
Abstract
Background and Aims:
Uncontrolled haemorrhage remains a leading cause of preventable mortality following traumatic injury. Orthopaedic trauma—particularly injuries involving the pelvis, femur, and complex extremity wounds—contributes substantially to exsanguination and early trauma-related deaths.
Objectives:
This narrative review aims to describe the evolution of massive transfusion protocols (MTPs) from military to civilian trauma care, examine their integration into orthopaedic trauma practice, and outline future directions in haemorrhage control and resuscitation science.
Methods:
A narrative review of the literature was conducted focusing on the development of MTPs during recent military conflicts and their subsequent adaptation to civilian trauma systems, with particular emphasis on implications for orthopaedic trauma management.
Results:
Over the past two decades, MTPs have transformed trauma resuscitation by promoting early balanced transfusion strategies using predefined ratios of red blood cells, plasma, and platelets. These approaches have replaced earlier practices dominated by crystalloid resuscitation and delayed plasma administration. In orthopaedic trauma, early haemorrhage control and damage control orthopaedics have become integral components of damage control resuscitation. Battlefield-derived principles have expanded the role of the orthopaedic surgeon beyond skeletal stabilisation to include active participation in haemorrhage management within multidisciplinary trauma teams.
Conclusions:
The translation of military resuscitation strategies into civilian practice has significantly influenced modern orthopaedic trauma care. MTPs have reinforced the central role of orthopaedic surgeons in early haemorrhage control and interdisciplinary trauma management. Ongoing refinements in resuscitation strategies and transfusion science are expected to further optimise outcomes in patients with severe orthopaedic injuries.
Introduction
Trauma is a global public health crisis, accounting for more than five million deaths annually, with haemorrhage responsible for a significant proportion of preventable fatalities. Within the domain of trauma, orthopaedic injuries hold a unique position because of their frequent association with massive blood loss.[1] Pelvic ring disruptions, femoral shaft fractures, and mangled extremities are notorious for producing exsanguinating haemorrhage that can overwhelm the body’s compensatory mechanisms within minutes. Historically, the focus of orthopaedic surgeons was on stabilising fractures, restoring anatomy, and salvaging limbs, often with little involvement in the systemic resuscitative process. However, as evidence accumulated from both military and civilian conflicts, it became apparent that survival hinged not only on operative fixation but also on integrated haemorrhage control strategies that included transfusion science.[2]
