
Abstract
Introduction:
The risk of dengue has expanded in terms of population size as well as its geographical distribution. Despite advances in pediatric critical care, dengue continues to be a challenging illness, affecting all ages and with a spectrum ranging from asymptomatic to fatal disease.
Objectives:
This article provides an in-depth narrative review of the latest dengue epidemiology, the current understanding of pathogenesis, clinical and laboratory diagnosis, management and prevention. The analysis has been drawn from a comprehensive review of recent research articles related to these topics.
Conclusion:
The management strategies for the critically ill have improved in recent years with attention to early risk stratification and judicious use of intravenous fluids and blood products. However, despite the increasing burden of dengue illness with every year, knowledge gaps remain in applicability of new biomarkers and development of therapeutics and universally acceptable vaccines.
Keywords
Introduction
Dengue is a mosquito-borne illness which can affect people of all ages. Half the world’s population lives with the risk of being infected with dengue.[1] Cases are expected to rise further with urbanisation, travel and climate change. The disease is caused by the dengue virus (DENV), which belongs to the same family as other vector borne viruses causing disease in humans, such as yellow fever, West Nile, Japanese encephalitis and tick-borne encephalitis viruses.
A narrative review of dengue in children is presented after extracting relevant research articles published over recent years.
Dengue Virus
DENV is a positive-stranded RNA virus inside a nucleocapsid and a roughly spherical envelope. It is classified into four strains called DENV-1, DENV-2, DENV-3 and DENV-4 numbered based on the chronological order of their discoveries. These are termed serotypes because they can differ in their interactions with the antibodies present in the host sera.
The four serotypes have a similarity of about 65% genome. A fifth variant, DENV-5, was isolated in Malaysia in October 2007, which follows the sylvatic cycle, unlike the other four serotypes, which have sustained transmission through the human cycle.[2]
Epidemiology
Global
Dengue cases have increased exponentially across the world in the last 25 years, from 0.5 million to 14 million in 2024, with endemicity in more than 100 countries.[1] There were a record 14 million cases and 9,000 deaths of dengue reported through the World Health Organisation (WHO) global surveillance system in the year 2024.[3] Since dengue infection is mostly asymptomatic or mildly symptomatic, the reported numbers might just be the tip of the iceberg. The maximum number of cases is reported from the Region of the Americas. Dengue has also expanded in geographical distribution, with the European and Eastern Mediterranean regions reporting dengue cases.
National
As per the data of the National Centre for Vector Borne Diseases Control, all states and union territories except Ladakh are endemic for dengue. In 2025, there were about 0.1 million cases reported with 95 deaths.[4] However, these numbers could be underreported. Dengue is known to have cyclic outbreaks every 2–4 years associated with serotype or genotype replacement.[5] Since 2000, all four serotypes have circulated in India. The serotypes which dominated were DENV-1 and DENV-3 till 2012, followed by DENV-2 in the last decade in many parts of the country and DENV-4 in Southern India.[6]
Dengue generally peaks in India during the monsoon months (June-September) due to the rise in mosquito population, as the vector is active throughout the year, causing illnesses post monsoon (October-January) and pre monsoon (February-May).[7]
Transmission
Transmission occurs through the domestic Aedes aegypti and peridomestic Aedes albopictus mosquitoes. Environmental factors such as temperature, humidity and vegetation cover affect dengue transmission dynamics.[8] Climate change appears to contribute to rising temperatures, an increasing rate of development of mosquitoes and precipitations encouraging breeding habitats.[9]
In India, the main vector is Aedes aegypti, especially in the urban areas, which breeds almost entirely in and around households, such as overhead tanks, construction sites, flower pots and open water drums. Aedes albopictus usually breeds in natural habitats such as the latex collecting cups in rubber plantations, coconut shells and tree holes. The mosquito becomes infected after an extrinsic incubation period of 8–10 days post bite of a human infected with dengue.
