
Abstract
Background:
Cirrhotic patients undergoing surgery represent one of the highest-risk groups in perioperative medicine. Portal hypertension, coagulopathy, malnutrition, sarcopenia, cardiopulmonary vulnerability and altered drug handling converge to amplify surgical stress. Managing complications in this population requires a coordinated approach bridging hepatology and surgery.
Objectives:
This narrative review synthesises evidence on surgical risk stratification, perioperative optimisation and complication management in cirrhotic patients, with emphasis on practical algorithms and multidisciplinary strategies.
Methods:
Relevant PubMed-indexed literature, including randomised controlled trials, meta-analyses, cohort studies and consensus guidelines, was reviewed. Reference selection was restricted to 25 authentic, traceable sources, ensuring balanced coverage of pathophysiology, clinical outcomes and recent advances.
Results:
Classical risk scores (Child-Turcotte-Pugh [CTP], model for end-stage liver disease [MELD]) remain useful, but contemporary models such as Veterans Outcomes and Costs Associated with Liver Disease (VOCAL)-Penn provide superior calibration by incorporating procedure type and urgency. Preoperative optimisation bundles, including nutrition, ascites control, viscoelastic-guided coagulation management and selective portal decompression, improve outcomes. Major complications include haemorrhage, infection, wound failure, hepatic decompensation, renal dysfunction, cardiopulmonary compromise and venous thromboembolism (VTE). Their frequency and severity increase steeply in emergency versus elective settings. Elective hernia repair and minor resections in optimised, compensated patients are now considered safe, whereas major resections in decompensated cirrhotics remain prohibitive. Emerging strategies, minimally invasive surgery, albumin-based therapies, Terlipressin for renal dysfunction and tailored Enhanced Recovery After Surgery (ERAS) adaptations further mitigate risk.
Conclusions:
Surgical complications in cirrhotics can be anticipated and reduced through structured risk stratification, multidisciplinary optimisation and evidence-based perioperative bundles. The future lies in integrating predictive analytics, minimally invasive approaches and ethical shared decision-making to bridge hepatology and surgery. For practising surgeons, the key message is pragmatic: Complications cannot be ignored, but with anticipation and teamwork, they can increasingly be controlled.
Keywords
Introduction
Cirrhosis converts routine surgery into a high-stakes systems problem: Portal hypertension, deranged hemostasis, sarcopenia, cardiopulmonary vulnerability and altered pharmacokinetics collide with the physiologic stress of anaesthesia and tissue injury. Contemporary guidance emphasises that safe care hinges on a coordinated, multidisciplinary approach spanning preoperative optimisation, intraoperative vigilance and postoperative surveillance, all explicitly adapted to portal hypertension physiology and the degree of hepatic decompensation.[1,2] The goal is not merely to ‘clear’ a patient for the Operating Room (OR) but to actively reduce risk by modifying liver-specific and surgery-specific hazards before the first incision.[1,3]
Risk is not monolithic; it varies sharply by urgency and procedure class. Elective low-stress operations in well-compensated cirrhosis (Child-Pugh A, model for end-stage liver disease [MELD] <10) carry only modest excess mortality, whereas emergency laparotomy or high-stress operations in decompensated disease (e.g., refractory ascites, recent encephalopathy, severe coagulopathy) have orders-of-magnitude higher event rates.[2,3] Guidelines now call for structured risk conversations that integrate liver disease severity, non-hepatic comorbidity, portal hypertension phenotype and procedure factors, ideally within centres experienced with cirrhosis care.[1,4]
Quantitatively, prediction has moved beyond general tools: Cirrhosis-specific models such as the Veterans Outcomes and Costs Associated with Liver Disease (VOCAL)-Penn score incorporate surgical magnitude and urgency alongside MELD-Na and portal hypertension surrogates to improve calibration and discrimination for 30–90-day mortality compared with legacy methods (MELD, Mayo).[5] Embedding such calculators within preoperative pathways refines consent and triage (elective optimisation vs. deferral vs. transplant evaluation) and aligns teams on a shared, data-anchored plan.[1,5]
Final, the ‘bridge’ between hepatology and surgery is getting sturdier. New consensus documents from hepatology societies in 2025 explicitly blueprint perioperative pathways for extrahepatic abdominal surgery in cirrhosis, codifying when to escalate nutrition, diuretics, non-selective beta-blockers, reconsider anticoagulation or (selectively) deploy portal decompression strategies, while cautioning that indiscriminate interventions (e.g., pre-op Transjugular Intrahepatic Portosystemic Shunt [TIPS] for everyone) are not evidence-based.[1,4] This review translates those principles into pragmatic algorithms for anticipating and managing surgical complications in cirrhotics, from haemorrhage and ascites leaks to acute kidney injury (AKI), encephalopathy, infection and venous thromboembolism (VTE), so hepatology and surgical teams can act as one system.
