
Abstract
Introduction:
Psychodermatological conditions, involving psychiatric disorders like depression and anxiety with skin conditions, are often overlooked by healthcare professionals in India. Psychotropic drugs are vital in treatment, but limited studies assess their use and impact on quality of life. This study evaluates psychotropic drug usage, psychological distress, and quality of life in these patients.
Methodology:
An observational, cross-sectional study was conducted in the psychiatry outpatient department of a tertiary care hospital over one year. Patients of all ages and sexes, diagnosed with psychodermatological disorders and on psychotropic drugs, were included. Sociodemographic and medication data were collected from records. Patients reported dermatological reactions due to psychotropic drugs. Quality of life was assessed using the WHO QoL-BREF scale, and psychological distress with the Kessler’s distress scale.
Results:
Thirty patients were included. Aripiprazole (50%) and escitalopram (43.33%) were the most prescribed for primary and secondary psychiatric disorders, respectively. Clonazepam was the most common benzodiazepine (60%). Severe psychological distress was found in 55.17% of patients. The physical domain of the QoL-BREF scale was most affected in primary psychiatric disorders.
Conclusion:
Psychotropic drugs were prescribed based on symptoms. Patients experienced significant psychological distress and poor quality of life, with adverse drug reactions contributing to distress. Judicious use of psychotropic drugs is essential.
Introduction
Psychodermatology is a relatively new branch of dermatology in India,[1] which is a merger between dermatology and psychiatry, explaining how psychological stress can influence skin disease and the dermatological aspects of psychiatric diseases.[2] The prevalence of psychiatric disorders, like depression and anxiety, is quite high, ranging from 25% to 43% among patients with skin conditions.[3] Approximately 30%–40% patients seeking treatment for skin disorders have an underlying psychiatric or psychological problem that either causes or exacerbates a skin complaint.[4]
Psychodermatological diseases are not serious or life-threatening, so they do not receive much attention from doctors or healthcare policy makers and funds are mainly diverted to the serious illnesses. However, their psychosocial impact is more than other chronic or life-threatening illnesses, which leads to poor quality of life among these patients. Psychocutaneous disorders can be categorised into four categories by the underlying psychiatric disorder that contributes to the skin conditions.[5]
European studies have reported that patients with atopic eczema, hand eczema, acne and hidradenitis suppurativa have an increased risk of depression.[6] After the ‘All-Party Parliamentary Group on Skin (APPGS)’s’ 2013 publication, public awareness was increased regarding the necessity to support people with mental health conditions. However, most patients with skin conditions and poor mental health are not able to access the specialist psychodermatology support required.[7] Thus, psychodermatology is a novel but essential area of research.
There is very little data available on drugs used in psychodermatological diseases. Individual disease studies, like in psoriasis they have reported poor quality of life, but a very small number of studies were found on the quality of life of psychodermatological disease patients. Another area less explored is the psychological distress affecting the patient’s feelings. Hence, the present study is done to evaluate the drugs used in psychodermatological diseases, along with an assessment of psychological distress and quality of life.
Methodology
It was an observational, cross-sectional study conducted in patients diagnosed with psychodermatological disorders attending the psychiatry outpatient department, over a period of one year, after obtaining permission from the Institutional Ethics Committee (Approval number-PDUMC/IEC/42/2022).
Selection Criteria
Patients of either sex and all ages diagnosed with psychodermatological disease receiving psychotropic medications were included in the study after obtaining written informed consent. We have included patients with primary and secondary psychiatric disorders, along with patients who have developed dermatological side effects due to psychotropic medications. Patients were selected based on convenience sampling. Primary psychiatric disorders include patients having a psychiatric component as primary, and all skin manifestations were secondary, like in delusional parasitosis and trichotillomania, and the patients of secondary psychiatric disorders include patients suffering from psoriasis, acne, alopecia areata, etc., in which psychiatric conditions like depression & anxiety are the consequence of the disfiguring skin diseases. Psychiatric diseases were diagnosed by a psychiatrist using DSM-5 criteria.
Data Collection
A case record form (CRF) was designed to include information regarding patients’ demographic details (age, sex, education, marital status & family history), duration of psychiatric or dermatological diseases and drugs used. WHO QoL BREF[8]scale and Kessler’s psychodermatological distress scale[9]were used to assess quality of life and psychological distress, respectively.