Dengue Pathogenesis
When an individual gets infected for the first time, it is called a primary infection, which is usually asymptomatic or mildly symptomatic. Immunity to other types, that is, heterologous immunity, is short -lived, re-infection with another serotype can occur. Subsequent infection with a different serotype leads to more severe disease or secondary dengue.
Dengue NS1 antigen directly disrupts the integrity of the vascular endothelial cells. It also acts on the complement system of the host. This results in inflammatory cytokine production, which causes an increase in vascular permeability and plasma leakage.
In secondary dengue, there is a swift decline of NS1 antigen levels with a rapid surge of dengue immunoglobulin G (IgG) antibodies, pre-existing from previous infection, which form immune-mediated complexes responsible for severe manifestations of secondary dengue. Antibody-dependent enhancement (ADE) occurs when the antibodies produced by primary infection are unable to neutralise the DENV belonging to a different serotype. These virion antibody immune complexes enter Fc receptor-bearing cells, resulting in an increase in the number of infected cells and the amount of virus produced per cell.[10] However, a recent study from India of hospitalised children with dengue showed that primary dengue infections accounted for more than half of total clinical cases (344 of 619), severe dengue cases (112 of 202) and deaths (5 of 7).[11] The results challenged the assumption that primary dengue is generally not associated with severe dengue.[11]
Host factors such as younger age, obesity, immunocompromised condition, pre-existing illnesses such as diabetes, renal cardiovascular disease are predictors for progression to severe dengue in children.[12–14]
In a few children, DENV can significantly impair the perfusion and endothelial impermeability of the microcirculation, leading to severe plasma leakage and hypovolemic shock. Though the virus shares a similar pathogenesis of microvascular dysfunction as in septic shock, the volume of plasma leakage appears to be much more significant in dengue.[15] There are various categories of host biomarkers showing promising prediction of progress to severe dengue, such as transcriptomic (20-gene set), anti- DENV antibody titer, circulating long non-coding RNAs (lncRNAs) and other inflammatory markers including chymase, interleukin 10 (IL-10), interferon-gamma (INF-Y).[16,17]
Among serotypes, DENV2 is mostly associated with severe dengue.
DENV causes thrombocytopenia by affecting the production of mature megakaryocytes and thrombopoiesis as well as by increasing platelet activation, apoptosis and clearance.[18]
Clinical Features
Symptomatic dengue can have a febrile phase, critical phase and recovery phase. Fortunately, the majority of the children do not experience the critical phase and the fever subsides with improvement in general condition.
Febrile Phase
After an intrinsic brief incubation period of 4–7 days, dengue illness starts abruptly with fever. During this febrile phase, viremia occurs, which manifests as headache, nausea, myalgia, body ache and rash. There is reduced urine output. Older children may complain about retro-orbital pain. There could be a recurrence of fever, which is also called ‘biphasic fever’ or ‘saddleback fever’.
The potential clinical issues that need attention are possible dehydration during the febrile phase and reduced urine output. A few children can have febrile seizures or delirium owing to fever and not associated with the underlying illness.
Critical Phase
In some children, the critical phase can begin around the time of defervescence of fever when the body temperature drops to lower than 38 °C and remains below this level. During this phase, plasma leaks out and can cause potential complications due to depletion of the intravascular compartment and resulting organ damage. Generally, this phase of plasma leak does not occur for more than 48 hours.
The critical phase is the most dangerous phase, where there could be shock, bleeding (usually in the gastrointestinal tract and rarely in the brain) or organ impairment defined as liver enzymes over 1000 IU/L, raised cardiac enzymes with ventricular dysfunction and impaired consciousness. As compared to adults, child presents with shock rather than bleeding manifestations. It is important to note that the fall in conscious level and systolic blood pressure could occur in advance stages of shock. Hence, the critical early signs to watch out for are prolonged capillary refill time, tachycardia, narrowing pulse pressure, cool peripheries and reduced urine output.