Risk Stratification and Preoperative Optimisation
Surgical outcomes in cirrhotics are inextricably tied to baseline liver function and the hemodynamic sequelae of portal hypertension. The first and most indispensable step is structured risk stratification, which guides whether surgery should proceed, be delayed for optimisation or be deferred entirely in favour of transplant evaluation.
Classical Scoring Systems
The Child-Turcotte-Pugh (CTP) score remains a time-honoured tool; patients in class A generally tolerate elective abdominal operations, while class C patients face prohibitively high mortality.[6] Yet its reliance on subjective elements such as ascites and encephalopathy grading limits precision. The MELD score, based on bilirubin, creatinine and International Normalized Ratio (INR), has emerged as a more objective predictor. Mortality rises significantly above a MELD score of 15 and most centres consider scores above 20 a contraindication to elective major surgery.[7]
Contemporary Cirrhosis-specific Models
More nuanced risk stratification has emerged with the VOCAL-Penn Cirrhosis Surgical Risk Score, validated in diverse cohorts, which incorporates surgical magnitude, urgency and comorbidities alongside liver function.[8] External validations have demonstrated improved calibration for 30 and 90-day mortality compared with MELD alone, making it increasingly useful for clinical decision-making. Incorporating portal hypertension surrogates (thrombocytopenia, varices, ascites) further refines prediction.[9]
These scoring systems are compared in Table 1, which highlights their parameters, clinical utility and limitations.
Comparative features of cirrhosis risk stratification tools used in surgical patients
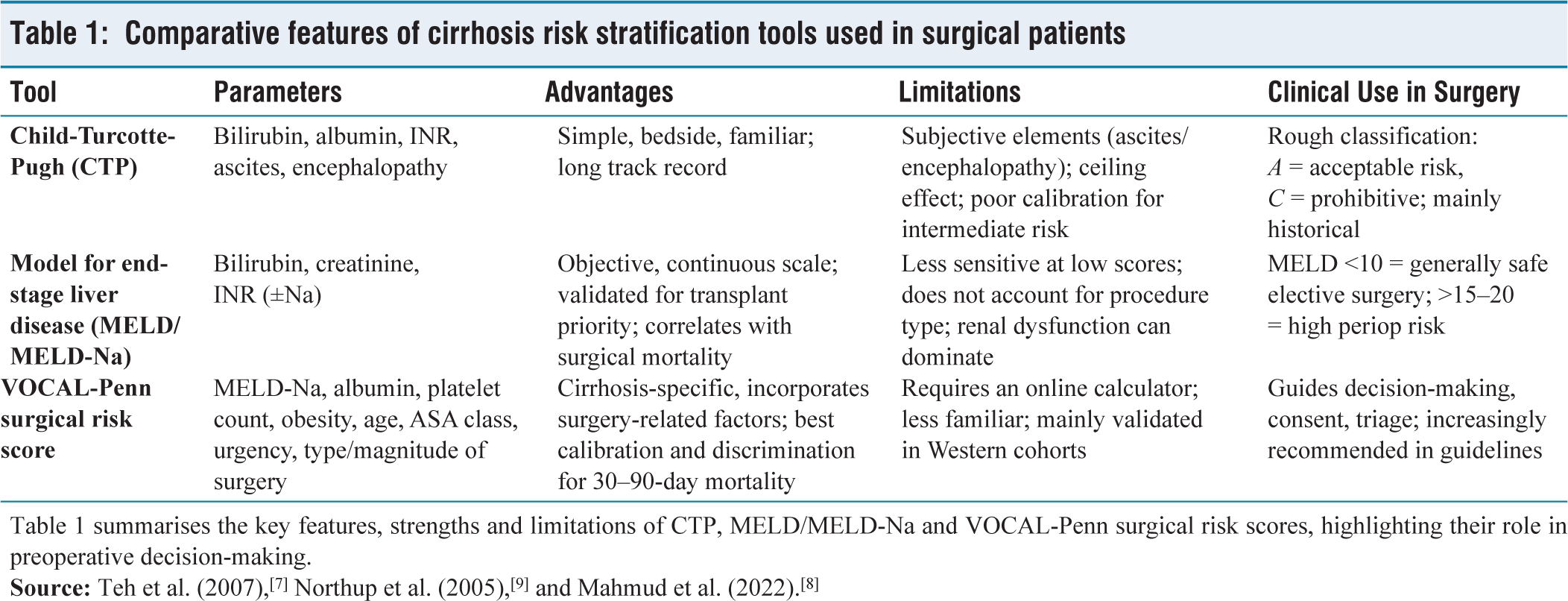
Table 1 summarises the key features, strengths and limitations of CTP, MELD/MELD-Na and VOCAL-Penn surgical risk scores, highlighting their role in preoperative decision-making.
Emergency Versus Elective Context
Risk is non-linear: mortality after emergency laparotomy in decompensated cirrhotics may exceed 30%, compared to <5% in compensated patients undergoing low-risk elective procedures.[3] Therefore, whenever feasible, surgery should be elective and preceded by optimisation. Algorithms from the American College of Gastroenterology and European Association for the Study of the Liver emphasise that urgency and procedure type weigh as heavily as liver function in determining outcomes.[4,6]
