
Abstract
Background:
Lipohaemarthrosis is the presence of intra-articular fat, synovial fluid, serum and blood products, almost always related to an intra-articular fracture, most commonly observed in the knee. Due to the layering of these components owing to density differences, lipohaemarthrosis has characteristic imaging appearances. Conventionally, it has been assumed that the components of a lipohaemarthrosis are influenced by gravity alone, resulting in layering of the contents parallel to the horizontal plane. Our anecdotal experience, however, suggests that the layers are not always gravity dependent, for reasons that are currently unknown.
Aims and Objectives:
It is the purpose of our study to investigate lipohaemarthroses of the knee and explore potential reasons that explain the associated imaging features.
Materials and Methods:
Computed tomography (CT) scans in 30 knees with a lipohaemarthrosis secondary to an intra-articular fracture were retrospectively analysed. Angles between the horizontal plane and the two interfaces between the three-layered components, as well as the angle of rotation of the knee relative to the horizontal plane in the axial CT images, were measured. A statistical analysis of the data was performed.
Results:
The three layers of lipohaemarthrosis were not perfectly aligned with the horizontal plane in any of the cases, with mean angles of 7 and 4 degrees relative to the horizontal for the two interfaces and the knees were also rotated by a mean of 16 degrees, which was statistically significant (P < .0001).
Conclusion:
The contents of a traumatic lipohaemarthrosis within the knee joint are not always gravity dependent as previously thought.
Introduction
Lipohaemarthrosis is a condition characterised by the presence of fat and blood products within a joint capsule and is almost invariably associated with an intra-articular fracture. It is most commonly observed in the knee joint, especially with fractures involving the tibial plateau, but lipohaemarthroses have also been described in cases of intra-articular fracture of other large joints such as the glenohumeral joint, hip and elbow.[1]
