
Abstract
Introduction:
When a child needs a tracheostomy, it will change their life. Paediatric tracheostomies are becoming more common. More children are getting tracheostomies at a younger age, living longer, and receiving care at home. A tracheostomy is an artificial airway for those who require long-term assistance with respiratory or secretion clearance, or where airway patency or safety is compromised.
Methods:
A comprehensive review of literature from databases such as Scopus, PubMed, Medline, and Google Scholar was conducted to discuss the quality of life (QOL) of paediatric patients with tracheostomy and their caregivers.
Results:
A paediatric patient and their family must adjust to a new way of life when they have a tracheostomy. To establish safe, unobstructed breathing, tracheostomy has great importance. Caring for children with a tracheostomy impacts the QOL of both the children and their caregivers. Children with a tracheostomy often face various challenges, including social, psychological, medical, and financial hardships, which are well recognised.
Conclusion:
The QOL of paediatric patients with tracheostomies is associated with moderate levels of distress in their caregivers and has a detrimental effect on the caregivers’ mental health. There is a paucity of medical literature on QOL and burden experienced by paediatric patients with tracheostomy and their caregivers. Therefore, this review article aims to discuss the QOL of paediatric patients with tracheostomy and their caregivers.
Introduction
Tracheostomy of a child is a life-changing event of patient. Tracheostomy care for paediatric patients can significantly affect the quality of life (QOL) of patients and their caregivers.[1] Tracheostomy is an artificial airway that compromises airway patency or safety for people who require long-term assistance with ventilation or secretion clearance.[2] The establishment of a safe and unobstructed airway has great importance for a paediatric patient.