
Abstract
Introduction:
Adenomyoepithelioma of the breast is an uncommon occurrence of breast cancer that can affect people of any age, although it most frequently affects middle-aged and older adults. It is typically found on breast imaging or manifests as a single palpable lump. On histopathology, it is a biphasic tumour that exhibits different forms of tissue metaplasia and the proliferation of the glands’ myoepithelial and epithelial components.
Case series:
This case series encompasses a huge number of 38 cases of adenomyoepithelioma during the four years. Among the 38 cases, 10 were histologically diagnosed as adenomyoepithelioma, 27 cases were adenomyoepithelial adenosis, and one case was malignant adenomyoepithelioma. Five and nine cases of adenomyoepithelial adenosis were coexistent with Phyllodes tumour and Invasive Breast carcinoma respectively.
Results:
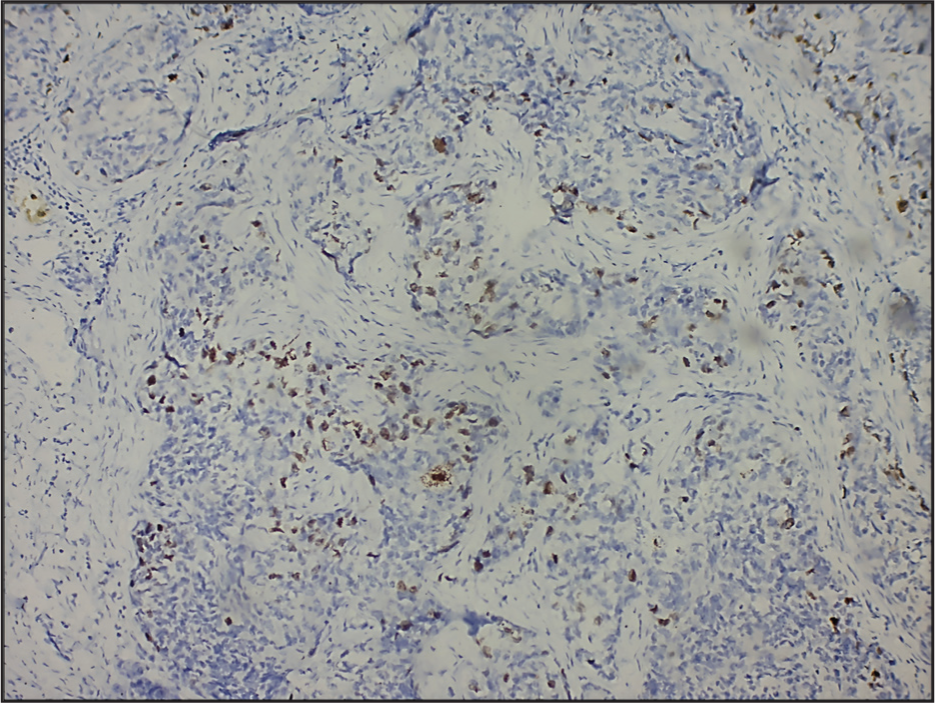
On further immunohistochemical examination, the tumour showed CK-7, p63 (nuclear positivity) and SMA (cytoplasmic positivity). Increased Ki-67 index (nuclear positivity) was present in the case of malignant myoepithelioma.
Conclusion:
This case series represents a large volume of cases compared to the available literature and throws light on the pathology of adenomyoepithelial tumours of the breast.