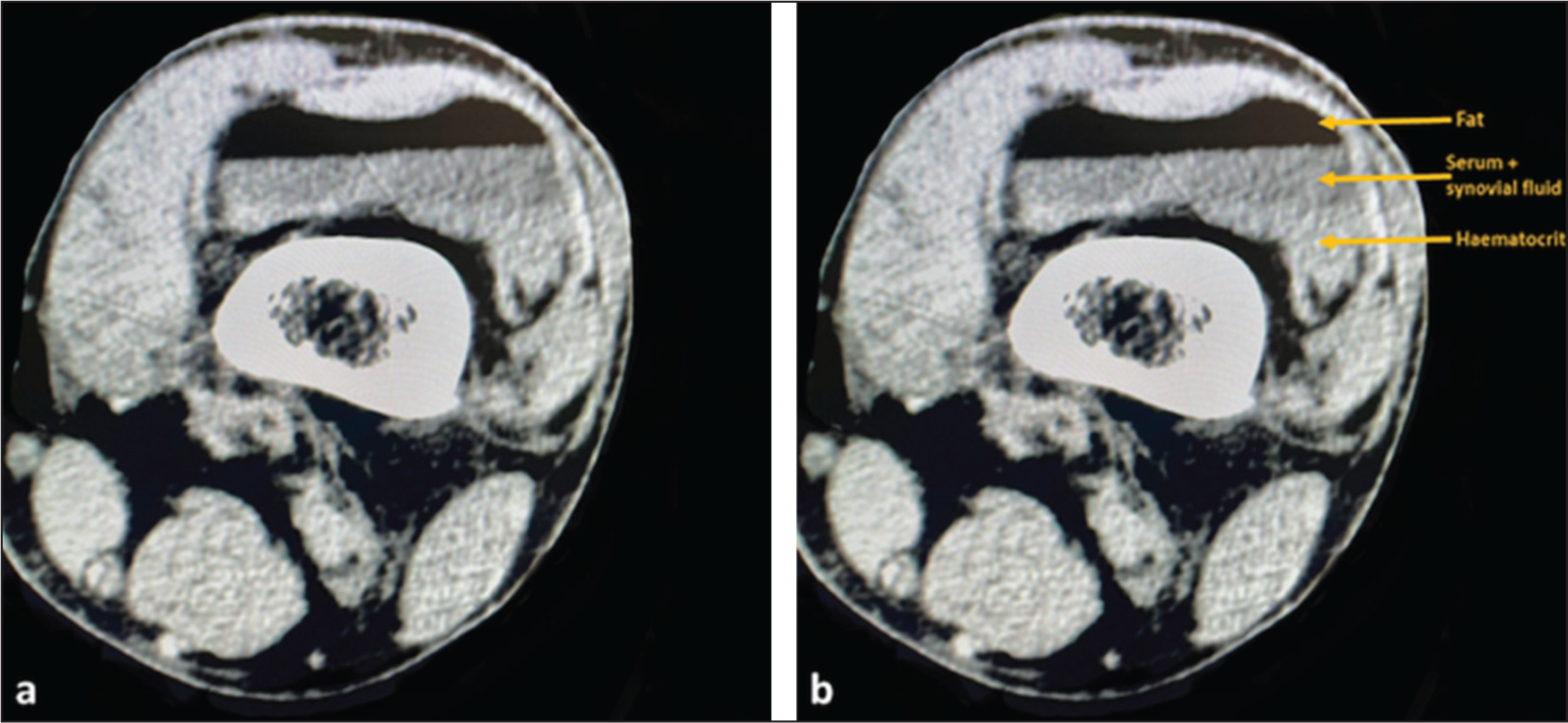
Lipohaemarthrosis results from the extrusion of fat and blood from the bone marrow into a joint space in the setting of an intraarticular fracture,[1,2] and, as such, this finding, when encountered on imaging, is almost pathognomonic for an intraarticular fracture. In the knee, lipohaemarthrosis has a specificity of 88.6% for intra-articular fractures and is observed in 27.1% of such fractures.[3] Fat, due to its hydrophobic nature, naturally separates from fluid and blood.[4] Owing to differences in density of the marrow fat and blood products, with fat being less dense than blood, the extruded fat in the joint floats to the top of the blood products and synovial fluid under the influence of gravity. Given that fat also has a lower attenuation value compared to that of synovial fluid or blood, a ‘fat-fluid’ level is identified in a horizontal cross-table lateral radiograph of the affected joint.[5] Owing to the more detailed fluid and tissue characterisation provided by computed tomography (CT) and magnetic resonance imaging (MRI), a ‘triple layer’ is often seen with these imaging methods, representing fat, serum/synovial fluid, and haematocrit, respectively[4] [Figure 1a and 1b].
(a and b) Axial CT images of a patient with a tibial plateau fracture demonstrating a lipohaemarthrosis, with the classically described ‘triple layer’ consisting of fat, synovial fluid, serum and haematocrit
Although most descriptions of lipohaemarthrosis focus on the knee joint, similar fat-fluid or fluid-fluid layering phenomena have been reported in other large synovial joints, including the hip, elbow and shoulder, particularly in the context of intra-articular fractures. In these joints, the appearance and orientation of layering have been shown to vary depending on joint volume, capsular anatomy, and patient positioning at the time of imaging.[6,7] These reports suggest that factors beyond gravity alone may influence the behaviour of intra-articular contents, raising the possibility that similar mechanisms operate within the knee joint.
