal femur diagnosed 4 years ago. The initial imaging revealed a characteristic appearing pedunculated osteochondroma complicated by an undisplaced fracture, which was managed conservatively. Subsequent imaging performed during the current presentation, due to the patient now being symptomatic, revealed interval growth of the osteochondroma and an unusual morphology with synostosis to the native bone resembling that of a mug handle. The lesion was surgically excised due to the symptoms, with histopathological examination of the specimen revealing no evidence of malignancy.
This article aims to make the reader aware of this unusual and previously undocumented complication that can arise in relation to a pedunculated osteochondroma, which we have termed the ‘mug handle sign’. The case adds to the existing knowledge of complications of osteochondromas, and it is important that radiologists and clinicians are able to recognise the entity as a benign complication if it is encountered in clinical practice.
Case Report
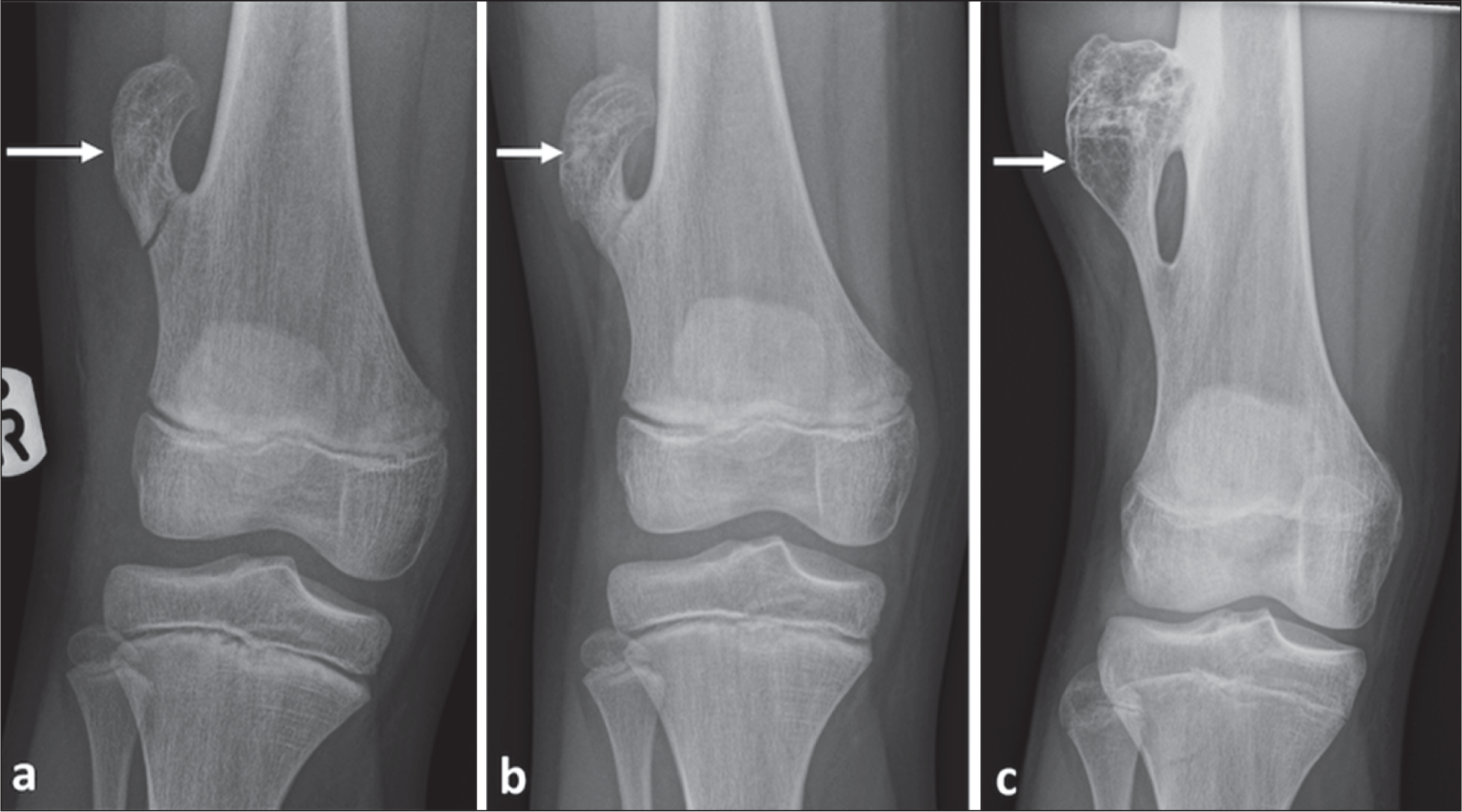
A 17-year-old male presented with a gradually enlarging lump on the lateral aspect of his right thigh, with associated discomfort, particularly during strenuous activity. It was tender to palpation. The lump was initially noticed 4 years prior, with associated pain resulting from a minor football injury. Initial radiograph at the time had demonstrated a pedunculated osteochondroma of the right lateral distal femoral metaphysis, with fairly typical imaging features. This was complicated at the time by an undisplaced fracture of the pedicle of the osteochondroma [Figure 1a]. Given the absence of concerning imaging features at the time, it was conservatively managed. Follow-up radiograph 4 weeks after the first presentation demonstrated evidence of fracture healing with some callus formation [Figure 1b]. The patient remained asymptomatic after this episode until his current presentation 4 years later.