Introduction
The unusual breast tumour known as adenomyoepithelioma (AME) is distinguished by its ability to differentiate into luminal and myoepithelial cells. These tumours exhibit various histologic patterns, even within the regions of a single tumour. Due to the varied morphology of AMEs, it can be challenging to diagnose these lesions, primarily when a core needle biopsy is carried out. Establishing the correct diagnosis requires recognising the biphasic cellular components and the distinctive overall architecture of the tumours in conjunction with immunohistochemistry. There have been reports of local recurrences, malignant changes, and distant metastases, even though most tumours have a benign clinical course. Every case of malignant AME that has been documented has metastases, and all of them exhibit considerable cytologic atypia and quick mitotic rates. Consequently, a sufficient tumour sample is necessary to detect these characteristics.[1]
Adenomyoepithelial adenosis of the breast is an uncommon form of adenosis that resembles micro glandular adenosis, in contrast to the considerable quantity of myoepithelial cells. High proliferation in both glandular and myoepithelial components, along with a propensity for carcinomatous transformation, are characteristics of adenomyoepithelial adenosis. It may be composed of multifocal ductules distributed randomly or a lesion with a well-defined perimeter. One feature of adenomyoepithelial adenosis is the asynchronous hypertrophy and modification of epithelial and myoepithelial cells.[2,3]
Histologically, AMEs are uncommon tumours with a bicellular pattern made up of myoepithelial and epithelial cells. Even though the majority of AMEs are benign lesions, one or both of the tumour’s cellular components may convert to malignancy, as evidenced by necrosis, cytologic atypia, higher mitotic rates, and infiltrative growth patterns. The diagnostic difficulties presented by AMEs are