Assessment Tools
We used the validated Gujarati (local language) version of the WHO QoL-BREF to assess the quality of life. This scale consists of 26 items assessing QoL in four dimensions: physical, psychological, social, and environmental QoL. Each item is rated on a 5-point scale. Scores are transformed on a scale from 0 to 100, with higher scores indicating higher QoL. We used Kessler’s psychodermatological distress scale, consisting of 10 questions which the patient answered during the last 4 weeks was asked and accordingly score was given from one to five. The total score was the summation of the individual question’s score. The final score was then categorised into mild, moderate and severe.
Statistical Analysis
Sample size was based on the number of patients that could be enrolled over a one-year duration. Recorded data were analysed by descriptive statistics like percentage, mean & standard deviation in MS Excel 2019 and Epi Info software version 7.2.
Results
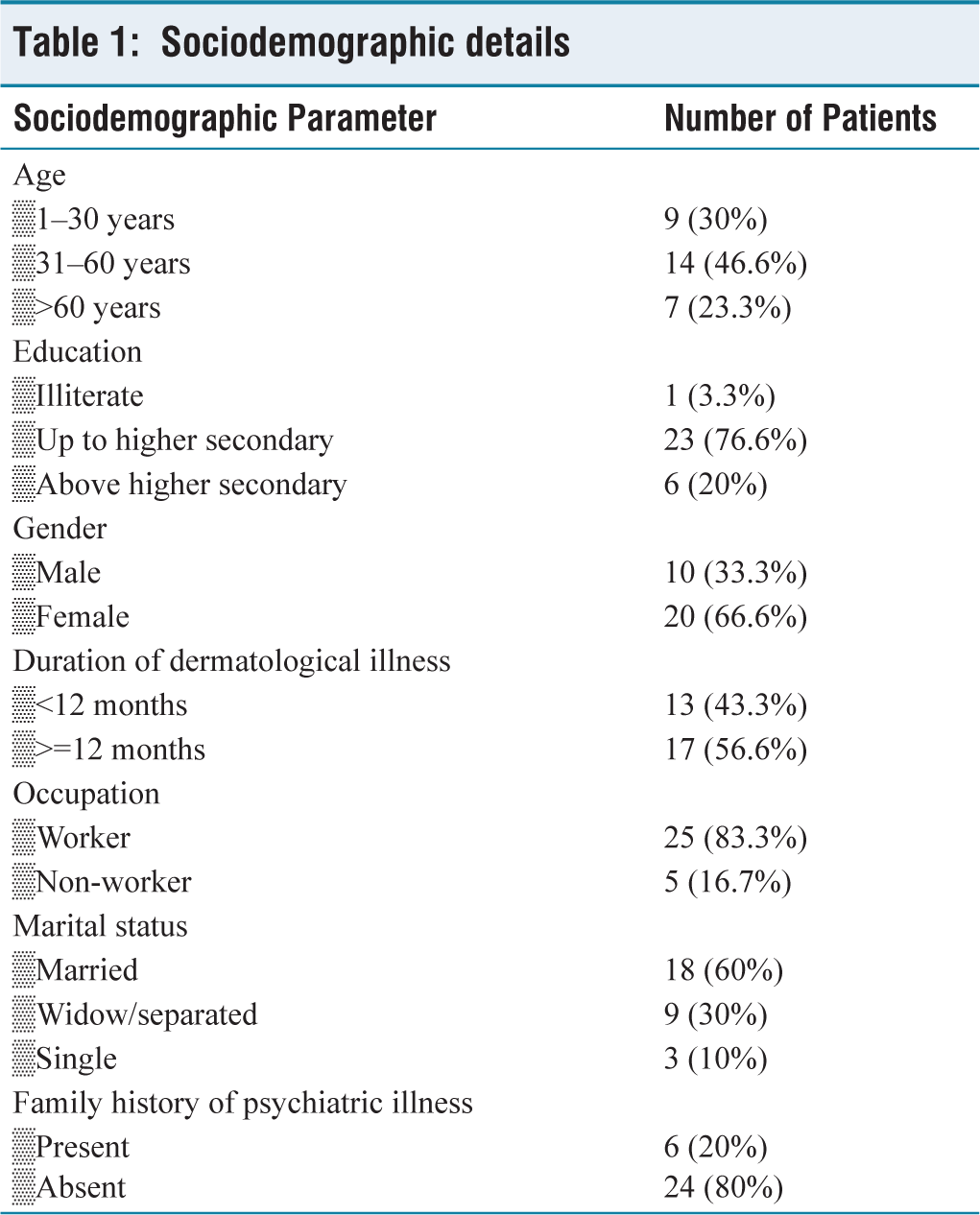
Among the 30 patients enrolled, there were 10 (33.33%) males and 20 (66.67%) females. The majority of patients were in the age group of 31–60 years. Sociodemographic details are given in Table 1.