Recovery Phase
The recovery phase starts when the plasma leakage resolves. A confluent, erythematous macular rash appears as a harbinger of the recovery phase with patches of normal skin, called ‘white islands in a sea of red’, which generally resolves in about three days and can be associated with itching.
During the recovery phase, there is gradual reabsorption of extravascular fluid in the next 48–72 hours. There could be development of rash, which is classically called as isles of white in the sea of red. Clinical issues are fluid overload in case too much of fluids were given in the leaking phase.
Laboratory Course of Dengue
The complete blood count can be normal in a febrile illness. Leukopenia, haematocrit rise and thrombocytopenia are more pronounced in the critical phase. Leucopenia is associated with a decrease in eosinophils, neutrophils and platelets and a significant increase in monocytes and lymphocytes.[19] The recovery phase is heralded by the rise in white blood cell counts, followed by a rise in platelets. Thrombocytopenia persists longer. The haematocrit generally becomes normal, but can reduce due to dilution caused by reabsorbed fluid.
During the febrile illness, especially within five days of illness, dengue may be diagnosed by virus isolation in cell culture, by detection of viral RNA by nucleic acid amplification tests (NAAT) or by detection of viral antigens NS1 by enzyme-linked immunosorbent assay (ELISA) or rapid tests. Dengue serological testing for antibodies, IgM ELISA, is useful for diagnosis after five days of illness. The IgG ELISA test is used to differentiate between primary and secondary dengue, as its presence indicates past infection. Here, rapid tests need to be utilised with caution due to a lack of standardisation.
A recent systematic review and meta-analysis comparing the performance of dengue NAAT and NS1 by ELISA done in the first four days and dengue IgM ELISA (days 1–7) estimated pooled estimates of sensitivity 95%, 90% and 71%, respectively and specificity of 89%, 93% and 91%, respectively.[20]
Rise in serum transaminases is the commonest biochemical abnormality noticed in children in the first week of illness, with more derangement of alanine transaminase than aspartate transaminase.[21]
A bedside ultrasound of the abdomen and lungs is useful in detecting early plasma leakage. It is reported that one-third of hospitalised dengue patients present with pleural effusion and the frequency increases with severity and younger age.[22]
Management
Risk Stratification Based on Clinical Criteria
The transition from febrile illness to critical phase can take place any day of the illness, as early as one day or beyond a week. The hallmark of this transition is the defervescence of fever. Therefore, in all suspected cases of dengue, it is important to identify any child who is at risk of critical phase symptoms and signs. For this purpose, the revised WHO 2009 guidelines classified dengue as dengue without warning signs, dengue with warning signs and severe dengue (severe plasma leakage, severe bleeding or organ failure).[23] WHO listed clinical warning signs as persistent vomiting, severe abdominal pain, mucosal bleed, lethargy, restlessness, hepatomegaly of over 2 cm and any signs of clinical fluid accumulation. The corresponding laboratory clues could be leucopenia, a sudden drop in platelet count and rising haematocrit. Recent studies report that the addition of clinical features such as peri-orbital oedema and splenomegaly and laboratory findings such as elevated urea and creatinine, hypoalbuminemia might help improve the sensitivity and specificity of the revised WHO dengue classification.[24]
Management Based on Risk Stratifications
Dengue without warning signs can be managed in ambulatory settings with symptomatic treatment, counselling regarding oral fluid intakes such as oral rehydration solutions and to seek attention in case of warning signs. These children should be regularly followed up by primary care physicians to pick up warning signs. Dengue with warning signs should be preferably admitted. Management of severe dengue would need critical care expertise and should be done preferably in an intensive care unit.
Management of Fluids in Dengue
For children requiring hospitalisation, management is centred around judicious use of intravenous crystalloids. The choice of fluids should be isotonic-normal saline (NS) (0.9%) or ringer lactate (if hypernatraemia or hyperchloremia).[25] Hypotonic solutions should be strictly avoided even during the febrile phase.