highlighted in a case series by Parikh et al., which also underlines the need for surgical excision for a conclusive histopathologic diagnosis and the exclusion of malignancy.[4–6]
Invasive malignant myoepithelioma of the breast (MAMEB) with carcinoma (when the malignancy is caused by epithelial characteristics that resemble those of traditional invasive breast cancer) and malignant myoepithelioma (when the malignancy affects epithelial, myoepithelial, or both components). Although it has not been confirmed yet, this classification is based on their clinical and histological characteristics.[7] In terms of clinical appearance, MAMEB typically affects middle-aged women and presents as a palpable lump with a rapid development trend. In addition to its risk for distant metastasis and local recurrence, MAMEB may exhibit peripheral tissue infiltration or metastasis in various organs, including the brain, thyroid, lungs, and bones.[8,9]
Case Details
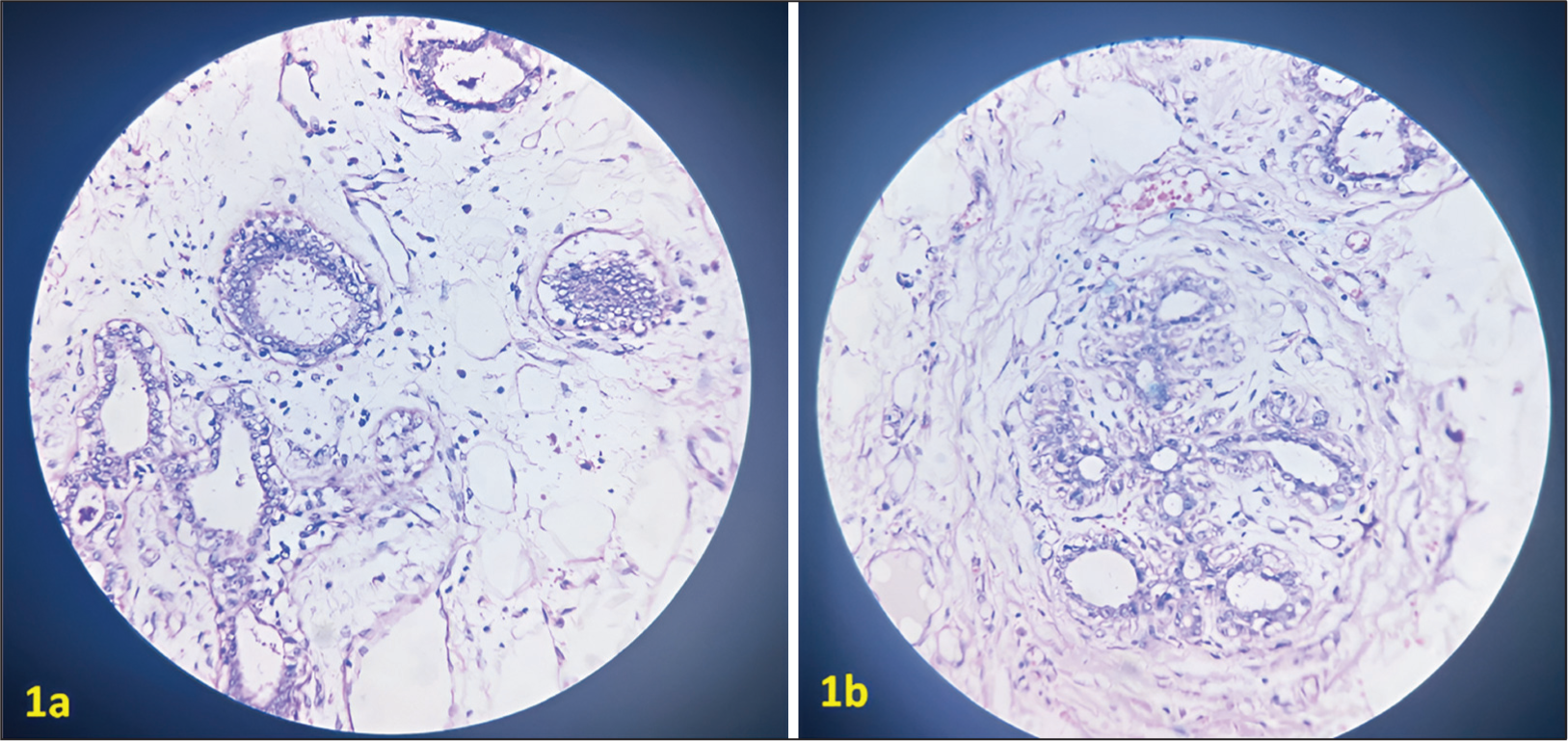