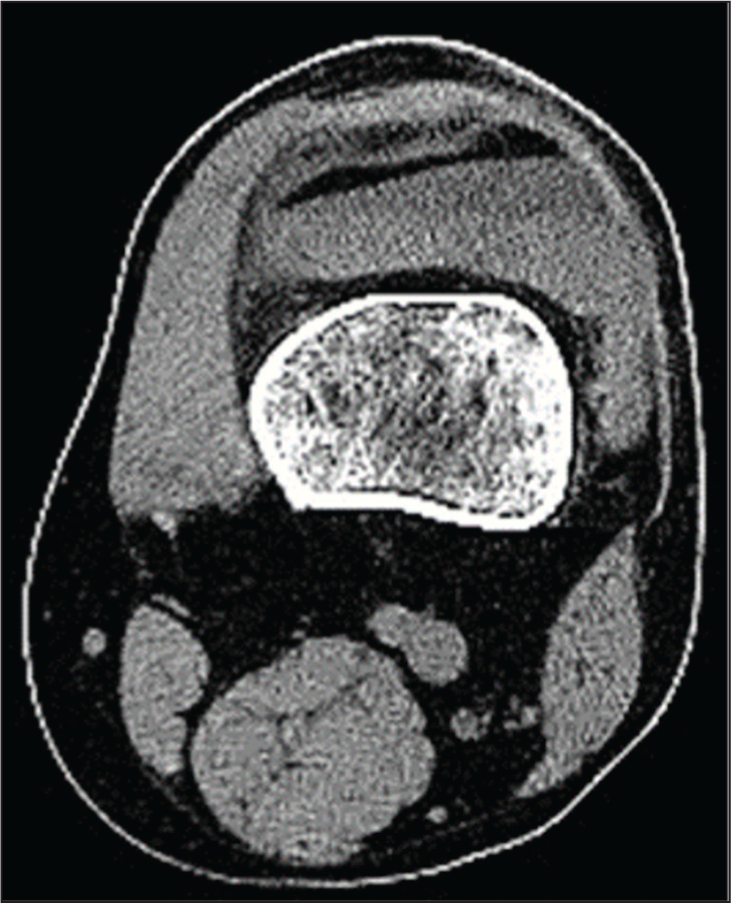
Traditionally, the behaviour of the contents within a joint in a lipohaemarthrosis has been thought to be substantially influenced by gravity, resulting in the appearance of layers of fat, serum/synovial fluid, and haematocrit parallel to the horizontal plane. In the authors’ collective experience interpreting a large volume of cross-sectional imaging of cases with a traumatic lipohaemarthrosis of the knee, however, it has been noticed that the layering of the contents does not always conform to the effects of gravity, with the layers in some instances oriented at varying angles to the horizontal plane. An example of this is provided in Figure 2. This suggests a more complex interplay of factors governing the behaviours of the intraarticular contents in cases of lipohaemarthrosis, rather than the effect of gravity alone. Our study aims to investigate this phenomenon by analysing the appearance of the layering contents of a lipohaemarthrosis in a series of patients with an intra-articular fracture of the knee.
Axial CT image demonstrating a lipohaemarthrosis in the suprapatellar pouch in a patient with an intra-articular (tibial plateau) fracture. Note the gravity-independent layering of the three components at varying angles to the horizontal plane
Materials and Methods
Study Design and Patients
The study was performed in accordance with the relevant ethical guidelines of our institution, with the approval of the ethics committee. A retrospective analysis of 30 CT scans of the knee in patients with acute trauma and a lipohaemarthrosis was performed at a tertiary orthopaedic centre. Only those studies demonstrating a ‘triple layer’ were included [Figures 1 and 2]. All of the patients had a radiograph of the knee (a