In comparison to a septic child, the fluid loss in dengue is roughly equivalent to plasma loss. During the leaking phase, the rate of the fluid is adjusted to target a pulse pressure of 30 mm Hg and urine output of at least 0.5–1 mL/kg/h. In compensated shock, isotonic crystalloid fluids are started at 10–20 mL/kg/h over one hour. If the vitals, capillary refill time and haematocrit improve, fluids should be gradually reduced to 7–10 mL/kg/h for 1–2 hours, then to 5–7 mL/kg/h for 1–2 hours, then to 3–5 mL/kg/h for 2–4 hours, then 2–3 mL/kg/h for 2–3 hours and then further depending on haemodynamic status, which can be maintained for up to 24–48 hours. If shock persists and haematocrit increases or is still more than 45%, repeat a second bolus of crystalloid solution at 10 mL/kg/h for one hour. If there is improvement, then reduce the rate to 7–10 mL/kg/h for 1–2 hours and then continue to reduce as above.[24] In case of compensated shock, initiate crystalloid or colloid solution (if available) at 20 mL/kg as a bolus given over 15 minutes. If there is improvement, follow the fluid titration as in compensated shock. Generally, plasma leakage stops after 48 hours; not usually more than the total volume of maintenance plus 5% deficit is required over 48 hours.[26]
In failure of fluid resuscitation with a 30 mL/kg bolus of crystalloids, colloids should be administered. Albumin could be the choice of resuscitation fluid administered as 1 g/kg over 6–8 hours with hemodynamic monitoring.[27] If albumin is not available, other colloids such as 4% gelatin, hetastarch or dextran can be used. Adverse effects such as anaphylaxis (maximum with gelatin), coagulopathy (maximum with dextran) and acute kidney injury are known with the use of colloids.[27]
Inotropes should be considered in refractory shock. In such situations, the patient should be evaluated for cardiogenic or septic or metabolic reasons or for hidden bleeding. Child in severe dengue may have a high chance of mortality if they are in fluid overload as high as 44%–72%.[27] Knowing when to stop is critical so that there is no volume overload. Fluids must be immediately stopped if there are signs of pulmonary oedema, hypertension with good volume pulse and 48 hours after.
Management of Fluid Overload During Recovery
Fluid overload in severe dengue is a challenging situation, many times due to dynamic variation in glomerular filtration rate in the leaky phase of dengue shock syndrome with or without acute kidney injury. A cumulative fluid overload of greater than 10% is highly associated with the requirement of mechanical ventilation and associated mortality.[28]
While working in a tertiary referral centre, we have observed many referrals from small hospitals of severe dengue with fluid overload. These children can be classified into categories for management purposes.
Diuretic-responsive fluid overload: Furosemide infusion can be started at the infusion rate of 0.05–0.1 mg/kg/h and titrated to maintain a urine output of 2–4 mL/kg/h.[29] Potassium levels should be monitored during furosemide infusion and corrected if hypokalaemia occurs. In normotensive children, if the blood pressure is borderline, 20% albumin with Lasix infusion can be started under strict hemodynamic monitoring in paediatric intensive care settings.
Intra-abdominal pressure (IAP) monitoring through a urinary catheter is critical to detect intra-abdominal hypertension and abdominal compartment syndrome (ACS). If IAP remains sustained at greater than 10 mmHg/cm H2O every two hours with concomitant progression of ACS in terms of worsening of circulation, acidosis, hypoxemia and decreased urine output, then drainage of fluid would be required.[27] However, this drainage must be slow-controlled drainage rather than a rapid decompression.
Diuretic-resistant fluid overload with acute kidney injury: Measures such as peritoneal dialysis, continuous renal replacement therapy or sustained low-efficiency dialysis may be beneficial.
Management of Bleeding and Use of Blood Products
Suspect bleeding if there is a drop in haematocrit along with unstable vital signs. Packed red blood cells (RBC) or whole blood transfusion should be immediately given in such situations. Platelet transfusion is not indicated unless there is bleeding. It may be considered prophylactically without bleeding if platelets are <10,000/cu mm and those who may need emergency surgery.