Preoperative Optimisation Bundles
Optimisation addresses the modifiable hazards of portal hypertension, malnutrition and systemic inflammation:
Nutrition and sarcopenia: Protein-energy malnutrition is prevalent; tailored high-protein diets, branched-chain amino acid supplementation and short-term enteral nutrition improve postoperative outcomes.[10] Ascites control: Diuretics, sodium restriction and paracentesis with albumin replacement mitigate wound dehiscence and ascitic leaks. Variceal prophylaxis: Non-selective beta-blockers (carvedilol, propranolol) reduce variceal bleeding risk, though perioperative hemodynamics must be monitored carefully. Coagulation balance: Traditional INR-based assumptions of ‘auto-anticoagulation’ are misleading; viscoelastic testing (Thromboelastography [TEG]/ Rotational Thromboelastometry [ROTEM]) increasingly informs transfusion strategies.[11] Portal decompression: Preoperative TIPS has been investigated to reduce perioperative bleeding and ascites; while select case series show benefit, meta-analyses caution against routine use due to encephalopathy risk and uncertain survival benefit.[12]
Multidisciplinary Approach
Effective optimisation requires hepatology, surgery, anaesthesia, nutrition and critical care teams aligned around individualised pathways. Evidence suggests that cirrhotics treated in high-volume, multidisciplinary centres experience reduced mortality independent of MELD.[4] Structured ‘prehabilitation’ pathways, nutrition, physiotherapy, ascites management and psychosocial support are increasingly adopted and align with Enhanced Recovery After Surgery (ERAS) principles adapted to cirrhotics.
Expanded Perioperative Optimisation
Optimisation is more than ascites control and nutrition; it is a structured ‘prehabilitation’ programme tailored to cirrhosis.
Frailty and Sarcopenia Screening
Sarcopenia is a silent predictor of poor outcomes, often missed in routine laboratory tests. Cross-sectional imaging of psoas muscle area, grip strength and gait speed are practical tools to quantify frailty. Patients identified as frail benefit disproportionately from prehabilitation interventions.