[3] However, a holistic clinical decision is made on the account of the complex ongoing care and psychosocial implications on the child and their caregivers. The decision of tracheostomy on a paediatric patient is a challenging situation for the paediatric patient, impacting not only the child but also their family members.[2] A child with a tracheostomy may experience difficulties with speech, eating, sleeping, school activities, and water-based activities.[2] For both routine care and emergency situations, the child must always be under the supervision of a trained adult. Significant adjustments to everyday life, family dynamics, and lifestyle are required due to the adjustment and obligations.[4] Constant vigilance is provided to paediatric patients with tracheostomy and their caregivers. There is a paucity of studies and reviews of QOL and burden experienced by caregivers of paediatric tracheostomy patients, which tempted author to undertake this review article. Discussing the QOL for paediatric tracheostomy patients and their caregivers is the goal of this review. In order to fully understand the various aspects that can affect the well-being of the child and caregiver, we include both QOL and caregiver burden in our review.
Methods of Literature Search
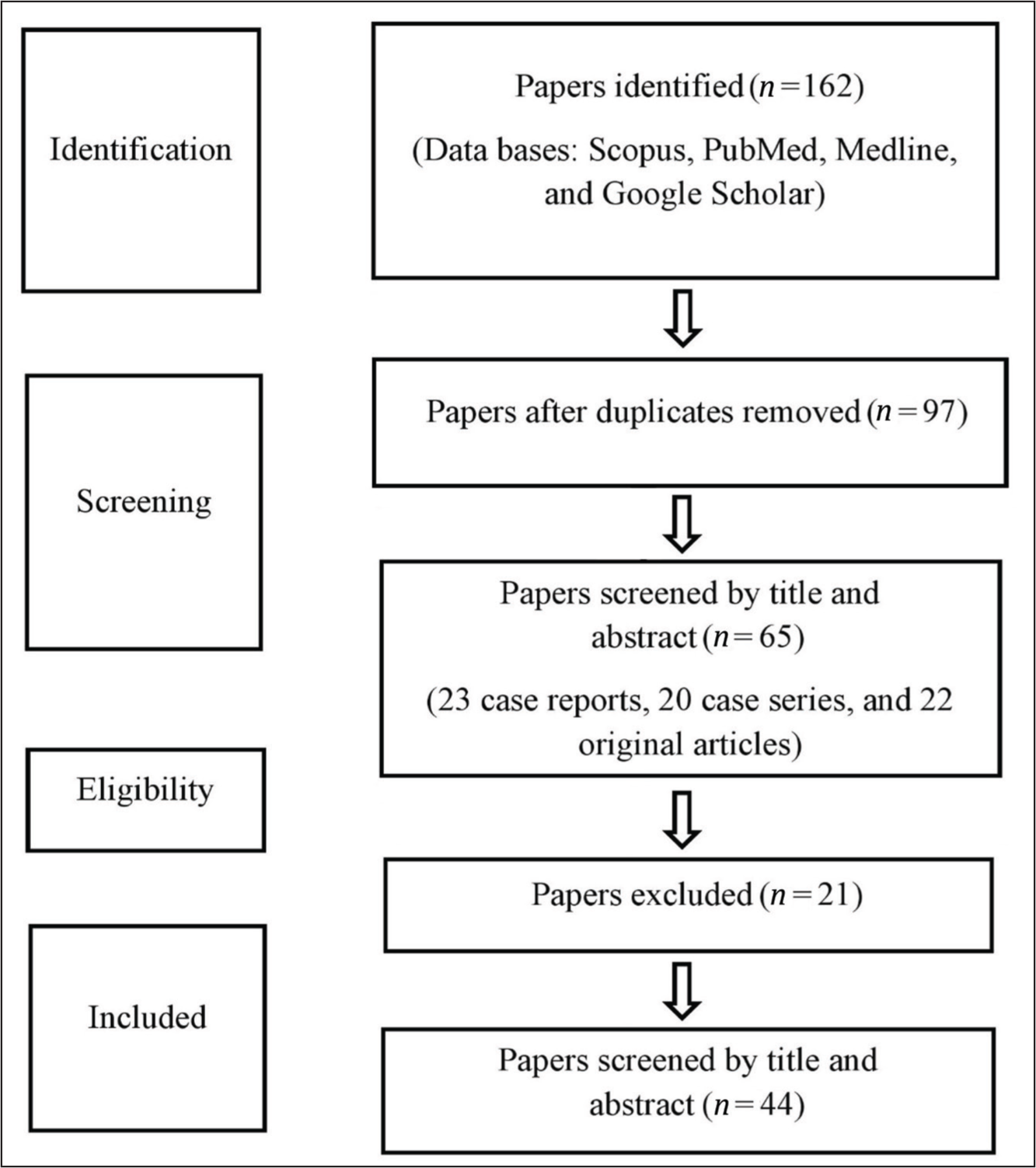
We conducted a search for research articles on the QOL of paediatric patients with tracheostomy and their caregivers using various methods. This began with searching online databases such as Scopus, PubMed, Medline, and Google Scholar. A search strategy was created based on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines. The search approach found published article abstracts, and citations were used to manually find more research publications. The suitability of observational studies, comparative studies, case series, case reports, and randomised controlled trials for inclusion in this review was evaluated. A total of 65 articles (23 case reports, 20 case series, and 22 original articles) were found across various databases, with 44 being included in this review [Figure 1]. This article discusses the QOL of paediatric patients with tracheostomy and their caregivers.