minimum of standard anteroposterior and lateral views) prior to the CT scan. All of the CTs were performed with the knee in complete extension and the patient lying supine. The images were analysed independently by two musculoskeletal radiologists with a combined experience of over 15 years.
Image Analysis
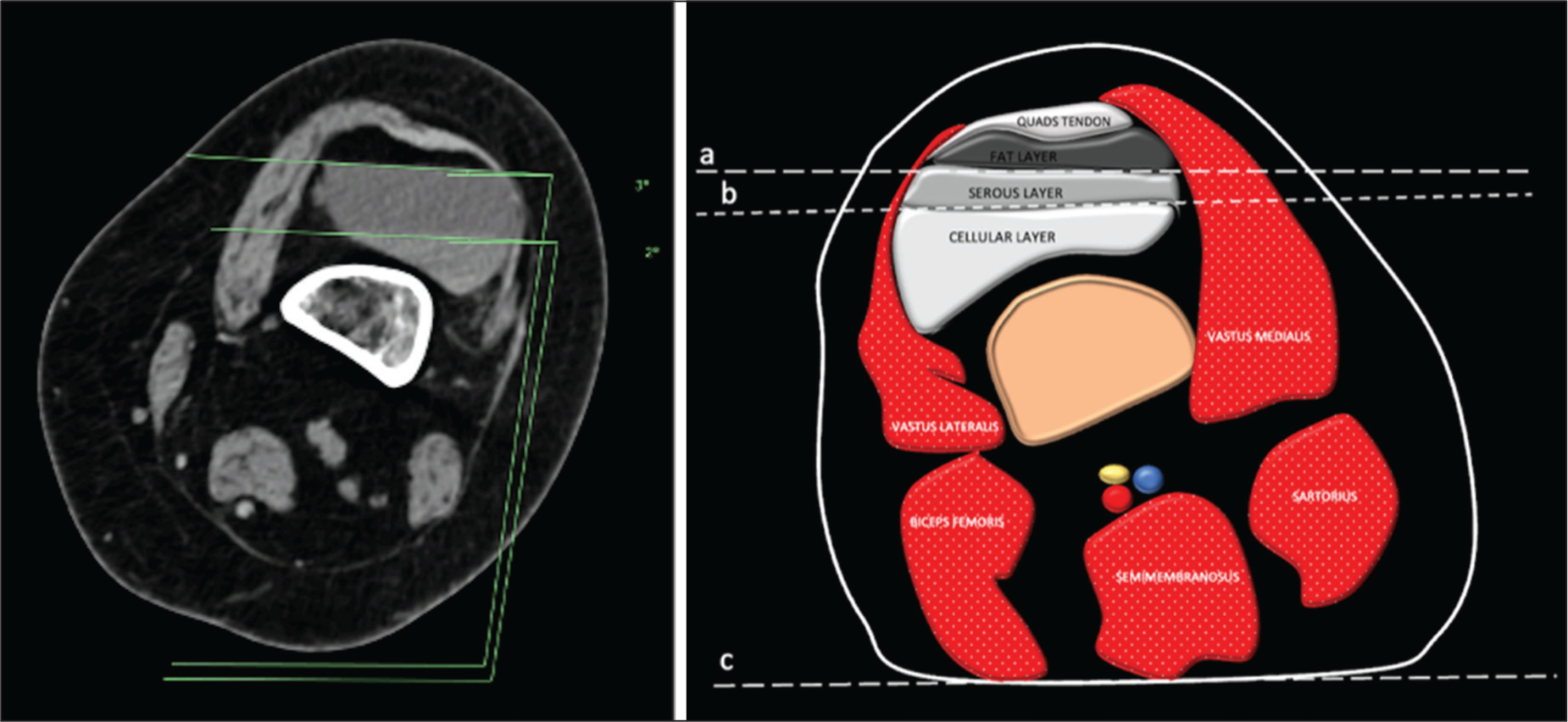
The angles between the horizontal plane and the two interfaces between the three-layered components of the lipohaemarthrosis were measured (Angles 1 and 2) [Figure 3]. The measurements were performed in the axial plane in which the lipohaemarthrosis was at its greatest depth (typically at the level of the suprapatellar pouch). The rotation of the knee in the axial plane relative to the horizontal plane was also measured. For the purposes of this analysis, lateral rotation of the knee was taken to be a negative angle; positive angles represented medial rotation. The nature of the intra-articular fractures was also recorded.
Annotated diagram demonstrating the measurements of the angles between the horizontal plane and the two interfaces between the three layers of the lipohaemarthrosis (Angles 1 and 2, in this case 3 and 2 degrees, respectively) (a) and schematic (b)
Data Collection
Microsoft Excel data sheet was used for data collection.
Statistical Analysis
Statistical analysis and graph creation were performed in STATA (Release 18, Stata Corp LLC, College Station, TX, USA). Descriptive statistics, including the average (mean) angles and standard deviations, were used to describe the angle measurements. The correlation between angles was assessed using Pearson’s correlation coefficient (linear correlation). Intra- and inter-observer reliability was assessed using the intra-class correlation coefficient (ICC 2,1).