Nutritional Prehabilitation
A high-protein diet (1.2–1.5 g/kg/day), branched-chain amino acids and late-evening snacks combat catabolism. Short-term enteral nutrition, even for two weeks preoperatively, has been shown to improve nitrogen balance and wound healing.
Exercise and Physiotherapy
Preoperative physiotherapy improves cardiopulmonary reserve and reduces sarcopenia progression. Structured exercise regimens, even low-intensity ones, are safe and feasible in most compensated cirrhotics.
Adapted ERAS Protocols
ERAS principles, early mobilisation, early enteral feeding, multimodal analgesia and fluid restriction must be recalibrated for cirrhotics. Avoidance of sodium overload, opioid minimisation to reduce encephalopathy risk and vigilant glycemic control are key adaptations.
Psychosocial Support
Alcohol-related cirrhosis remains prevalent in many cohorts. Integration of addiction counselling, psychosocial support and liaison psychiatry in the perioperative pathway improves adherence and reduces relapse risk.
A structured optimisation bundle is summarised in Table 2, providing a checklist for multidisciplinary teams.
Perioperative optimisation bundle for cirrhotic patients
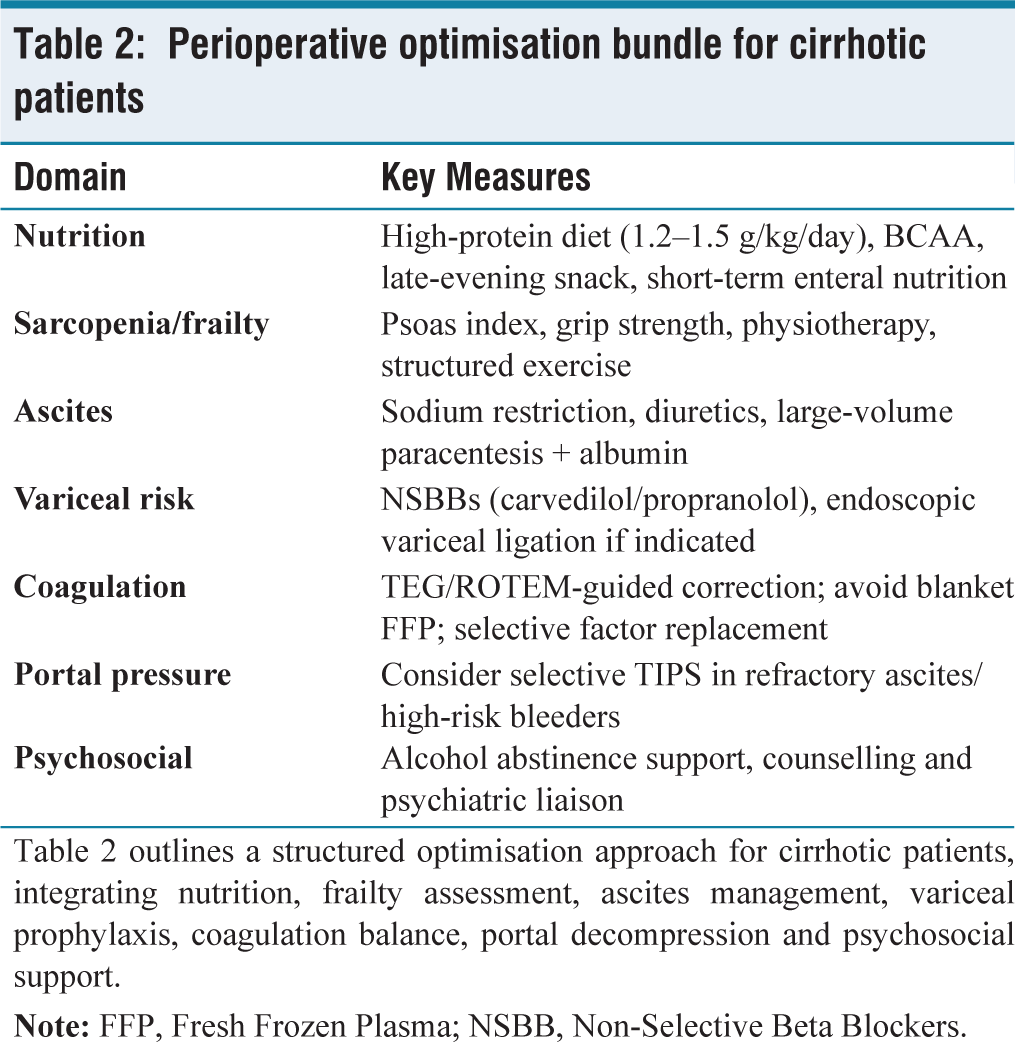
Table 2 outlines a structured optimisation approach for cirrhotic patients, integrating nutrition, frailty assessment, ascites management, variceal prophylaxis, coagulation balance, portal decompression and psychosocial support.