An immature platelet fraction of >10% predicts the platelet recovery. Elevated levels of platelet micro-particles derived from activated platelets may act as a biomarker guide to decide prophylactic platelet transfusion in severe dengue with platelets <10,000/cu mm with or without bleeding manifestation.[25]
Expanded Dengue Syndrome
Expanded dengue syndrome refers to severe dengue with multiorgan involvement [Figure 1] and requires intensive care monitoring and multidisciplinary team management.
Potential complications in an expanded dengue syndrome[23]
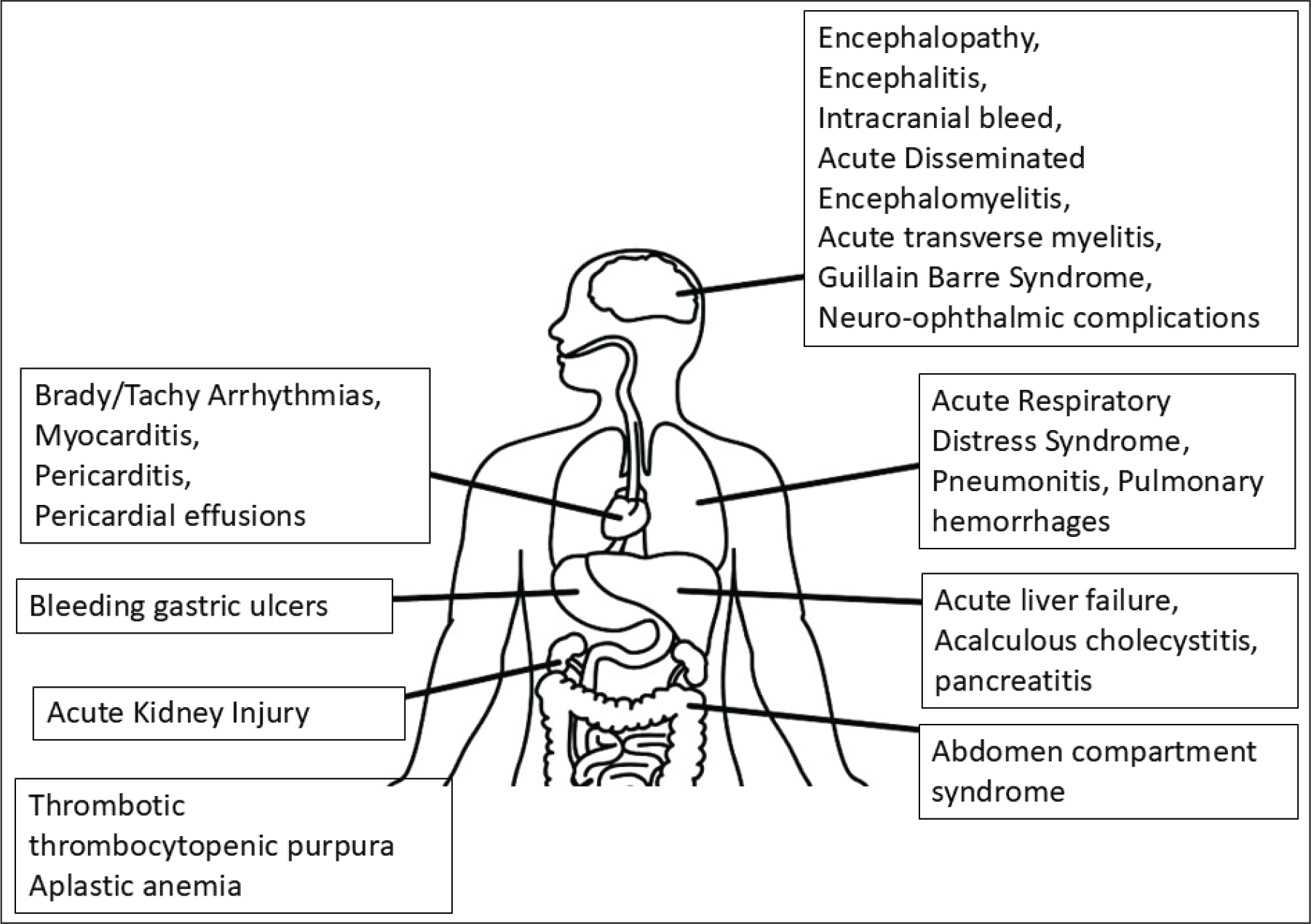
Those with cardiac complications require close monitoring of heart rate, blood pressure, 2D echo, NT pro-BNP and need to watch for congestive cardiac failure and pulmonary oedema. Early initiation of inotropic support is recommended. Management of acute liver failure is similar to that of liver failure due to other causes. Early initiation of continuous renal replacement therapy may be required in acute kidney injury. Pleural tap should be avoided in dengue unless it results in hemodynamic compromise. Anti-epileptics may be needed in cases of seizures and 3% sodium chloride in raised intracranial tension. Intravenous (IV) immunoglobulins and pulse steroids may be useful in cases of immune-mediated complications such as Guillain-Barré syndrome or acute demyelinating encephalomyelitis.