Methods of literature search
Prevalence
The prevalence of paediatric tracheostomy is increasing in several countries, with more children receiving the procedure at a younger age and surviving longer.[5] As a result, many require ongoing care at home. This caregiving responsibility significantly impacts the QOL of both the children and their caregivers. Different centres in developed countries report high rates of serious tracheostomy-related complications, including airway obstruction, accidental decannulation, bleeding, and infections, with morbidity rates ranging from 24% to 58%.[6] One study reported that 24% parents of children with tracheostomy caring for home-ventilated children lived in an informal house, and 66% have incomplete schooling.[7]
Paediatric Tracheostomy
The treatment of acute airway obstruction is no longer the primary reason for paediatric tracheostomy; instead, it is being used to treat children with medically complex diseases.[8] Many children are undergoing tracheostomy at a younger age and living longer, and are cared for at home.[9] After being released from the hospital, these children are cared for by family members or caretakers, usually their parents, with sporadic assistance from medical professionals.[10] Paediatric tracheostomy is a challenge in the practice of otorhinolaryngology. Currently, the common indications of tracheostomy among paediatric patients include airway stenosis, craniofacial anomalies, neuromuscular disorders, and prolonged endotracheal intubation.[11] For children with cardiac, craniofacial, or upper airway issues, the average age of tracheostomy placement is between 4 and 6 months; for children with neurological illnesses or trauma, it is between 2 and 3 years.[12] In addition to living longer and receiving care at home, more paediatric patients are having tracheostomies at younger ages.[9] Following their hospitalisation, these tracheostomy-afflicted children are cared for by family members and caregivers, usually their parents, with varying degrees of assistance from the medical services.[13] It is associated with higher morbidity and mortality in children than in adult age groups. Paediatric tracheostomy needs a multidisciplinary approach and involves otorhinolaryngologists, child specialists, specialist nurses, physiotherapists, and speech language therapists. This is very important as paediatric tracheostomy can affect the QOL of children. Paediatric tracheostomy has a detrimental effect on a child’s physical and mental or psychosocial health.[14] One study highlighted the adverse effects of tracheostomy in paediatric age on children’s speech development.[2]
Paediatric Tracheostomy Care
The daily care of paediatric tracheostomy includes suctioning and replacing the tracheostomy tube. The daily care of paediatric tracheostomy involves cleaning of the stoma, changing tracheostomy ties and tubes, suctioning secretions, and ensuring proper humidification and hydration.[2] The caregiver should know who to contact for tracheostomy issues when arises such as bleeding on inadvertent decannulation.[15] It also needs careful attention to prevent complications like skin breakdown, infection, and accidental decannulation. The development of scar tissue surrounding the stoma may make it difficult to change the tracheostomy tube; in certain cases, surgical revision and scar tissue excision are required. A better outcome can be achieved by coordinating the care of otorhinolaryngologists, pulmonologists, paediatricians, anaesthetists, cardiologists, respiratory therapists, primary care physicians, nurses, neurologists, equipment specialists, and family members or caregivers.[15]
Quality of Life
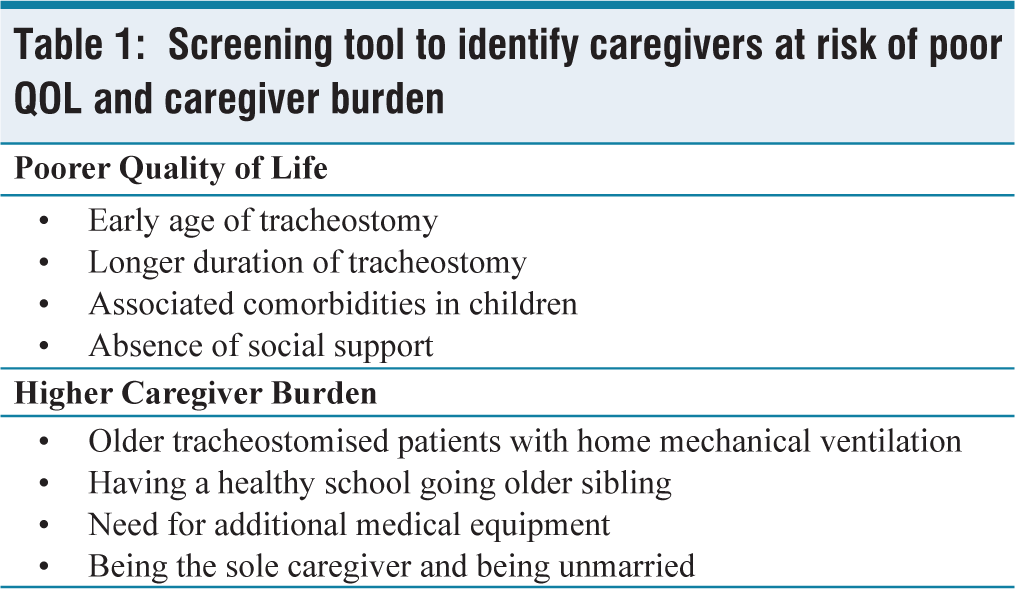
A child with a tracheostomy must adjust to a new way of life and deal with a number of social, psychological, physical, and financial difficulties.[16] Setting up a house for a tracheostomised child’s stay and care can be difficult. Long-lasting medical equipment must be acquired, feeding regimens and home nursing support must be set up, and caregivers must be instructed on how to take care of a tracheostomy at home.[17] QOL, a concept closely related to the burden of caregiving, is defined as an individual’s perception of their place in life, shaped by the cultural and value systems in which they live, as well as their personal goals, expectations, standards, and concerns.[18] QOL serves as an important indicator of functional abilities related to illness.