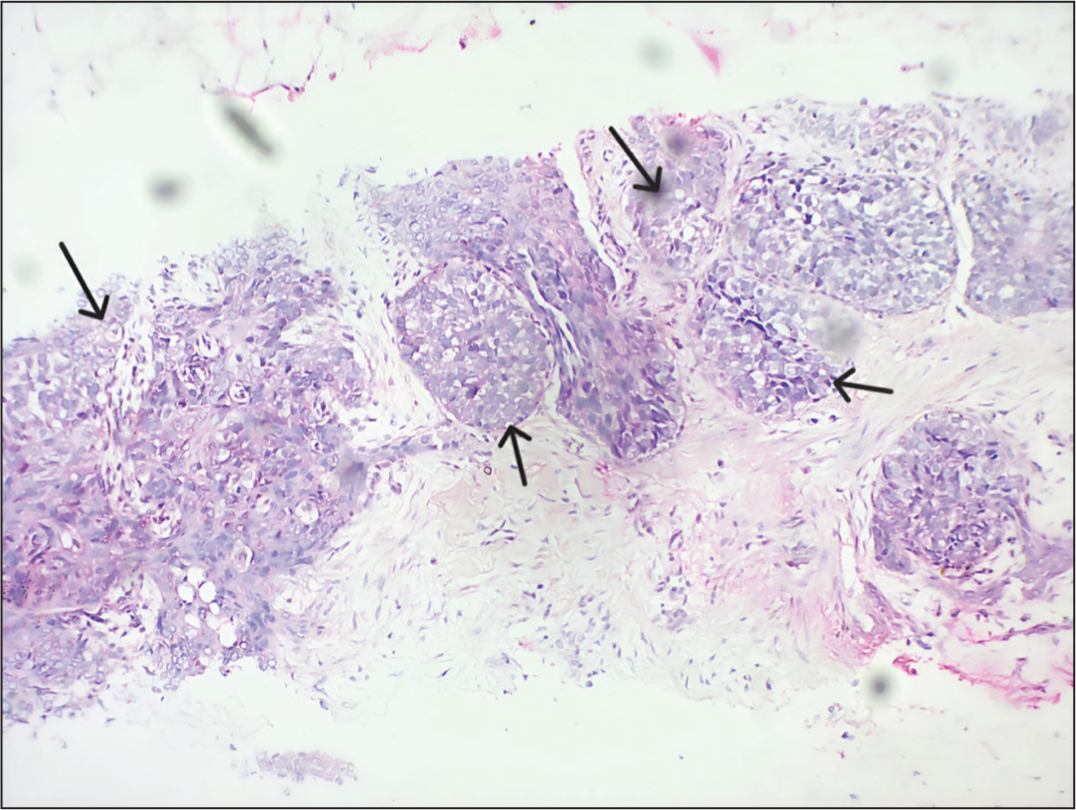
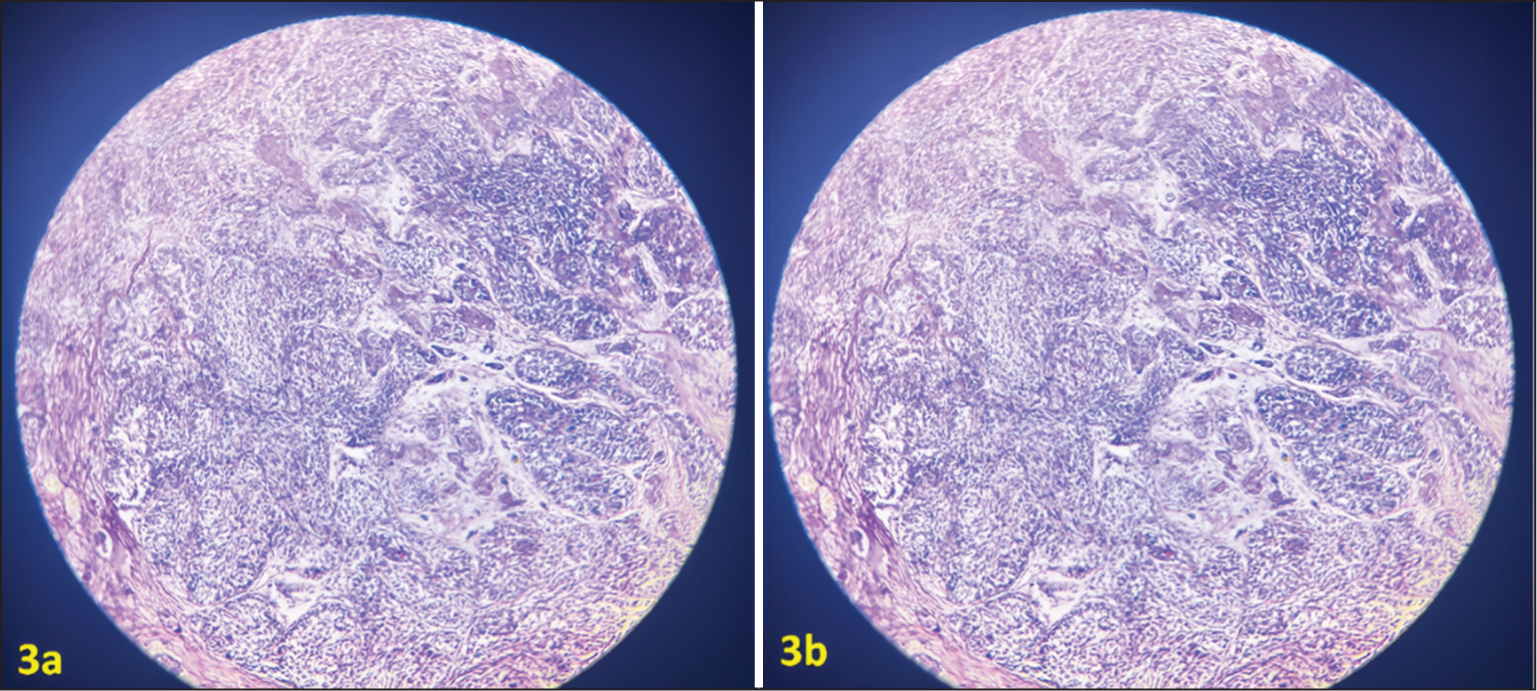
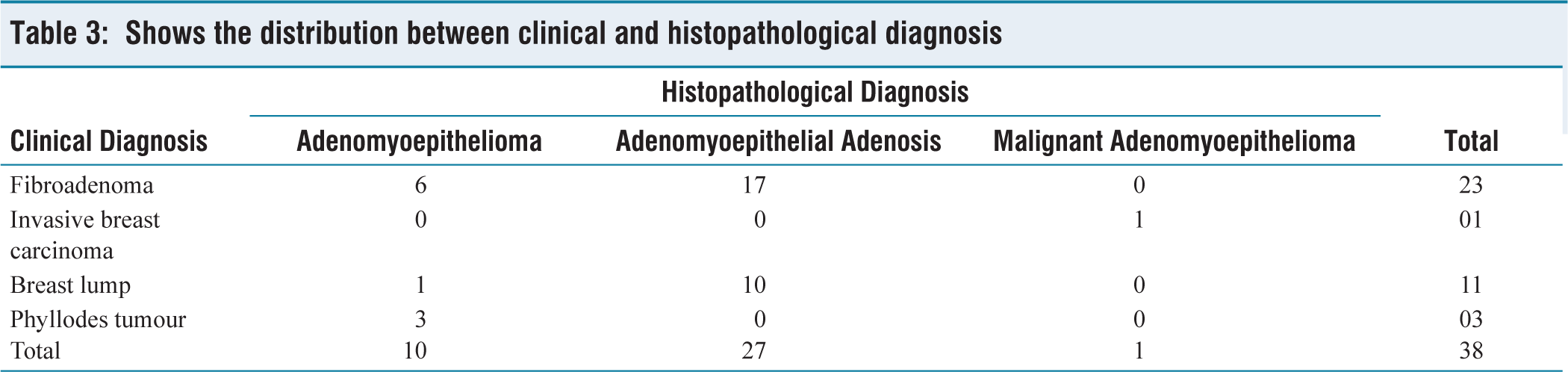
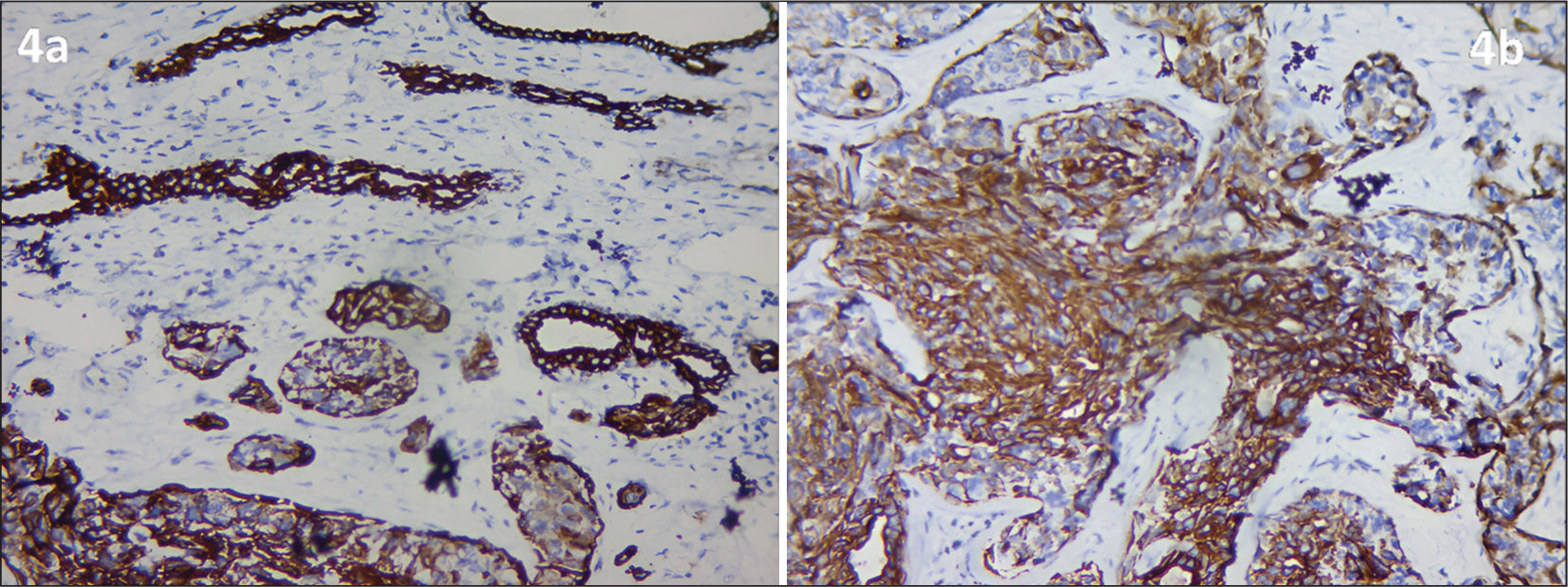
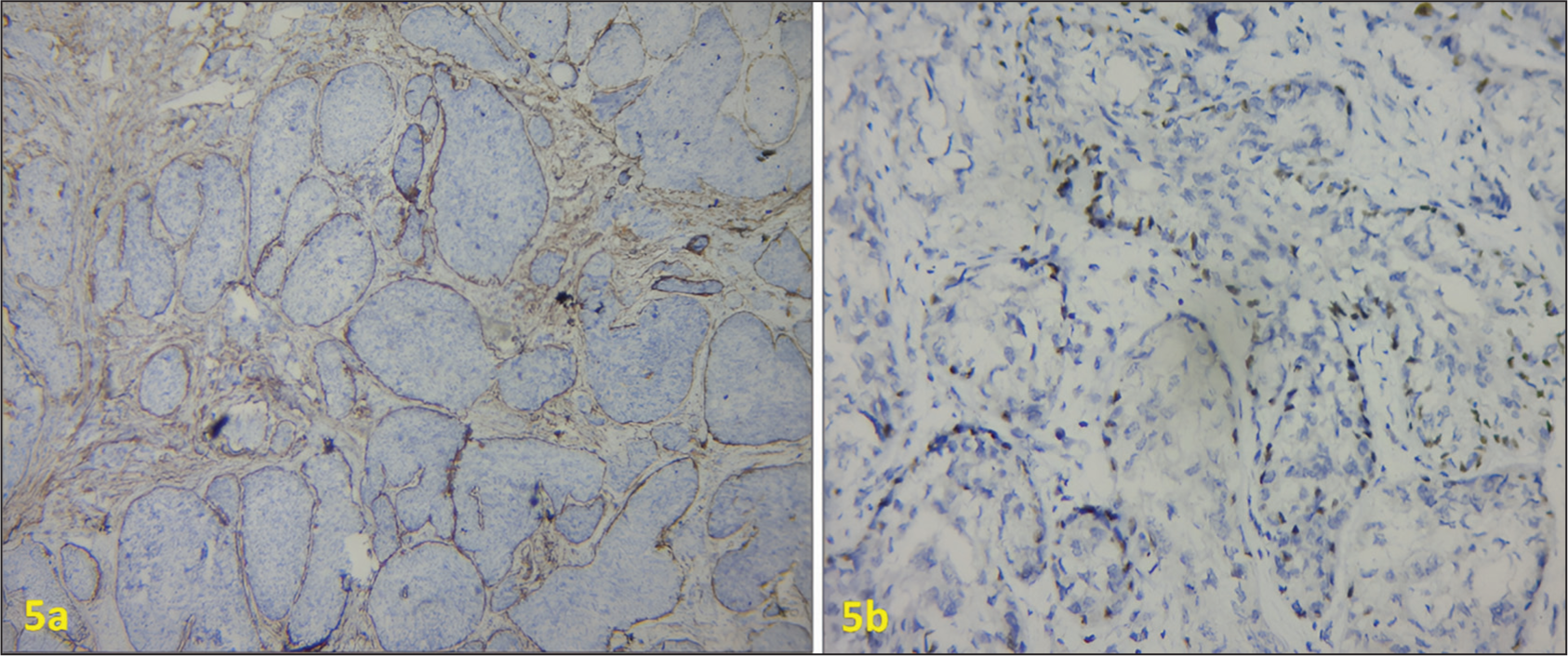
A series of 38 cases that were assessed from January 2020 to December 2024 was included in this report. These patients had a wide range of clinical diagnoses, such as fibroadenoma, invasive breast carcinoma, and phyllodes tumour, that were operated upon, and the specimens were sent to a histopathological laboratory for further evaluation and diagnosis. Out of the 38 cases, 20 were excision specimens, 6 were modified radical mastectomy specimens, 4 were simple mastectomy specimens, and 8 were excision biopsy specimens [Table 1]. Of the total 38 cases, 27 patients were diagnosed with adenomyoepithelial adenosis [Figure 1a and 1b], 10 cases came out as AME [Figure 2], and a solitary case was reported as malignant AME [Figure 3a, 3b and Table 2]. In 23 cases, the clinical diagnosis was a fibroadenoma, 11 cases had a clinical diagnosis of a breast lump, and a solitary case had invasive breast carcinoma [Table 3]. Also, these cases were assessed for co-existence with other tumours; out of the 38 cases studied, 14 cases showed co-existence with other tumours. All 14 cases were adenomyoepithelial adenosis, in which nine patients showed co-existence with invasive breast carcinoma, and five patients showed co-existence with phyllodes tumour [Table 4]. Immunohistochemistry panels for adenomyoepithelial tumours were performed in the above 38 cases and demonstrated the following findings. The epithelial component of the tumour showed CK-7 (cytoplasmic positivity) [Figure 4a and 4b], whereas the myoepithelial component of the tumour showed p63 (nuclear positivity) and SMA (cytoplasmic positivity) [Figure 5a and 5b]. Increased Ki-67 index (nuclear positivity) was present in the case of malignant myoepithelioma. [Figure 6].