Dengue-associated Hemophagocytic Lymphohistiocytosis
In a recent systematic review and meta-analysis, the prevalence of hemophagocytic lymphohistiocytosis (HLH) in severe dengue was higher in the paediatric population (22.8%) compared with the adult population (19.0%), with a significant increase in mortality.[30] Hence, early recognition and prompt treatment are crucial as well as challenging. Figure 2 gives the overlapping features and clinical and laboratory clues to help differentiate dengue-associated HLH from severe dengue without HLH.[31]
Diagnosis and management of dengue-associated hemophagocytic histiocytosis[27]
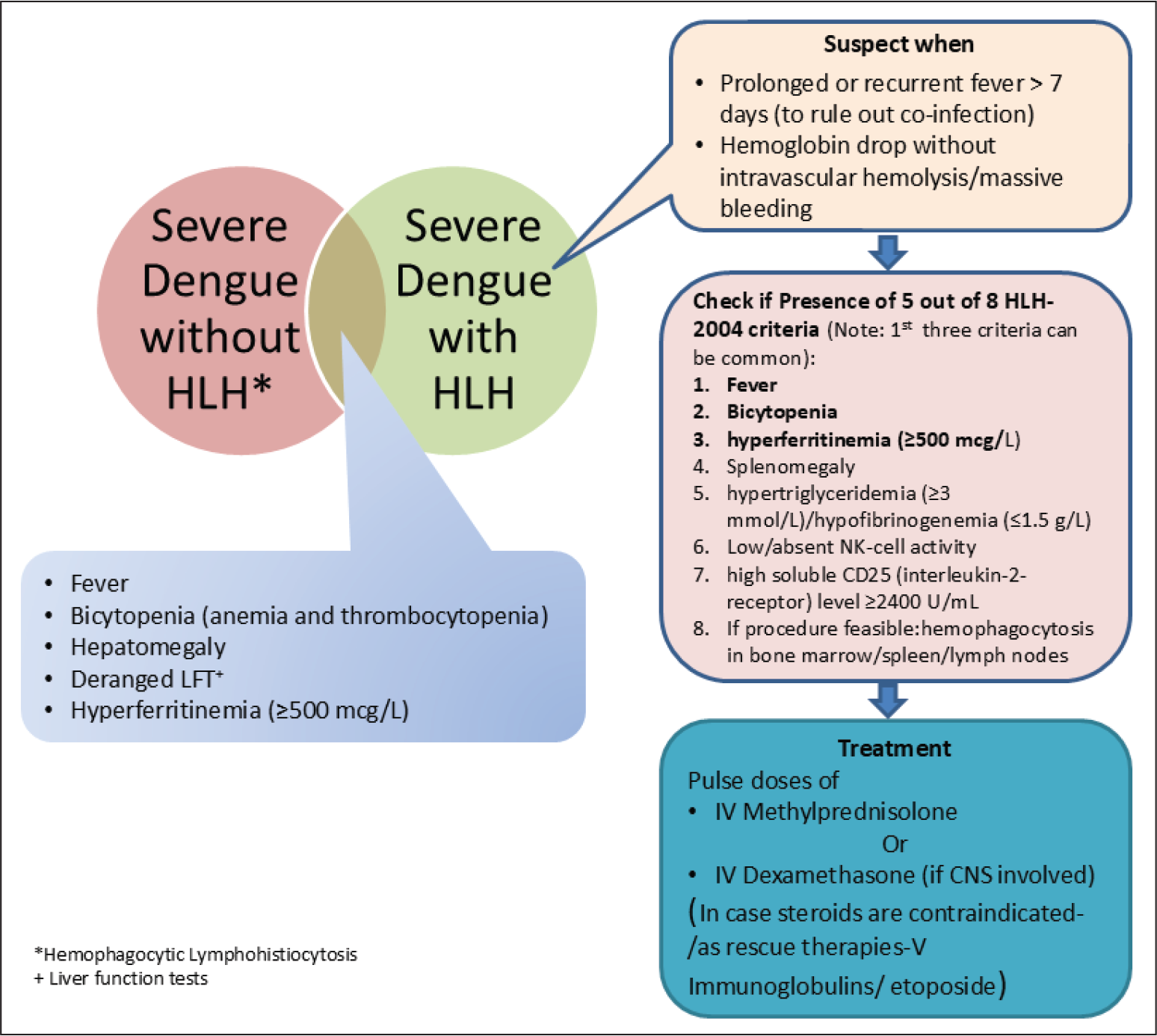
Usually, bone marrow examination is not needed when most of the other parameters of the HLH criteria are fulfilled.[31] High dose of steroids with either methylprednisolone or dexamethasone is the main therapeutic method. Immunoglobulins, along with antibiotics, can be an alternative if sepsis is also suspected. Some other agents, such as cyclosporine or etoposide, are usually not required in dengue-related HLH. Novel agents such as emapalumab, tocilizumab, anakinra and ruxolitinib need to be studied in the context of dengue-associated HLH while preserving immune response against infections.