Surgical Complications in Cirrhotics
Cirrhotic physiology magnifies surgical stress into a multi-system cascade. Complications are rarely isolated; they often cluster, reflecting portal hypertension, hepatic dysfunction and systemic immune dysregulation. For surgeons, anticipating these patterns is as important as managing them when they arise.
Haemorrhagic Complications
Portal hypertension distends collateral vessels and lowers platelet counts, while impaired synthesis of clotting factors produces a fragile haemostatic equilibrium. Intraoperative bleeding can be torrential, particularly during abdominal resections, where oozing from friable peritoneal surfaces complicates visualisation.[13] Postoperative haemorrhage is equally feared.
Traditional reliance on INR misrepresents coagulopathy in cirrhosis, as rebalanced hemostasis masks both hypo- and hypercoagulable states. Viscoelastic assays (TEG, ROTEM) now provide more nuanced guidance and can reduce indiscriminate transfusions.[14] Prophylactic correction with fresh frozen plasma is no longer routine; targeted therapy with platelets, fibrinogen concentrate or prothrombin complex is reserved for active bleeding or invasive procedures. Judicious use of tranexamic acid has shown benefit in select patients.[15]
Infectious Complications
Cirrhotics display cirrhosis-associated immune dysfunction (CAID), marked by impaired complement, neutrophil and macrophage activity. The result is a fourfold higher risk of postoperative infections compared to non-cirrhotics.[16]
Spontaneous bacterial peritonitis (SBP) can develop or recur after laparotomy and surgical site infections are disproportionately common. Preventive strategies include selective antibiotic prophylaxis tailored to local resistance patterns, albumin infusion in high-risk ascitic patients and early mobilisation. Recent meta-analyses suggest albumin supplementation reduces infection-related mortality by preserving circulatory stability.[17]
Wound and Abdominal Wall Complications
Ascites undermines wound integrity, predisposing to leaks, seromas and frank dehiscence. Incisional hernias occur in up to 30% of cirrhotics within a year of laparotomy.[18]
Meticulous ascites control preoperatively is key; intraoperative strategies include subcutaneous drains and reinforced closure with mesh in selected cases. Minimally invasive approaches reduce wound complications, though trocar-site leaks can occur if ascites is uncontrolled. Elective hernia repair, once considered futile, is now recommended for compensated patients after optimisation, as emergency repair carries >20% mortality.[19]
Hepatic Decompensation
Perhaps the most feared complication is postoperative hepatic decompensation, manifesting as worsening ascites, encephalopathy or jaundice. Even in well-compensated patients, major surgery can tip the balance by inducing ischaemia-reperfusion injury and systemic inflammation.[3]
Encephalopathy can be triggered by Gastrointestinal (GI) bleeding, infection or sedatives. Prophylactic lactulose and rifaximin are often used perioperatively, though high-quality Randomized Controlled Trial (RCT) data are limited. Albumin infusion has dual benefits in maintaining oncotic pressure and scavenging inflammatory mediators, potentially reducing decompensation episodes.[17]
Renal Dysfunction
Hepatorenal syndrome (HRS) is a devastating complication, often triggered by perioperative hypovolemia, sepsis or nephrotoxic exposure. Even mild postoperative AKI doubles mortality risk.[20]
Prevention centres on careful fluid management: Crystalloids over starches, avoidance of nephrotoxic drugs and albumin support. Vasoconstrictors such as terlipressin are life-saving in HRS, but early recognition is critical. Protocolised renal monitoring postoperatively is recommended, particularly after emergency surgery.