The modern concept of massive transfusion protocols (MTPs) emerged from lessons learned on the battlefield, where young, otherwise healthy soldiers sustained devastating blast and gunshot injuries. These injuries frequently involved extensive orthopaedic trauma, pelvic disruptions, and multiple long-bone fractures complicated by vascular injuries. Traditional resuscitation, heavily dependent on crystalloids and unbalanced red blood cell transfusion, resulted in dilutional coagulopathy, acidosis, hypothermia, and high mortality rates. In response, military surgeons pioneered balanced transfusion strategies that sought to replicate whole blood by delivering red blood cells, plasma, and platelets in near-equal proportions. These approaches were later codified into structured MTPs, which transformed trauma care not only in warzones but also in civilian trauma centres worldwide.[3]
The central role of orthopaedic trauma in driving haemorrhage highlights the importance of this topic. Understanding MTPs is essential for orthopaedic surgeons, who are often called upon to stabilise bleeding fractures, apply external fixators, control junctional haemorrhage, or coordinate with general and vascular surgeons in the damage control sequence. This review aims to narratively explore the evolution, principles, and applications of MTPs in orthopaedic trauma, tracing their battlefield origins and analysing their current and future roles in both civilian and military practice.[4]
Methods
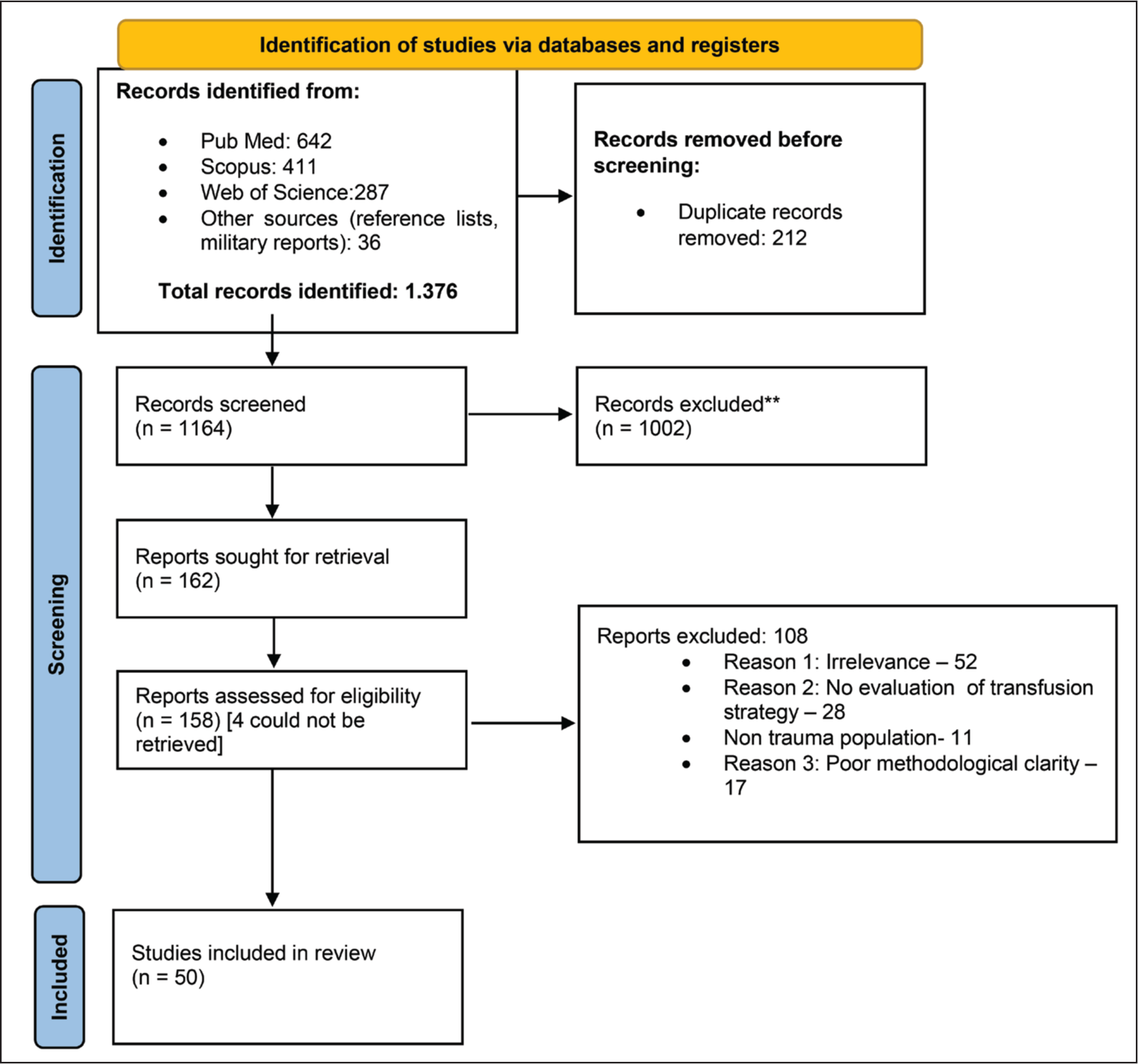
This review synthesises literature spanning the last two decades, focusing on the evolution, implementation, and outcomes of MTPs in trauma and their particular relevance to orthopaedic injuries. Databases including PubMed, Scopus, and Web of Science were searched for publications from 2000 to 2025. Keywords included ‘massive transfusion’, ‘orthopaedic trauma’, ‘pelvic fracture haemorrhage’, ‘battlefield transfusion’ and ‘damage control resuscitation’. Studies were selected if they discussed either the development of MTPs in military conflicts or their application to orthopaedic trauma scenarios in civilian settings. Both randomised controlled trials and observational studies were included, alongside systematic reviews and narrative analyses. Military reports, registry data, and trauma system reviews were also incorporated, given their significant role in shaping MTP concepts. This narrative synthesis avoids statistical meta-analysis but instead integrates the historical context, clinical practice changes, and emerging strategies to create a comprehensive review. The PRISMA flow diagram for this review is mentioned in Figure 1.