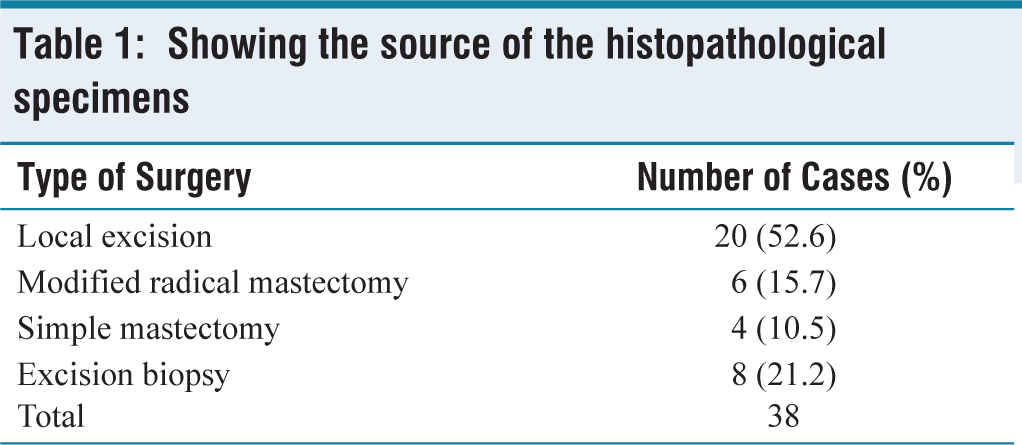
Showing the source of the histopathological specimens
(a and b) Shows adenomyoepithelial adenosis with encircled hyperplastic myoepithelial cells and cuboidal to columnar epithelial lining
Shows adenomyoepithelioma consisting of epithelial and myoepithelial components proliferating in two phases. There is a dominance of myoepithelial cells, which are polygonal with transparent cytoplasmw
(a and b) The epithelium and myoepithelial component exhibit severe atypia, a high mitotic rate and an infiltrative growth pattern. Predominance of the myoepithelial component is seen
Shows the distribution of cases among the different diagnoses

Shows the distribution between clinical and histopathological diagnosis
Shows the adenomyoepithelial tumours co-existence with other tumours

(a and b) Shows epithelial component of adenomyoepithelial tumours exhibiting CK7 Membrane and cytoplasmic positivity
(a) Shows SMA cytoplasmic positivity signifying the presence of myoepithelial component. (b) Shows p63 nuclear positivity signifying the myoepithelial component
Malignant adenomyoepithelioma showing increased Ki67 index (nuclear positivity)
Discussion
Hamperl first defined AME in 1970 as a biphasic neoplastic growth of luminal and myoepithelial cells.[10] Hamperl pointed out that the fluctuating growth of epithelial and myoepithelial cells may cause this tumour to exhibit a heterogeneous pattern. Since most tumours exhibit papillary architecture, AME is considered a subtype of intraductal papilloma.[11,12] Although benign AMEs predominate, there have been isolated reports of malignant AMEs with distant metastases.[13]
Tavassoli described three different AME variations. The first kind is the tubular pattern, distinguished by an even growth of rounded tubules and by especially prominent and hyperplastic myoepithelial cells. The second type is known as the spindle cell type, and it is made up primarily of spindled myoepithelial cells. The third type is a lobulated pattern with nests of myoepithelial cells surrounding compressed epithelial-lined spaces.[14]
In this study, it was noted that adenomyoepithelial tumours that occur in the breast could be either of the three: AME, adenomyoepithelial adenosis, or malignant AME. AMEs are found to be circumscribed, encapsulated, and lobulated. Though morphologically benign, it has high rates of recurrence.[15] AME is difficult to diagnose histologically as well. Cytology by itself is challenging to diagnose since it might be mistaken for other neoplasms. However, a core biopsy gives a more accurate diagnosis. There have been reports of a wide range of histological changes, including nodular sclerosis, sclerosing adenosis, localised adenosis, and the less frequent occurrence of calcification and cystic appearance.[16] Adenomyoepithelial adenomas are found as isolated mass lesions or are found to be associated with adjacent breast invasive carcinoma. These associations are to be considered as premalignant and to be followed up regularly. These tumours have a unique morphology of biphasic proliferation of the epithelial and myoepithelial cells. Dominant proliferation of myoepithelial cells appears as polygonal-shaped or with clear cytoplasm. They have a completely different morphology of fibroadenoma and phyllodes tumour.[17–19]
In our case series, five cases of AME resembled phyllodes tumours clinically, which differed in the predominance of the myoepithelial component over the stromal component on histopathology. Adenomyoepithelial tumours like phyllodes tumour have uncertain malignant potential and have a prognostically different course from phyllodes tumour; hence, distinguishing between both diagnoses is needed for better treatment. Five cases in this series that were clinically similar to phyllodes tumours had a high rate of recurrence; further, upon clinical and pathological follow-up, it was found to be an adenomyoepithelial tumour rather than a phyllodes tumour. This rendered the treating doctor to pave the correct line of management, which prevents future recurrence. There were similar case studies reported in the literature where AME and adenosis mimic the phyllodes tumour, which was comparable to the current series.[17,20]