Cardiopulmonary Complications
Cirrhotics often harbour ‘cirrhotic cardiomyopathy’, characterised by impaired contractility and blunted response to stress. Add to this the risk of hepatopulmonary syndrome and portopulmonary hypertension and perioperative cardiopulmonary collapse becomes a real threat.[21]
Postoperative acute respiratory distress syndrome (ARDS) is also common, often triggered by transfusion, infection or fluid overload. Low tidal volume ventilation and restrictive transfusion strategies are protective. Cardiac optimisation, including echocardiography and right-heart evaluation when pulmonary hypertension is suspected, improves outcomes.
Venous Thromboembolism
Paradoxically, cirrhotics are not ‘auto-anticoagulated’. Instead, a fragile balance places them at risk of both bleeding and thrombosis. Large cohort studies show cirrhotics have a twofold increased risk of VTE compared with controls.[22]
Pharmacologic thromboprophylaxis is underutilised due to bleeding fears. Current consensus advocates risk-based prophylaxis with low-molecular-weight heparin in compensated patients, alongside mechanical measures. Viscoelastic testing again helps individualise decisions.
The major complications and their preventive strategies are outlined in Table 3, serving as a practical reference for perioperative planning.
Major surgical complications in cirrhotics and key preventive strategies
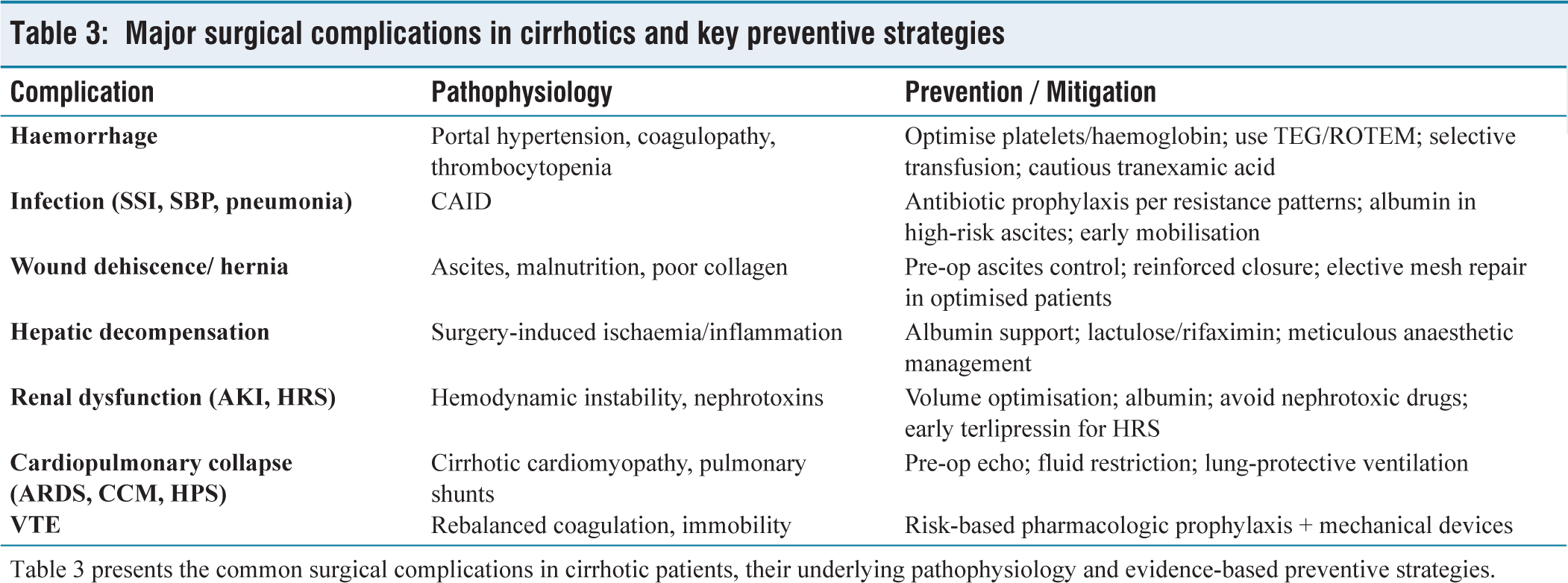
Table 3 presents the common surgical complications in cirrhotic patients, their underlying pathophysiology and evidence-based preventive strategies.