PRISMA
Evolution of MTPs: From Battlefield to Civilian Trauma
Before the widespread adoption of MTPs, trauma resuscitation followed a ‘rescue with fluids’ paradigm, where crystalloid solutions such as normal saline and Ringer’s lactate were given in large volumes to restore blood pressure. Blood products, particularly plasma and platelets, were administered sparingly and often late in the resuscitation process, long after red blood cell transfusion had begun. This approach often exacerbated coagulopathy, diluted clotting factors, and worsened acidosis. The outcomes were poor, with mortality in massively transfused trauma patients exceeding 50% in many series.[5]
Military physicians confronted unprecedented numbers of young soldiers with catastrophic blast injuries from improvised explosive devices (IEDs). These injuries were characterised by multiple amputations, open fractures, and pelvic disruptions—injuries that bled profusely and demanded immediate resuscitation.[6] Observational data from military hospitals showed that patients receiving high ratios of plasma and platelets to red cells had improved survival compared to those given red cells alone. These findings drove the adoption of balanced transfusion strategies, where red blood cells, plasma, and platelets were administered in approximately 1:1:1 ratios. This approach sought to replicate the haemostatic profile of whole blood, which had been the standard during earlier conflicts but was abandoned with the advent of component therapy.[7]
In addition to product ratios, military resuscitation also emphasised damage control principles. The concept of damage control resuscitation (DCR) emerged, encompassing permissive hypotension, minimisation of crystalloid, prevention of hypothermia, and rapid control of haemorrhage. Orthopaedic strategies such as pelvic binders, tourniquets, and early external fixation of long bones were integrated into DCR as essential steps to control bleeding and stabilise the patient physiologically.[8] The lessons learned from military conflicts were rapidly translated into civilian trauma systems, where Level I trauma centres formalised MTPs with activation criteria, product ratios, and multidisciplinary coordination. The pivotal PROPPR trial later confirmed the benefits of balanced resuscitation in reducing exsanguination deaths, solidifying the evidence base for civilian adoption.[9]
Principles of Modern MTPs