Prevention of Dengue
Vector Control
Physical methods, such as reducing breeding sites, biological methods such as the use of Wolbachia-infected mosquitoes and community engagement seem to be effective as vector control strategies.[32]
Antivirals
There is currently no effective antiviral available for use. Drug repurposing and novel candidates, such as eltrombopag, doxycycline, UV-4B and plant drugs such as Caripill, are under research and most have not advanced beyond preclinical stages.[33,34]
Dengue Vaccine
Of the at least seven DENV vaccines that have undergone different phases of clinical trials, only three of them (Dengvaxia→, TV003 and TAK-003) have shown promising results (Table 1).[6,35–37]
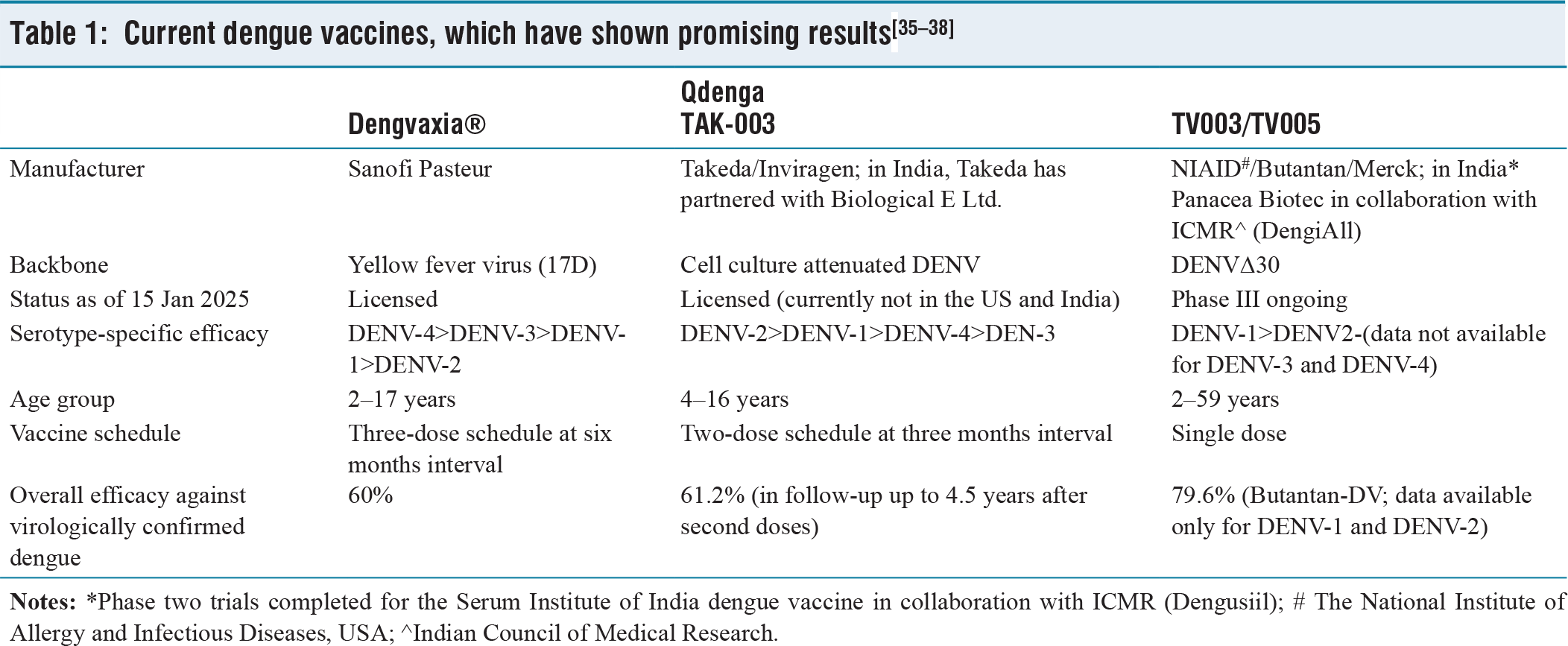
Dengvaxia is licensed for use in children aged 9 through 16 years of age in a few countries; however, there was an increased risk of hospitalisations in seronegative individuals when they were exposed to natural infection. TAK-003 has been shown to be well-tolerated in the phase III clinical trials in children.[35] TAK-003 has been recommended by WHO in geographical locations where there is high transmission intensity of dengue transmission as a two-dose schedule between 6 and 16 years.[37]
Immune selection pressure is a primary driver in the evolution of serotypes, which has a direct impact on the vaccine efficacy. Indian DENV-1 and DENV-4 are distinct from all available vaccines compared to DENV-2 and DENV-3, highlighting the need for an India-specific vaccine strain for good efficacy against all serotypes. Indian researchers are targeting the envelope protein domain III for developing a tetravalent vaccine, which has the potential for broader protection as well as safety from ADE.[6]
Conclusion
There have been substantial advancements in knowledge of dengue, with a deeper understanding of the pathogenesis and discovery of new biomarkers for diagnosis and targets for prevention. However, knowledge gaps remain for the wider applicability of these novel agents, a lack of therapeutics and a uniformly acceptable dengue vaccine for prevention. There is an urgent need to cope with the increasing burden of this disease and the mortality caused.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/ or publication of this article.
Institutional ethical cmmittee approval number
Not applicable.
Informed consent
Not applicable.
Credit author statement
DD conceptualised the draft, DD and NM reviewed literature, edited and approved the final draft.
Data availability
Not applicable.
Use of artificial intelligence
No Artificial Intelligence was used.