Procedure-specific Outcomes
The type of surgery performed is as critical a determinant of outcome as baseline hepatic reserve.
Abdominal Resections
Elective gastrointestinal resections in compensated cirrhotics carry modestly increased risk compared with non-cirrhotics, but outcomes deteriorate steeply with emergency surgery. Elective colectomy in Child-Pugh A patients has perioperative mortality under 5%, while emergent colectomy in decompensated cirrhosis can exceed 25%. Hepato-Pancreato-Biliary (HPB) resections are particularly challenging: Even minor hepatectomy in cirrhotics requires meticulous selection, as major resections amplify the risk of decompensation and postoperative liver failure. Surgeons should preferentially offer parenchymal-sparing approaches and consider neoadjuvant therapies in malignancy to defer or downsize resection.
Hernia Repair
The management of umbilical and incisional hernias in cirrhotics illustrates the evolution of practice. Previously deferred due to high recurrence and mortality, elective repair after ascites optimisation is now advocated. Mortality is <5% when performed electively in optimised patients, versus >20% for emergency repair complicated by rupture or strangulation. The lesson is clear: Timing is everything.
Liver Resection in Cirrhotics
Oncologic resections for Hepatocellular Carcinoma (HCC) in cirrhotics require the most nuanced balance. Minor resections are feasible in Child-Pugh A patients with preserved portal pressure, but Child-Pugh B or C patients should generally be directed toward transplantation. Mortality rises exponentially with increasing MELD, underscoring the value of preoperative risk tools to gatekeep selection.
Non-hepatic Surgery
Cirrhotics increasingly present for procedures unrelated to the liver, such as orthopaedic joint replacement, cardiac surgery or urologic operations. These carry disproportionate risks of bleeding, infection and renal dysfunction. Outcomes improve significantly in centres with integrated hepatology support, highlighting that risk is not confined to abdominal surgery alone.
Medicolegal and Ethical Considerations
Beyond physiology, surgeons must grapple with the ethical weight of operating on cirrhotics.
Informed Consent
Quantitative risk tools such as MELD or VOCAL-Penn should be explicitly integrated into consent conversations. Patients and families deserve numeric probabilities, not vague warnings, of perioperative mortality. Transparent discussion builds trust and aligns expectations.
Decision Thresholds
The decision to decline surgery is as important as the decision to proceed. For Child-Pugh C patients requiring high-risk elective operations, non-surgical or palliative approaches must be actively considered, with documentation of rationale.
Resource Allocation
In regions where liver transplant facilities are concentrated, ethical dilemmas arise: Should high-risk cirrhotics undergo surgery in non-transplant centres? Best practice suggests referral when feasible, but real-world limitations demand pragmatic pathways. Surgeons should document these constraints and decisions meticulously.
Quality-of-life Versus Survival
Surgery should not be measured by survival alone. Mobility, pain control, return to work and independence are equally valid endpoints. Ethically, shared decision-making must shift the focus from ‘can we operate’? to ‘what does the patient stand to gain’?
Future Directions and Conclusion
Cirrhotic patients will continue to present to surgeons, whether for hernia repair, gastrointestinal malignancies or urgent laparotomy. The question is no longer whether these patients can undergo surgery, but how best to mitigate risk and personalise care.