On clinical examination, malignant AME and invasive breast carcinoma (ductal/lobular) are difficult to differentiate, as both can present as rapidly growing tumours in a middle-aged woman at the time of presentation. These conditions can only be differentiated and diagnosed by histopathological examination. The invasive component in malignant AME is usually myoepithelial in origin, and it will be positive for CK-7, SMA, and p63 with an increased Ki67 index, whereas in invasive breast carcinoma, it is usually ER/PR/Her2Neu positive.[21–24] In the present study, one case of clinically diagnosed invasive breast carcinoma showed CK-7, SMA, and p63 positivity with increased Ki67 index; hence, the diagnosis was confirmed to be malignant AME. In this context, a case of malignant adenomyopeithelial tumour mentioned in the current series presented as invasive breast carcinoma, and it was treated as a case of triple-negative breast carcinoma. After 1 year of follow-up, the patient had recurrence and metastasis to the axillary node, and upon further workup, it was found to be a case of malignant AME with invasive component showing CK7, SMA and P63 positivity.
In about 14 cases in the current series, we have co-existence of other tumours along with ademyoepithelioma components. Five cases were mixed with features of phyllodes tumour, and both these tumours have a high propensity to turn into malignant potential. Nine cases of invasive breast carcinoma have coexisted with AME adenosis. Hence, complete resection of adenomyoepithelial adenosis may be advised due to the risk of developing breast cancer or malignant AME and its recurrence.[25–27]
In this current era of histopathology and breast pathology, adenomyoepithelial tumours are often neglected. These tumours cannot be clinically differentiated from other common entities, such as phyllodes tumours, but prognostically, they have a different course. Hence, these entities of tumours should be clinically and histomorphologically emphasised in reducing morbidity and mortality.
Conclusion
A spectrum of lesions with varying morphologies and clinical behaviours makes up AME. The classification of AME should be further refined to guide therapy according to the available data. Classical AME is classified into benign and atypical. Clinical diagnosis of AME and its variants is very difficult to understand, as it has signs and symptoms that are similar to phyllodes and even fibroadenoma; hence, histopathological and immunohistochemical studies stand as the diagnosis of choice. Histopathological study shows proliferation of epithelial and myoepithelial components, whereas immunohistochemistry shows positivity for CK-7 (epithelial component), SMA, and p63 (myoepithelial component). Increased Ki67 index could signify malignancy, which in this context is termed malignant adenomyopeithelioma. This case series emphasises the significance of the pathological diagnosis of adenomyopeithelioma, as the tumours show a wide scope of behaviour, such as recurrence and, in rare cases, metastasis. AMEs are triple-negative tumours, and their response to chemotherapy and hormonal therapy is negligible; hence, surgical modality is the treatment of choice.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable.
Informed consent
Informed consent was obtained from the patients for the publication.
Credit author statement
All authors have reviewed the final version to be published and agreed to be accountable for all aspects of the work.
Concept and design: Dr Sathiyabama D, Dr Akash K.
Acquisition, analysis, or interpretation of data: Dr Sathiyabama D, Dr Akash K.
Drafting of the manuscript: Dr Akash K, Dr K Sathish.
Critical review and editing of the manuscript: Dr Akash K, Dr K Sathish.
Supervision: Dr Sathiyabama D, Dr Akash K, Dr K Sathish, Dr Deepana P.
Data availability
Not applicable.
Use of artificial intelligence
The authors hereby declare that Artificial Intelligence was not used in the above article.