Results
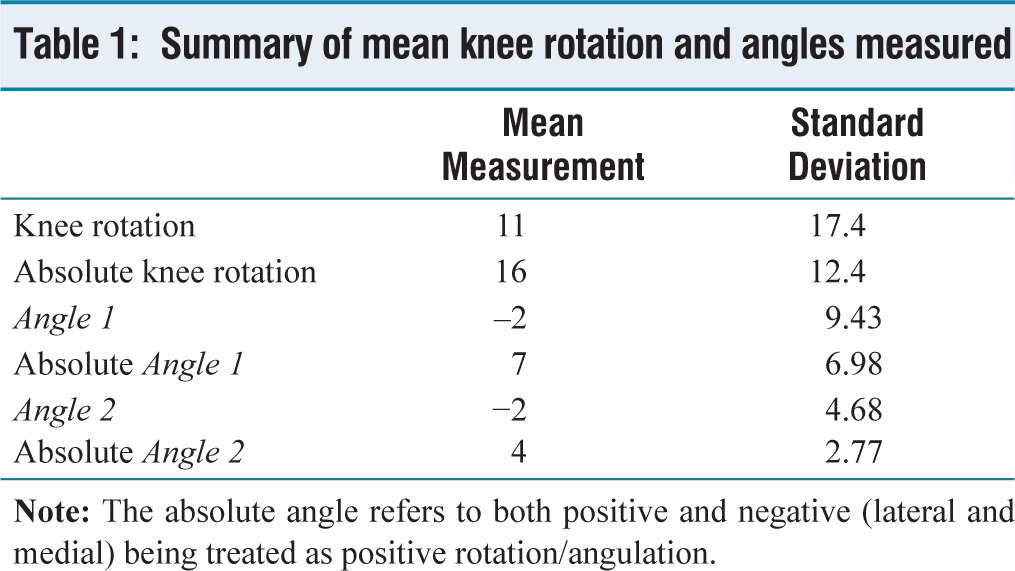
The study included 30 patients, 21 (70%) of whom were male. The mean age of participants was 39.4 years (inter-quartile range 29.3–46.5 years). Seventeen patients sustained a tibial plateau fracture, six patients sustained a patellar fracture, and seven patients sustained a femoral condylar fracture. In 28 of 30 (93.3%) patients, the fracture was visible with conventional radiography; in all patients, the fracture was visible on CT. In 21 (70%) patients, the subsequent lipohaemarthrosis was visible with conventional radiography; the lipohaemarthrosis was visible on CT in all patients. The CTs were acquired with a mean knee rotation of 11 degrees (SD 17.4); this value was reduced because examples of both medial and lateral rotation of the knee were observed in our patients. Mean deviation from horizontal was 16 degrees (SD 12.4). The mean Angle 1 was −2 degrees (SD 9.43), and the mean Angle 2 was −2 degrees (SD 4.68). The mean angle values were also low because examples of both lateral and medial angulation were observed in our patients. The mean deviation from horizontal for Angle 1 was 7 degrees (SD 6.98), and the mean deviation from horizontal for Angle 2 was 4 degrees (SD 2.77). Angle 1 was not perfectly horizontal (0 degrees) in every single patient, and Angle 2 was horizontal only in two patients. In summary, there was not a single study in which the three layers of the lipohaemarthrosis were perfectly horizontal. Table 1 provides a summary of these results. There was excellent intra-observer and inter-observer reliability for the measurement of all angles. Intra-observer reliability ICC for knee rotation, Angles 1 and 2 was 0.996, 0.986 and 0.994, respectively. Inter-observer ICC was 1, 0.975 and 1, respectively.