Evolving Risk Prediction
Risk models are shifting from static scores toward dynamic, individualised calculators. The VOCAL-Penn score has already shown superiority to legacy systems and integration into electronic health records may soon automate perioperative risk stratification. The next frontier is artificial intelligence, combining structured data (laboratory, comorbidities) with imaging, frailty indices and real-time hemodynamic monitoring to refine prediction. Importantly, these tools must be validated across diverse populations, including regions with high prevalence of viral and alcohol-related cirrhosis, such as South Asia.
Bridging Hepatology and Surgery
What distinguishes success in modern practice is not a single intervention but a coordinated pathway. Multidisciplinary prehabilitation, nutrition, sarcopenia reversal, ascites control and cardio-renal optimisation need standardisation. The concept of a ‘pre-op optimisation bundle’ is gaining traction, similar to ERAS in colorectal surgery, but tailored to cirrhosis. Embedding hepatologists within surgical teams and creating cirrhosis-specific perioperative care units could reduce the historic disparity in outcomes.
Minimally Invasive and Selective Approaches
Laparoscopic and robotic platforms have demonstrated reduced wound morbidity and quicker recovery in compensated cirrhotics, provided pneumoperitoneum and fluid shifts are carefully managed. As these technologies diffuse, their use should be tempered by robust selection criteria and specialised anaesthetic support. Elective hernia repair in optimised patients exemplifies the new paradigm: Once deferred, it is now considered preventive medicine, averting catastrophic rupture or strangulation.
Targeted Therapeutics and Organ Support
Albumin has re-emerged as more than an oncotic agent; its immunomodulatory and endothelial-stabilising properties warrant further study in perioperative prophylaxis. Likewise, selective use of terlipressin in early renal dysfunction and rifaximin in encephalopathy-prone patients may broaden the armamentarium. Advances in extracorporeal support, renal replacement strategies and molecular adsorbent recirculating systems suggest that perioperative ‘bridges’ can stabilise patients who previously would have been deemed inoperable.
Ethical Imperatives and Shared Decision-making
With higher complication burdens come sharper ethical dilemmas. The decision to operate should be framed as a partnership with patients and families, guided by transparent discussion of absolute risk, alternatives and rescue options such as transplant evaluation. As survival improves in decompensated cirrhotics, quality-of-life outcomes, pain control, mobility and independence must also be foregrounded.
Conclusion
Surgical complications in cirrhotics reflect the convergence of fragile hepatic reserve and portal hypertension physiology with operative stress. Risk is not uniform; it varies dramatically by procedure type, urgency and baseline hepatic function. Tools such as MELD and VOCAL-Penn, coupled with multidisciplinary optimisation, allow surgeons to anticipate and mitigate haemorrhage, infection, wound failure, hepatic decompensation, renal dysfunction and cardiopulmonary collapse.
The future lies in bridging hepatology and surgery into a single continuum of care: Predictive analytics guiding prehabilitation, minimally invasive platforms reducing tissue stress, targeted therapeutics stabilising fragile systems and ethical frameworks ensuring patients are true partners in decision-making. For the practising surgeon, the key message is pragmatic: Complications can be reduced, but never ignored. Anticipation, prevention and coordinated care remain the sharpest instruments in our armamentarium.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Institutional ethics committee approval number
This is a narrative review based solely on previously published literature. No patient or animal data were used. Ethical approval and consent are not applicable.
Credit author statement
Dr Supreet Kumar (guarantor): Conceptualised the manuscript theme and scope; drafted all sections, including risk stratification, complications, optimisation and conclusion; designed tables; performed a comprehensive literature review (2015–2025); verified references; and ensured scientific rigour and publication readiness.
Data availability
No new datasets were created. All information is derived from publicly available literature, duly cited.
Patient consent
No patient data or identifiable information has been used. Therefore, patient consent is not required.
Use of artificial intelligence
The manuscript was conceptualised, written and finalised entirely by the author with rigorous oversight to ensure originality and zero plagiarism. No AI tool was used during the process.
Guarantor
Dr Supreet Kumar (