Modern MTPs are built on the concept of delivering balanced haemostatic resuscitation in the earliest phases of trauma care. Activation typically occurs when patients present with signs of severe haemorrhage or when predictive scores such as the Assessment of Blood Consumption (ABC score) indicate a high likelihood of requiring massive transfusion. Once activated, the protocol ensures immediate delivery of blood products in predefined packs containing red cells, plasma, and platelets, which are transfused simultaneously rather than sequentially.[10]
The cornerstone principle is the 1:1:1 ratio, designed to mimic the haemostatic properties of whole blood. Plasma provides clotting factors, platelets restore primary haemostasis, and red cells restore oxygen delivery. This strategy addresses trauma-induced coagulopathy, which can occur within minutes of injury and is worsened by dilution and hypothermia. Calcium supplementation is a critical adjunct, as citrate in stored blood products can cause profound hypocalcaemia, impairing both cardiac contractility and coagulation. Similarly, aggressive warming strategies are employed to prevent hypothermia, which exacerbates coagulopathy.[11]
Antifibrinolytics such as tranexamic acid (TXA) are incorporated early, particularly within 3 hours of injury, based on evidence of mortality reduction in major bleeding.[12] Viscoelastic assays, including thromboelastography and rotational thromboelastometry, are increasingly used to guide targeted transfusion beyond empiric ratios, allowing clinicians to tailor therapy to the patient’s specific coagulation profile. Collectively, these principles have shifted resuscitation from a reactive to a proactive model, with predefined protocols ensuring rapid delivery and coordinated team response.[13]
Orthopaedic Trauma and Haemorrhage Control
Orthopaedic injuries are among the most haemorrhage-prone in trauma. Pelvic fractures can disrupt both arterial and venous structures, leading to exsanguination into the retroperitoneal space. Long-bone fractures such as femoral shaft injuries may bleed up to 1.5 litres internally, while bilateral femoral fractures can result in fatal losses if not rapidly controlled. In addition, extremity trauma from high-energy mechanisms or battlefield injuries can involve vascular disruption, soft-tissue devastation, and junctional haemorrhage, all of which complicate resuscitation.[14]
On the battlefield, innovations in haemorrhage control revolutionised outcomes. The widespread use of tourniquets dramatically reduced deaths from extremity bleeding. Far from causing the feared complications of ischaemia, early and proper tourniquet application saved thousands of lives.[15] Haemostatic dressings impregnated with agents that accelerate clotting were also deployed effectively in junctional and extremity wounds.[16] For pelvic fractures, rapid application of pelvic binders or improvised sheets provided immediate mechanical stabilisation, reducing pelvic volume and tamponading venous bleeding. These principles have translated into civilian practice, where emergency responders and trauma teams now employ tourniquets and pelvic binders routinely in prehospital care.[17]