Sociodemographic details
Out of 30 patients, six patients had primary psychiatric disorders, 20 patients had secondary psychiatric disorders, and four patients had dermatological side effects of psychotropic medications. Among the secondary psychiatric disorders, 10 patients were diagnosed with depression, and seven patients were diagnosed with anxiety disorder [Figure 1].
Diagnosis of illness

Table 2 shows drugs used in psychodermatological disorders. Among the antipsychotics, aripiprazole was most commonly prescribed (50%) in primary psychiatric disorders, followed by olanzapine. Among SSRIs, escitalopram was most commonly prescribed (43.33%), followed by fluoxetine in secondary psychiatric disorders. Among the benzodiazepines, clonazepam was most commonly prescribed (60%).
Drugs used in psychodermatological disorders
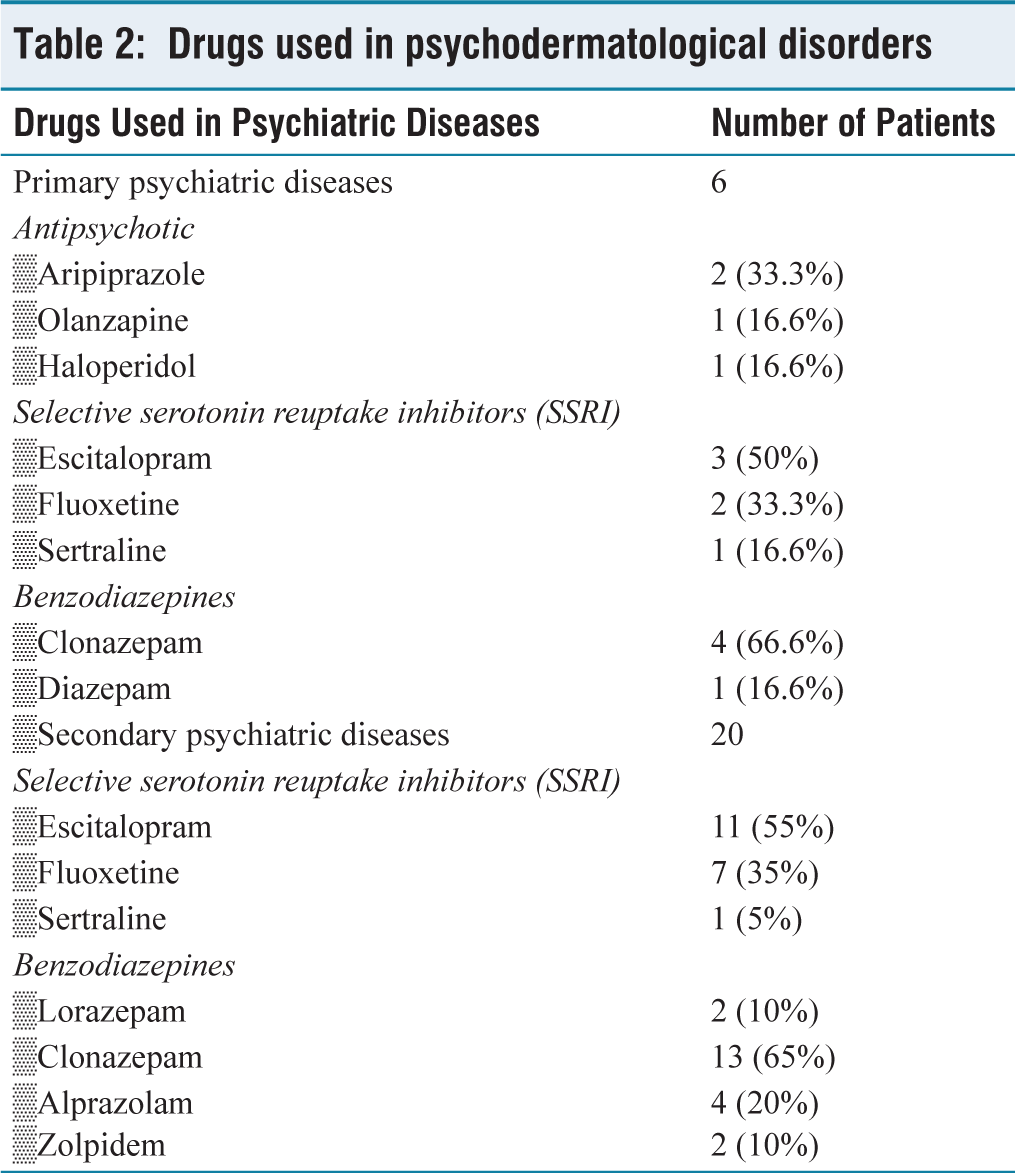
Table 3 shows patients with dermatological side effects of psychotropic medication causing distress in them.