[19] While caregiver burden provides a more specific assessment of how caregiving affects various aspects of a caregiver’s wellbeing, QOL offers a broader, more integrative view of overall wellbeing, albeit with less specificity than caregiver burden measures.[20] Paediatric tracheostomy requires a multidisciplinary approach that includes not only otorhinolaryngologists but also paediatricians, nurses, physiotherapists, and speech therapists. This comprehensive care is essential, as tracheostomy can have a profound impact on the QOL of both the patient and the caregiver. The lack of time and energy to perform daily activities, social isolation, worries, as well as difficulty in communicating and perceived lack of understanding of their child’s health are instrumental in reduced QOL of caregivers.[21] The anxiety about the future of the child affects the majority of caregivers. This psychosocial impact may be lost in the delivery of medical care. The provision of psychosocial support for these families is now also recommended. In order to help tracheostomised children and their caregivers, especially those with comorbidities who typically have worse QOL scores and need more structured support, home care training is necessary. A screening technique for identifying caregivers at risk of poor QOL and caregiver load is shown in Table 1.
Screening tool to identify caregivers at risk of poor QOL and caregiver burden
Impact of Tracheostomised Child
A child’s ability to communicate vocally, eat, sleep, attend school, play, and engage in water-based activities is significantly impacted by tracheostomy.[22] In order to handle both routine care and emergencies, the child must always be under the supervision of a trained adult. The care for children with tracheostomy places a significant responsibility on the parents, which can affect the family’s cognitive, emotional and physical functioning.[23] There is also an impact on their lifestyle, daily routine and family dynamic. The high costs of frequent medical appointments, consumable supplies, and specialised equipment needed to care for a child with a tracheostomy make a heavy financial burden on families.[3] Additionally, the social stigma of tracheostomy often results in social isolation, further reducing the family’s overall QOL.[23]
Caregivers
Among the different duties that caregivers of paediatric patients with tracheostomies provide at home are cleaning the stoma, dressing, tracheostomy suctioning, and giving medications.[24] In hospital settings, these duties are typically carried out by qualified personnel. Children with tracheostomies have a number of duties for their caregivers. They keep a close eye on the youngster, keeping an eye out for any emergencies such as device failure, secretion-induced tube obstruction, or unintentional dislodgment.[25] The duration of tracheostomy care by caregivers varies depending on the child’s underlying medical conditions. A tracheostomy may be necessary for the rest of one’s life for some illnesses, such as neuromuscular impairments. On the other hand, tracheostomy can be successfully reversed in certain paediatric illnesses, such as chronic lung disease of prematurity, which tend to improve over time.[26] The influence that caring for a patient has on a person’s psychological, physical, emotional, and financial health, as well as their perception of how well they are handling their responsibilities in reaction to requests from the person they are caring for, is known as the caregiver’s burden.[27] The welfare of caregivers is negatively impacted by caregiver strain in a number of ways. According to one study, single parenthood, perceived capacity to manage caring, perceived family functioning, socioeconomic situation, community support, and the needs of the child were risk factors for caregiver stress among caregivers of children with cerebral palsy.[28] The strain of caring for a child with a tracheostomy impacts caregivers’ physical health (more home care duties), psychological health (continuous anxiety for emergencies), emotional health (the child’s incapacity to speak like other kids), and financial health (higher expenses for frequent medical visits, supplies, and the need for equipment).[23] Families with paediatric tracheostomy patients experience a decline in household income due to the greater unemployment rate among caretakers, which restricts their social activities and further degrades their general QOL.