Orthopaedic surgeons play a central role in definitive haemorrhage control. External fixation of long bones not only stabilises fractures but also reduces bleeding surfaces and venous oozing. In unstable pelvic fractures, external fixators or pelvic C-clamps provide temporary but life-saving stabilisation until definitive fixation can be achieved.[4] In hospital settings, preperitoneal pelvic packing and angioembolisation complement orthopaedic interventions, forming a multidisciplinary approach to haemorrhage control. Damage control orthopaedics (DCO), which prioritises rapid external fixation and defers definitive surgery, aligns seamlessly with MTP-driven resuscitation, minimising operative stress in physiologically unstable patients.[18]
Evidence from Literature
Evidence supporting MTPs has steadily grown over the past two decades. Observational studies from military registries consistently demonstrated survival benefits associated with high plasma and platelet ratios. Civilian trauma centres subsequently confirmed these findings, with multiple cohort studies showing reduced mortality in patients managed with structured MTPs compared to ad hoc transfusion.[19] The landmark PROPPR trial, a large multicentre randomised study, compared 1:1:1 ratios with 1:1:2 strategies and found that the former improved haemostasis and reduced deaths from exsanguination within the first 24 hours. Although overall mortality at 30 days did not differ significantly, the trial established 1:1:1 as the gold standard for early resuscitation.[9]
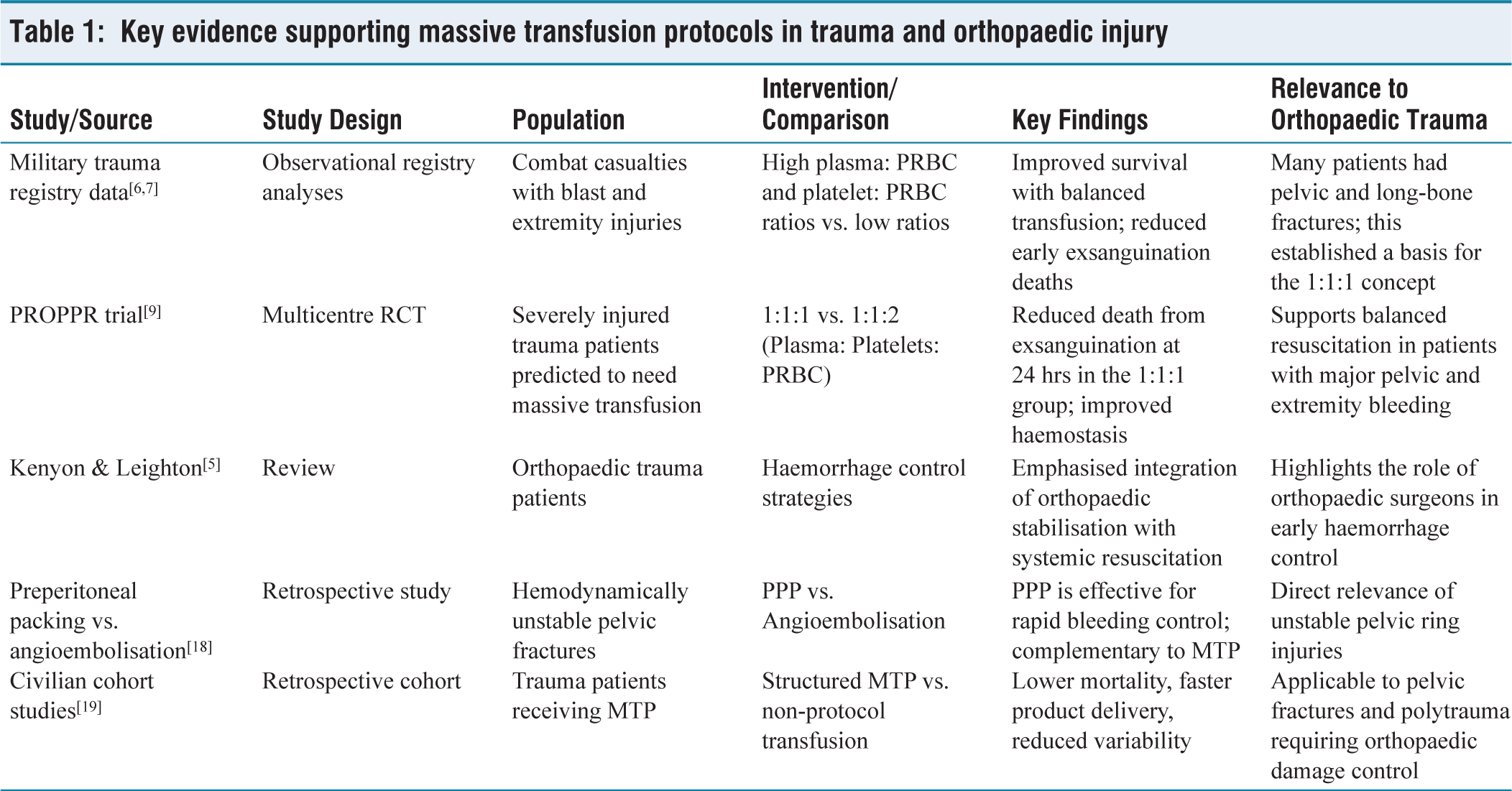
Orthopaedic-specific studies are fewer but increasingly supportive. Patients with pelvic fractures requiring massive transfusion have shown improved outcomes with early activation of MTPs, including lower mortality and reduced incidence of coagulopathy. Similarly, studies of long-bone fractures complicated by vascular injury suggest that early balanced transfusion improves limb salvage rates and reduces amputation risk. Meta-analyses pooling data across trauma populations confirm that structured MTPs reduce variability in practice, shorten time to product delivery, and improve survival in severely injured patients.[14] This is summarised in Table 1.