Dermatological adverse drug reaction due to psychotropic medications
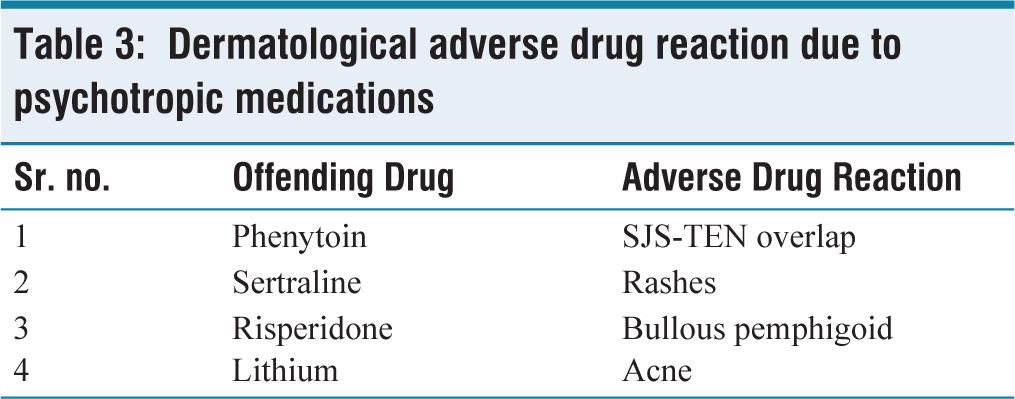
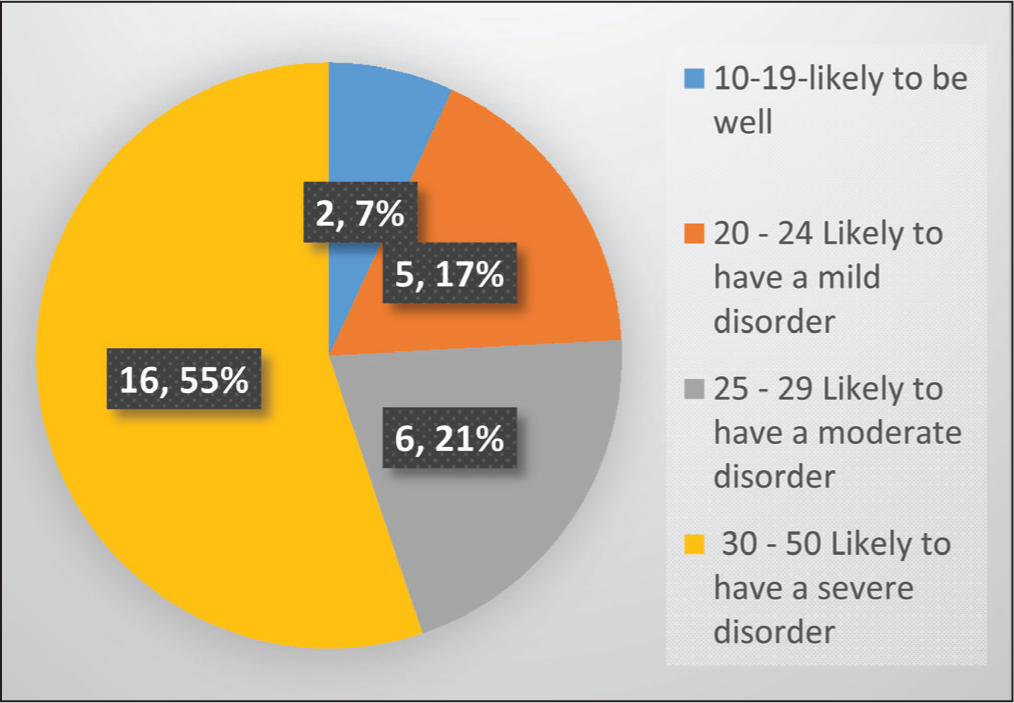
Figure 2 shows, 16 (55.17%) patients had severe psychological disorder according to Kessler’s psychological distress scale.