Risk Factors for Poor QOL
Risk factors for reduced QOL and increased caregiver burden include children with related comorbidities, younger age at tracheostomy, poor functional status, need for additional therapeutic interventions, having a healthy older sibling who attends school, increased financial strain, being the only caregiver and not married, and maternal depression.[17,29] The indications for tracheostomy and duration do not have a consistent association with caregivers’ QOL and caregiver burden.[30] Moderate to severe burden of caregiver are related to maternal depression, but not associated with educational level, duration of tracheostomy and age of child.[31] A study showed that a close association exists between caregivers’ well-being and health, and psychosocial outcomes, which included an increased chance of child abuse and neglect.[32] Tracheostomy has a negative impact on the family’s financial situation, the caregivers’ career prospects, and the family’s capacity to give patients the services they require, which may result in the tracheostomised child receiving less than ideal care.[33] Higher QOL scores, on the other hand, are linked to greater coping, reduced stress, and enhanced psychosocial health in caregivers.[34]
Improvement of QOL
Children’s and their caregivers’ QOL may be enhanced by the introduction of an in-hospital tracheostomy care programme and the presence of a dedicated tracheostomy coordinator and nurse in a medical setting.[35] Since early intervention can greatly assist families in coping with a child who has a tracheostomy, it is imperative to identify the elements that affect the QOL for both children and caregivers. Children with several comorbidities would benefit substantially from a specialised tracheostomy care programme and require more focused attention from doctors. The effect of the programme on QOL was demonstrated in a study, which also discovered that families participating in tracheostomy care programmes experienced a notable decrease in medical issues, improving outcomes for both the children and their caregivers.[15] Training of caregivers needs to be intense in-hospital training for effective care in the home. This training of caregivers includes understanding of breathing, obstruction and how to alleviate obstruction by inserting a tracheostomy.[36] Caregivers receive further training in the form of an easy-to-use, educational pamphlet with pictures that they can keep at home. Registered nurses should conduct the training and practice tracheostomy care on mannequins and dolls. The group counselling for caregivers is also provided. The intensive one-to-one training is done to ensure the airway in emergencies.
Socioeconomic Implications
Tracheostomy care compounds challenging socioeconomic circumstances.[35] Children who have significant medical comorbidities are a group that requires additional assistance and care. When providing hospital and home care for a child with a tracheostomy, the socioeconomic consequences should be taken into account.[35] Families face psychological and emotional trauma, more home care duties, and more healthcare expenses. According to a study, the increasing duties of raising these kids led to broken marriages.[37] Numerous parents have reportedly abandoned their children, most likely due to their inability to handle the demands of caring for a child with a tracheostomy.[38] The remaining parent who has been abandoned frequently experiences more stress and social isolation.[38] Many families with children who have tracheostomies are already struggling financially, and additional tracheostomy care duties may keep caregivers from looking for work, further stagnating the economy.
Conclusion
The QOL of children with tracheostomies and their caregivers is greatly influenced by tracheostomy. Family dynamics are also greatly affected by paediatric tracheostomy. Therefore, determining the elements linked to QOL is necessary since prompt treatments and an early decannulation plan may reduce family stress and improve general well-being. Numerous physical and psychological variables might worsen the low QOL and significant caregiver burden experienced by caregivers of children with tracheostomies.
Footnotes
Acknowledgements
The acknowledgements for this review are extended to those who have previously contributed to and conducted research on the same topic. This recognition acknowledges the existing body of work and the collective efforts of researchers in the field. The author expresses gratitude to those who contributed to the development and execution of this research, acknowledging their invaluable support and collaboration. AI plagiarism detection tools were employed to ensure the authenticity of the acknowledgements and avoid any instances of plagiarism.
Consent for publication
The article adheres to ethical principles rooted in the Declaration of Helsinki.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/ or publication of this article.
Institutional ethical committee approval number
Given that this is a literature-based study, it is important to note that strict adherence to ethical principles and guidelines was not required. The research primarily involved the examination of existing literature and did not directly involve human subjects.
Informed consent
Not applicable.
Credit author statement
SKS: Concept,data collection,technical review,editing, and drafting.
Data availability
Santosh Kumar Swain, the author, maintains a commitment to transparency in presenting data in this literature-based study. All information and findings shared in this work are authentic and accurately represent the research conducted. Any potential conflicts of interest have been meticulously disclosed to ensure transparency.
Use of artificial intelligence
No AI tools were used in the preparation of this manuscript.