Summary of mean knee rotation and angles measured
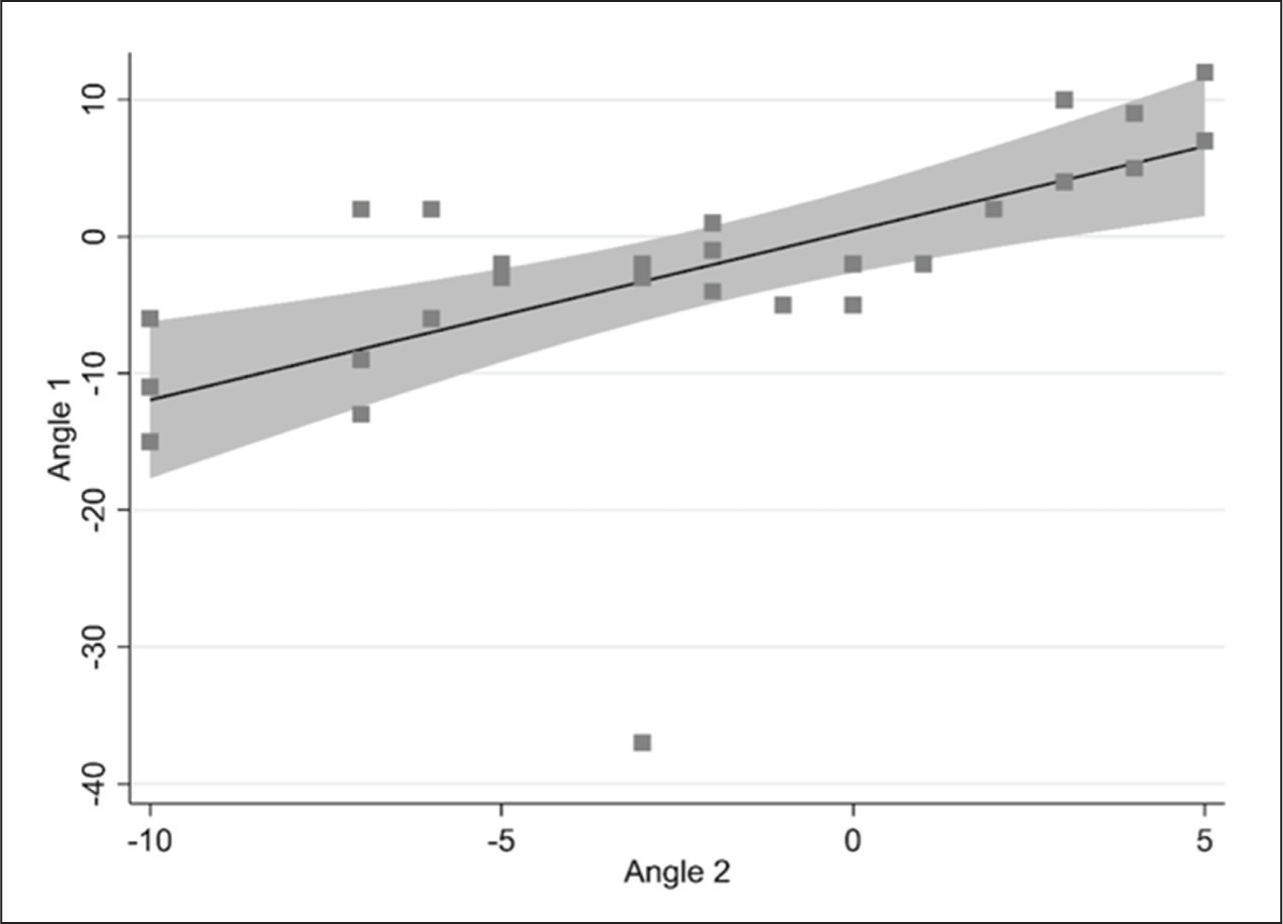
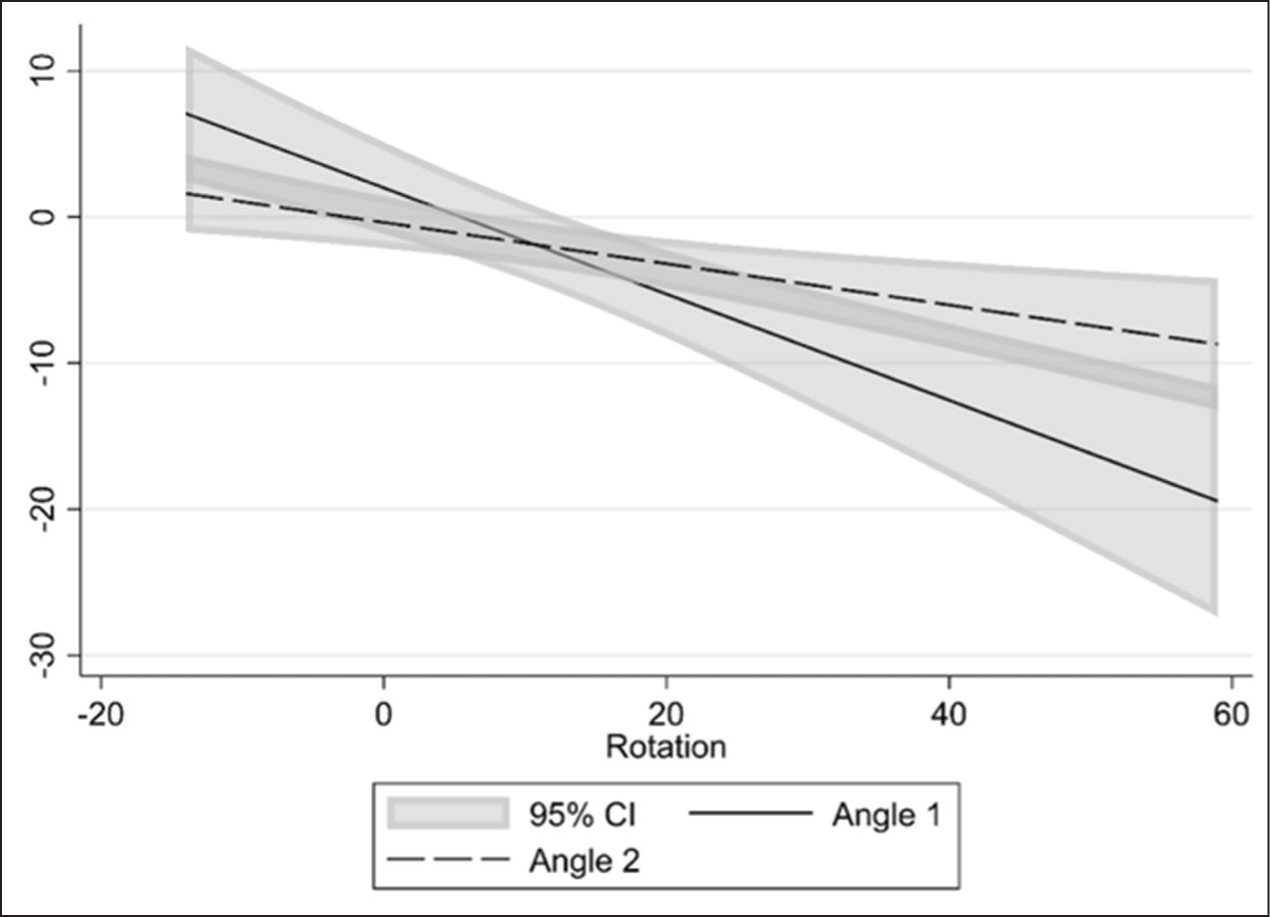
Parameters of knee rotation, Angles 1 and 2, were found to be highly correlated. The correlation coefficient between Angles 1 and 2 was 0.613 (P = .0003), the correlation between Angle 1 and knee rotation was −0.672 (P < .0001), and the correlation between knee rotation and Angle 2 was −0.572 (P = .0028). Figures 4 and 5 demonstrate the correlation between rotation and angles, along with confidence intervals.
The correlation between Angles 1 and 2. The line represents the best-fit linear regression with 95% confidence intervals
The correlation between Angles 1 and 2> and the rotation of the knee. The two lines represent the best-fit linear regressions along with 95% confidence intervals
Discussion
The results of the study demonstrate that all three layers in a lipohaemarthrosis are essentially never perfectly horizontal. Additionally, the results demonstrate that there is a strong correlation between the angulations of the interfaces between the three layers. Further, the results indicate that the angulation of the interfaces between the layers is strongly correlated to the rotation of the knee at the time of the study.