Key evidence supporting massive transfusion protocols in trauma and orthopaedic injury
Discussion
The transformation of trauma resuscitation through MTPs is a testament to the iterative process of military-civilian collaboration. Orthopaedic trauma, with its high risk of exsanguination, has been both a driver and a beneficiary of these advances. Battlefield experience demonstrated that aggressive crystalloid use was detrimental and that balanced blood product resuscitation saved lives. These lessons were quickly adapted to civilian trauma, where structured MTPs standardised care and improved survival.[14]
Orthopaedic surgeons are now integral to the broader resuscitative team, not merely as technicians of bone fixation but as key players in haemorrhage control. From applying pelvic binders and external fixators to coordinating with interventional radiologists and trauma surgeons, orthopaedic specialists contribute directly to achieving haemostasis. DCO aligns perfectly with MTP-driven DCR, creating a unified approach to managing physiologically unstable patients.[8]
Nevertheless, challenges remain. Overtransfusion risks must be balanced against the dangers of under-resuscitation. Logistics and supply chain issues continue to limit widespread adoption in low-resource settings. Ethical dilemmas in resource allocation persist in both battlefield and civilian disasters. Moving forward, advances in portable blood products, viscoelastic-guided resuscitation, and AI-driven decision support may further optimise outcomes. The ultimate goal remains consistent: to save lives and limbs by integrating orthopaedic expertise with systemic resuscitation science.[10]
Challenges and Limitations
Despite their success, MTPs are not without challenges. Overtransfusion remains a significant concern, with risks including transfusion-related acute lung injury, transfusion-associated circulatory overload, and immunomodulatory complications.[20] Resource allocation is another challenge, as maintaining adequate supplies of plasma and platelets is logistically demanding, particularly in austere environments or smaller civilian hospitals. Battlefield innovations such as fresh whole blood and walking blood banks are not easily replicable in civilian settings due to regulatory and donor safety constraints.
Ethical dilemmas also arise, particularly in mass-casualty or battlefield scenarios where resource rationing becomes necessary. Deciding which patients receive scarce blood products can be agonising, particularly when survival probabilities are uncertain. Training gaps among orthopaedic surgeons and trauma teams also exist, as not all providers are equally familiar with transfusion science. Ensuring interdisciplinary education and simulation training is critical to optimise protocol adherence.[21]
Future Directions
The future of MTPs lies in enhancing precision, portability, and sustainability. Cold-stored platelets and freeze-dried plasma are under development to extend shelf life and allow use in resource-limited or battlefield environments.[22] Artificial oxygen carriers and haemoglobin-based substitutes may one day replace or supplement red cells, reducing dependence on donor supply.[23] Portable viscoelastic devices may allow point-of-care assessment even in prehospital settings, enabling truly tailored resuscitation.[24] Artificial intelligence tools capable of predicting transfusion needs based on real-time vital signs and injury patterns may further refine MTP activation and delivery.[25] Civilian-military integration, through joint trauma registries and shared training programmes, will continue to drive progress.[26] For orthopaedic trauma specifically, these innovations hold promise for earlier intervention, improved survival, and better functional outcomes.
Conclusion
MTPs, born from the crucible of battlefield medicine, have transformed trauma care and profoundly influenced orthopaedic practice. By shifting resuscitation from crystalloid-heavy strategies to balanced, protocolised blood product delivery, MTPs have reduced mortality in patients with exsanguinating orthopaedic injuries. Orthopaedic surgeons, once peripheral to resuscitation, now play a central role in haemorrhage control within the framework of DCR. The continued evolution of MTPs promises even greater gains, with innovations such as freeze-dried plasma, cold-stored platelets, and AI-guided resuscitation shaping the future. As civilian and military systems continue to share knowledge and experience, the lessons of the battlefield will remain vital in saving lives on both warfronts and home fronts.
Footnotes
Data availability
Data is available within the manuscript itself. Additional data if required may be obtained from the corresponding author upon request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable.
Informed consent
Not applicable.
Credit author statement
VS: Conceptualisation and methodology; Data curation and investigation; Formal analysis and drafting.
MR: Conceptualisation and methodology; Review, editing, visualisation, and supervision; Project administration and correspondence.
Use of artificial intelligence
No.
Trial registration number
Not applicable.