Assessment of psychological distress with Kessler’s psychological distress scale
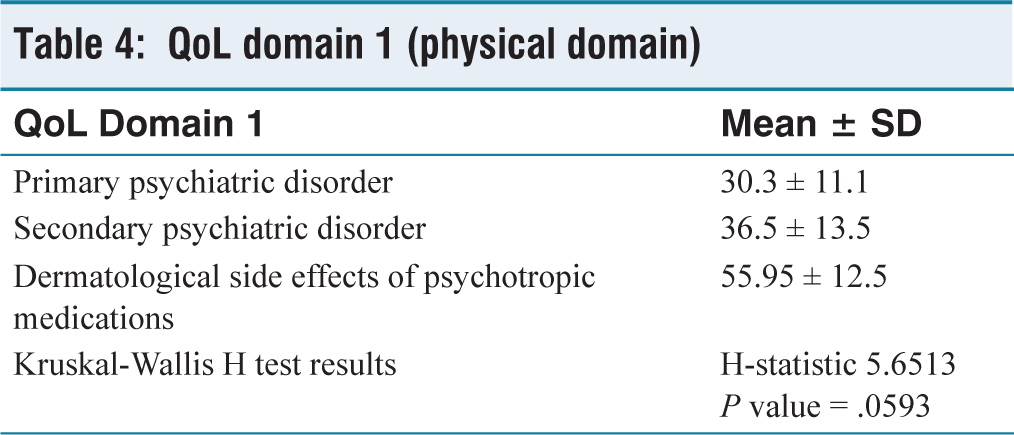
In QoL-BREF, the physical domain showed no significant difference among groups. Details of domain 1 are depicted in Table 4.
QoL domain 1 (physical domain)
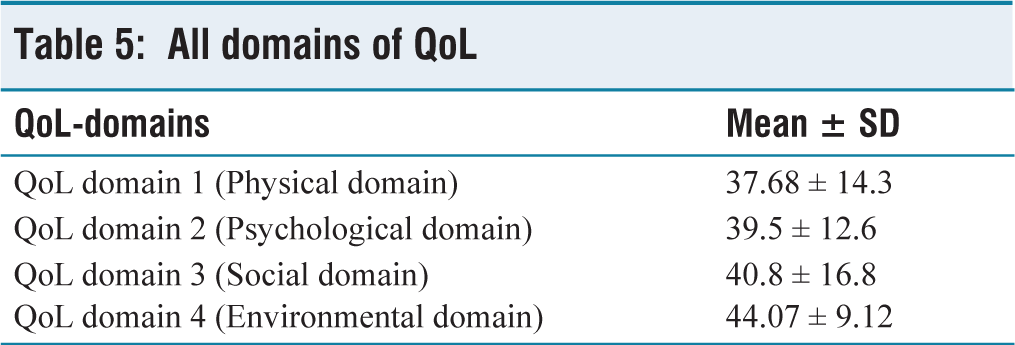
As shown in Table 5, all domains were affected by the disease process and the physical domain was affected the most, which includes parameters like pain, discomfort, energy level, fatigue, sleep and rest.
All domains of QoL
Discussion
Since the skin and psyche share a closely intertwined bond by sharing a common ectodermal origin, managing a chronic skin disorder is incomplete without caring for the mental health of the patient.[10,11]
In our study, the prevalence of psychodermatological disease is higher among females, which is similar to the study done by Picardi et al.[4] and Zachariae et al.[12] The reason is that females are more concerned about their appearance. However, there was no significant difference in the quality of life between the genders in our study. A similar result was found in the study done by Zachariae R.[12] Most of the patients belonged to the 31–60 years. It was observed that patients with dermatological illnesses of more than one year duration had more psychological distress. In our study, five patients lost their work due to psychological problems, which caused financial burden, leading to further psychological distress and thus a vicious cycle was set in.