(a-c) Radiographs demonstrating an osteochondroma of the right distal femoral metaphysis (white arrows). Initial radiograph 4 years prior to the time of diagnosis (a) demonstrates an undisplaced fracture at its base. Note the typical location and features of a pedunculated osteochondroma, pointing away from the joint as classically described. Subsequent radiograph 4 weeks later demonstrates evidence of ongoing fracture healing (b). Radiograph 4 years later (c) demonstrates interval enlargement with an unusual morphology, with synostosis of the distal portion to the native femur, the ‘mug handle sign’
He had no relevant medical or surgical history. Examination revealed a firm and mildly tender palpable mass on the lateral aspect of the right distal thigh, at the site of previously diagnosed osteochondroma.
During the current presentation, radiographs and magnetic resonance imaging (MRI) scans were obtained to further characterise the underlying osteochondroma, and also to assess for possible complications, including malignant degeneration, particularly given the patient’s new symptoms. The radiograph revealed some interval enlargement of the osteochondroma with synostosis of the distal portion to its native femoral shaft, resulting in an unusual mug handle-like appearance [Figure 1c], the ‘mug handle sign’. There was no osseous destruction or new fracture.
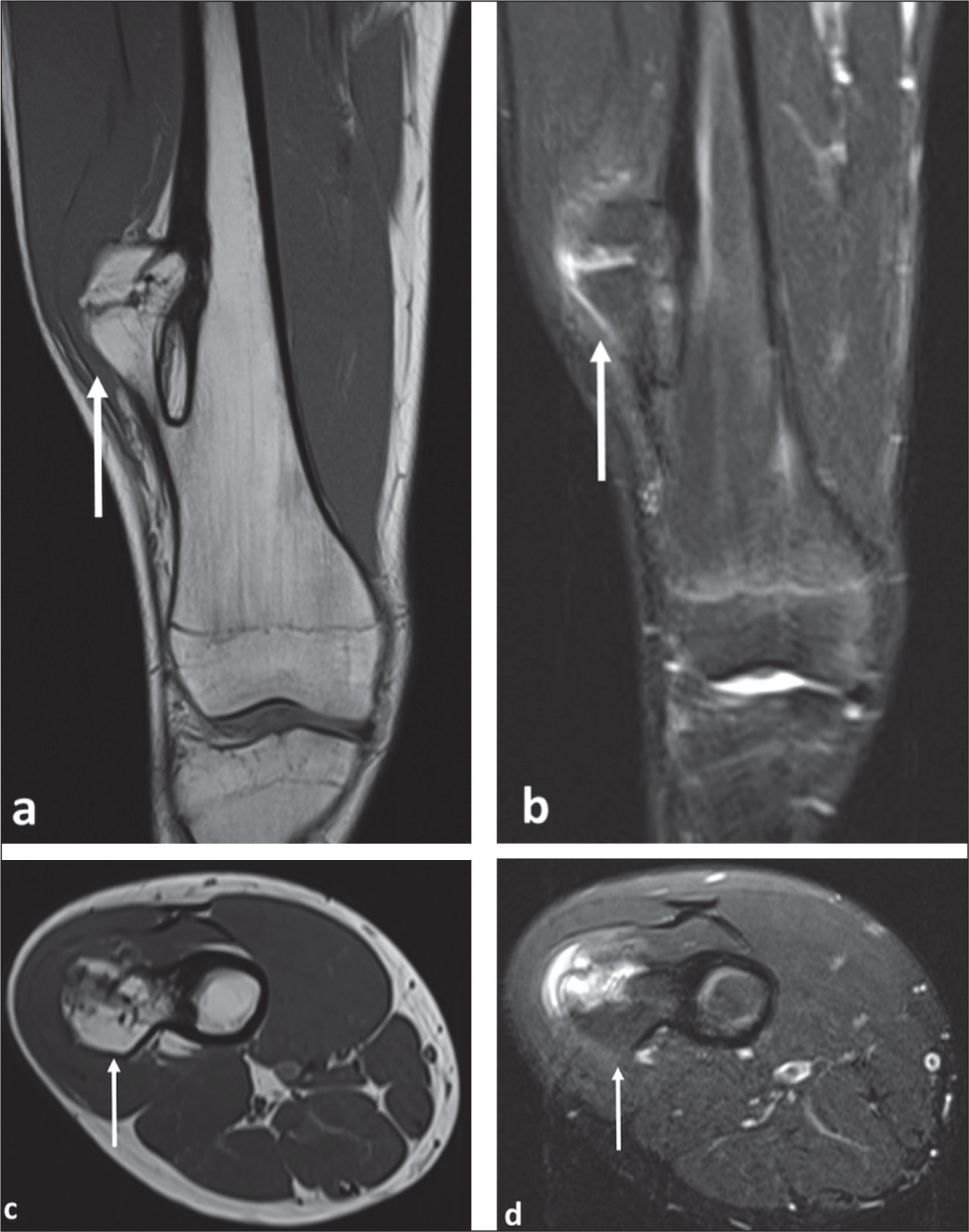