Several factors may contribute to the aforementioned gravity-independent layering of the contents of a lipohaemarthrosis. Complex interactions between the fat, synovial fluid/serum and blood components, as well as the formation of fibrin and other cellular elements, may impact the behaviour of the fluid levels, preventing the clear stratification of the components under the influence of gravity. The viscosity of the contents may also play a role; the bottom layer, being the haematocrit, is substantially more viscous than the superficial layering of synovial fluid, serum and fat components, and it may resist easy stratification under gravity. This could result in the non-parallel alignment of the fluid layers, particularly if the patient has been moved immediately prior to the scan being performed. The knee joint capsule and, in particular, the suprapatellar pouch, where the lipohaemarthrosis is typically observed, is not always a continuous space. Congenital thickening and folding of the synovial membranes occur, resulting in the formation of plicae.[8] These may also impede the normal gravity-dependent layering of components. Furthermore, structural asymmetry exists between the medial and lateral aspects of the knee joint and the suprapatellar pouch,[9] which can result in variations in the hydrostatic pressure within the joint cavity, potentially leading to differential distribution and displacement of the contents of a lipohaemarthrosis. It is also possible that additional factors, such as the paramagnetic properties of blood and the influence on it by an external magnetic field, given the known diamagnetic behaviour of erythrocytes,[10] may play a potential role when this phenomenon is observed on MRI.