There are pharmacological and non-pharmacological interventions for patients having psychodermatological problems.[10,13]A lot of non-pharmacological interventions have been tried successfully for these problems, like hypnosis, biofeedback, meditation, behavioural therapy and have been found useful in various diseases like eczema, hyperhidrosis, urticaria, rosacea, lichen planus and vitiligo.[10]
In pharmacological intervention, for treating anxiety, benzodiazepines or buspirone or antidepressants with anxiolytic effects can be used. In our study, benzodiazepines were prescribed to 86.67% patients with anxiety, distress & impaired sleep related to psychodermatological disorders. For the depressed patients with neurotic excoriations, tricyclic antidepressant doxepin can be used, which has an additional antipruritic effect. Other antidepressants like fluoxetine, escitalopram, venlafaxine and bupropion can be used in secondary psychiatric disorders.[14] In our study, escitalopram was most commonly prescribed, followed by fluoxetine, in secondary psychiatric disorders. In primary psychiatric disorders, antipsychotic medications like olanzapine, aripiprazole, risperidone, and pimozide are most frequently used, whereas in our study, aripiprazole and olanzapine antipsychotic were most commonly prescribed.
In our study, among the four patients who developed dermatological adverse drug reactions (ADRs) due to psychotropic medications, two patients had mild ADR like rashes and acne, one patient had a very severe reaction like SJS-TEN overlap (Stevens-Johnson syndrome and toxic epidermal necrolysis overlap), and one had bullous pemphigoid, which suggests that psychotropic medications should be judiciously used.
Among all patients who were interviewed, the majority, 16 (53.3%) of the patients had severe mental distress scores based on the Kessler classification scale. A similar result was found in Laura Dixon et al., in which anxiety severity was very high in psychodermatological diseases.[15] Additionally, the immense emotional distress that vitiligo patients often experience has been shown to interfere with employment, cause social withdrawal due to fear of rejection, and has been shown to lead to substance-use disorder, as reported by Parsad D.[16]
QoL-BREF score contains physical, psychological, social and environmental domains. Among all domains, physical QoL has the lowest mean score of 37.68 (SD =14.3), followed by psychological QoL with a mean score of 39.5 (SD =12.6). This suggests that physical health, body image and concentration are relatively more affected than other domains of quality of life among psychodermatological disease patients. Bonotis et al. investigated that vitiligo impairs their quality of life of patients to a greater extent.[17] Quality of life is decreased, which may be due to embarrassment, stigma, low self-esteem, social withdrawal, Frustration, and hopelessness experienced by psychodermatology patients.
Future Directions
With growing awareness and research in psychodermatology, there is an opportunity to identify gaps in dermatologists’ knowledge and improve services through better coordination between dermatology and psychiatry. Setting up psychodermatology clinics can enhance patient care. Including psychodermatology in residency training and developing internationally recognised programmes in psychotherapy for dermatologists could further strengthen this field.
Strengths
Our study can be a trigger to understand the need to pay more emphasis on the psychodermatology, drugs used in this condition, quality of life and psychological distress these patients are facing.
Limitations
There are certain limitations of our study. One is a cross-sectional study. Longitudinal, prospective studies are needed to see the development & cure rate among psychodermatological disorders. Another limitation is the small sample size. Large-scale studies are required to generalise the findings of our study.
Conclusion
Our study found that patients with psychodermatological disorders were most commonly prescribed benzodiazepines, selective serotonin reuptake inhibitors (SSRIs), and atypical antipsychotics. However, these agents may act as a double-edged sword, as they can also induce dermatological ADRs. Therefore, non-pharmacological interventions should be prioritised whenever possible before initiating pharmacotherapy. Recognising psychodermatological interactions and fostering collaboration between dermatologists and psychiatrists are essential for effective management and improved patient outcomes.
Footnotes
Acknowledgements
We would like to acknowledge our participants for contributing their valuable time.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Permission obtained from the Institutional Ethics Committee (Reference Letter No-PDUMCR/IEC/42/2022).
Credit author statement
All authors contributed significantly to the article.
RP: Primary manuscript draft and preparation of figures.
FC: Drafting and review.
AP: Supervision and final approval, proofreading.
AS: Supervision and final approval, proofreading.
Data availability
The authors confirm that the data supporting the findings of the study are available within the article and its supplementary files. Raw data that supports these findings are available with the corresponding author, upon reasonable request.
Use of artificial intelligence
No Artificial Intelligence was used.