MRI revealed characteristic features of a pedunculated osteochondroma, with the pedicle of the lesion demonstrating continuity with the cortex and medullary cavity of the femur. There was a thick periosteal reaction adjacent to the pedicle, and the distal portion was fused to the femoral diaphysis a short distance superior to the pedicle [Figure 2a-2d]. The cartilage cap was of normal thickness (<15 mm), without evidence of malignant degeneration. There was also an adventitial bursa superficial to it [Figure 2c and 2d].
(a-d) Coronal T1 (a) and T2 STIR (short tau inversion recovery) (b) MR images at current presentation demonstrate unusual fusion of the distal portion of pedunculated osteochondroma to the femoral diaphysis (white arrows), with thick periosteal reaction of the adjacent femur. Axial T1 (c) and T2 STIR (d) images showing complete fusion at distal end of osteochondroma. Note the normal cartilage cap thickness and overlying adventitial bursa, latter best seen on the STIR image
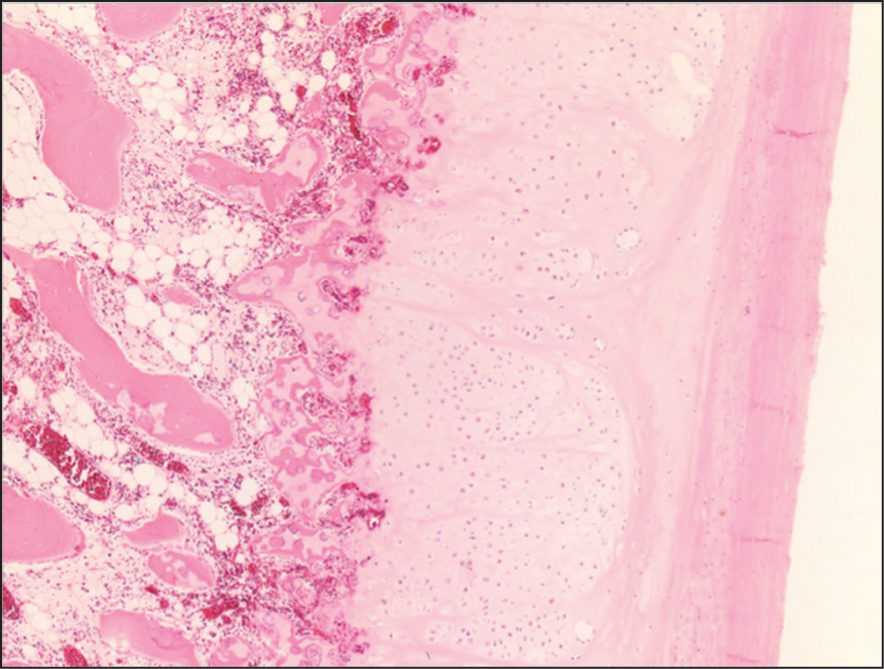
Given the clinical symptoms, which impacted the patient’s physical activity, the lesion was surgically excised. Histopathological examination of the excised specimen showed features of a benign osteochondroma composed of a hyaline cartilaginous cap, demonstrating enchondral ossification [Figure 3]. There was no evidence of malignancy.