In addition to viscosity-related effects, the temporal evolution of intra-articular haemorrhage may further influence layering behaviour. Partial clot formation and progressive sedimentation of cellular blood components can alter density gradients over time, resulting in irregular or non-horizontal interfaces. Variations in the relative proportions of fat, serum, and cellular elements between patients may also contribute to differences in layering appearance. Together, these factors highlight that the intraarticular environment in acute trauma is dynamic rather than static, and that imaging findings may reflect a transient state rather than a simple equilibrium governed by gravity alone.
A number of pathological conditions and imaging artefacts can mimic the appearance of layered intra-articular contents. Proteinaceous or haemorrhagic effusions without fat, lipoma arborescens, synovial chondromatosis, and layering of intra-articular contrast following arthrography may produce fluid-fluid or fat-fluid interfaces.[11,12] In addition, chemical shift artefact and partial volume averaging can exaggerate or simulate layering, particularly on cross-sectional imaging. Careful assessment across imaging planes, correlation with clinical context, and evaluation of signal characteristics across sequences are essential to distinguish true lipohaemarthrosis from these mimics.
Given the strong statistical correlations between the angulations of the interfaces between the three layers, and their strong correlation with the knee rotation, it can be reasonably inferred that the gravity-independent layering of the three layers in our study was probably related to patient positioning prior to the CT scans being undertaken and the effect of the viscosity of the contents as described above.
This phenomenon has direct implications for clinical practice, particularly in the radiographic assessment of suspected intra-articular fractures. Gravity-independent layering may obscure classical fat-fluid levels on lateral radiographs, potentially reducing sensitivity for detecting lipohaemarthrosis. In the present study, lipohaemarthrosis was visible on radiographs in only 70% of cases. Awareness of this variability may prompt a lower threshold for cross-sectional imaging when clinical suspicion remains high despite negative or equivocal radiographs. Furthermore, if viscosity-related effects contribute to altered layering, allowing time for intraarticular contents to stabilise prior to obtaining lateral radiographs—particularly after patient movement—may improve detection rates and reduce diagnostic delay.
Our study had several limitations, which include the relatively small sample size. The analysis was also performed based on CT findings alone, as CT scans of the knee were more frequently performed in the setting of acute trauma compared to MRI at our institution. Further studies with larger sample sizes analysing a combination of imaging modalities, including CT, MRI and ultrasound, may lead to a better understanding of the underlying mechanism of this phenomenon.
Conclusion
The contents of a traumatic lipohaemarthrosis within the knee joint are not always gravity dependent as previously thought. We hypothesise that a complex interplay of factors within the joint space can result in this phenomenon. Our results suggest that the viscosity of the contents (particularly related to patient movement prior to the imaging study) may play a role. This could have important implications in the radiological assessment of a lipohaemarthrosis.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors Rajesh Botchu and Karthikeyan P Iyengar are members of the Editorial Board of Apollo Medicine. The authors did not take part in the peer review or decision-making process for this submission and have no further conflicts to declare.
Funding
The authors received no financial support for the research, authorship and/ or publication of this article.
Institutional ethical committee approval
Ethical approval number not obtained for this study, as it involved the analysis of non-identifiable data only and did not include any information that could lead to patient identification.
Informed consent
Informed consent was not required, as all data were fully anonymized and no identifiable patient information was included.
Credit author statement
Conception and design, or acquisition of data, or analysis and interpretation of data: Ariyaratne S, Resnick D, Botchu R.
Design, or acquisition of data, or analysis and interpretation of data: Ariyaratne S, Mittal AK, Raniga SB, Botchu R.
Drafting the article or revising it critically for important intellectual content: Ariyaratne S, Mittal AK, Raniga SB, Davies AM, Resnick D, Botchu R.
Final approval of the version to be published: Ariyaratne S, Mittal AK, Raniga SB, Davies AM, Resnick D, Botchu R.
Data availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request. Any shared data will be fully de-identified in accordance with institutional and privacy regulations.
Use of artificial intelligence
No artificial intelligence (AI) tools were used in the generation, analysis, or interpretation of the study data. AI-assisted tools were used solely for language editing and formatting of the manuscript. The authors take full responsibility for the content and accuracy of the work.