Histopathological image of the resected osteochondroma demonstrating features of a benign osteochondroma composed of a hyaline cartilaginous cap with enchondral ossification
The patient made an uncomplicated recovery from surgery and was discharged.
Discussion
Osteochondroma is a common primary bone lesion which can either be seen in isolation (solitary) or in hereditary multiple exostoses (HME), an autosomal dominant hereditary condition arising due to mutations in the Exostosin (EXT1 or EXT2) genes.[1,4] Solitary osteochondroma can also be associated with mutations in the Exostosin 1 (EXT 1) gene, which suggests that these are benign neoplastic lesions rather than developmental lesions as previously thought.[1] They most commonly occur in the second decade of life and usually involve the metaphysis of long bones such as the tibia, femur, fibula and the humerus.[5,6]
Two morphological forms of osteochondroma are recognised: pedunculated osteochondroma, characterised by a thin pedicle connecting the lesion to the native bone, with the lesion typically pointing away from an adjacent joint, and sessile forms, which have a broad base at its attachment to the bone.[1] The classic distinguishing feature of an osteochondroma is the continuity between the cortex and medullary cavities of the host bone and the lesion, and the presence of a cartilage cap, best assessed on computed tomography (CT) or MRI.[1,7]
Several complications can arise in relation to osteochondromas, and these include deformities, fractures, vascular compromise, neurological sequelae from compression of adjacent nerves, overlying adventitial bursa formation, and malignant transformation into peripheral chondrosarcoma. The latter is seen in 1% of solitary osteochondromas and in approximately 3%–5% of patients with HME. Continued growth of the lesion and a hyaline cartilage cap thickness >15 mm after skeletal maturity are concerning for malignancy.[2] Fracture of a pedunculated osteochondroma complicated by non-union has also been previously reported.[8]
Pedunculated osteochondromas, however, are not known to fuse to the native bone, and the imaging features highlighted in our case are unusual. Davis et al. have described pressure erosion of adjacent bones as a rare complication of osteochondroma, highlighting several cases of mechanical pressure from an osteochondroma resulting in erosion of adjacent bones, as well as synostosis between two abutting, separate osteochondromas.[3] Wani et al. also described a similar case of a tibial osteochondroma causing pressure erosion of the adjacent fibula.[6] Hence, it is quite possible that a similar mechanism of pressure erosion between the distal end of a pedunculated osteochondroma and the native bone, potentially resulting from the growth of the osteochondroma, gave rise to the entity described in this article. We hypothesise that this can also be precipitated by a fracture of the osteochondroma, as was in this case. Fractures result in periosteal reaction,[9] which forms a part of the healing process. The resulting lifting of the periosteum may promote synostosis of the osteochondroma to the native bone.
Most cases of solitary osteochondromas are asymptomatic and hence do not require any active management apart from surveillance due to the low risk of malignancy.[7] It is worth noting that the presence of synostosis in isolation is not a concerning feature, as was confirmed by the histopathological analysis of the resected surgical specimen in our case. As such, the presence of this complication should not be the sole indication for surgical resection. Our patient was surgically managed due to ongoing pressure symptoms on the adjacent soft tissue, which was a significant source of pain and discomfort, and impacted his physical activity.
Conclusion
The case report highlights an unusual and previously undescribed case of synostosis of a pedunculated osteochondroma to the native bone, possibly precipitated by mechanical pressure erosion. Its unusual morphology resembling that of a mug handle may result in diagnostic uncertainty, and it is important that radiologists and clinicians recognise this entity as a benign complication of pedunculated osteochondromas.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author Rajesh Botchu is member of the Editorial Board of Apollo Medicine. The authors did not take part in the peer review or decision-making process for this submission and have no further conflicts to declare.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
N/A.
Informed consent
Consent was obtained from the patient for publication of the anonymised images.
Credit author statement
SA: Primary author involved in drafting manuscript. Performed literature search and gathered information for discussion. Prepared radiological images.
VK: Provided assistance and input with drafting manuscript and performing revisions. Liaised with patient and obtaining consent.
RT: Provided assistance and input with drafting manuscript and performing revisions. Provided idea for manuscript.
SV: Provided and reported histology images for manuscript
RB: Provided assistance and input with drafting manuscript and performing revisions. Provided idea for manuscript.
Data availability
Data can be shared on request.
Use of artificial intelligence
No.