
Abstract
Background:
Enhanced Recovery After Surgery (ERAS) improves outcomes in colorectal surgery, but whether its principles translate seamlessly to hepatopancreatobiliary (HPB) oncology, where pancreaticoduodenectomy (PD) and major hepatectomy carry unique physiologic hazards, remains uncertain.
Objective:
To synthesise contemporary evidence on ERAS in pancreatic and hepatic cancer surgery and determine if direct transfer from colorectal pathways is appropriate or if speciality-specific adaptation is required.
Methods:
Narrative review of ERAS Society guidelines, randomised trials, multicentre cohorts and systematic reviews/meta-analyses addressing prehabilitation and nutrition, goal-directed fluid therapy (GDFT), multimodal or regionally augmented analgesia, early feeding and mobilisation, selective drain and nasogastric (NG) management and integration with minimally invasive approaches. Outcomes included morbidity, length of stay, readmission, oncologic adequacy and timing of adjuvant therapy.
Results:
ERAS for pancreatic and liver resections is feasible and safe, shortening hospital stay by ~2–4 days and reducing complications by ~20%–30% without increasing readmissions or mortality. Oncologic metrics (microscopically margin-negative resection [R0] margin and nodal yield) are preserved and ERAS pathways more often enable initiation of adjuvant chemotherapy within 6–8 weeks. Translation is not uniform: Compliance, an independent determinant of benefit, tends to be lower in HPB (~60%–70%) than in mature colorectal programmes (≥80%–90%), largely due to caution with early oral intake, selective or early drain removal and fluid restriction. Patient factors common in HPB oncology (obstructive jaundice, cholangitis, sarcopenia and chemotherapy-related frailty) necessitate tailored prehabilitation and individualised fluid and analgesia strategies. Evidence for ERAS in biliary malignancies is promising but limited.
Conclusions:
ERAS principles are universal, but their execution in HPB oncology demands thoughtful adaptation. Precision-based pathways, digital tools to improve adherence, synergy with minimally invasive surgery and trials incorporating oncologic endpoints should define the next phase of ERAS in HPB cancer care.
Keywords
Introduction
Enhanced Recovery After Surgery (ERAS) represents a paradigm shift in perioperative medicine. Emerging from Henrik Kehlet’s pioneering work in the 1990s, ERAS demonstrated that multimodal strategies, including optimising analgesia, nutrition, mobilisation and fluid balance, could dramatically shorten hospital stay after colorectal surgery without increasing morbidity.[1] Building on this foundation, the ERAS→ Society, led by Kehlet, Fearon and Ljungqvist, formalised the first colorectal guidelines in 2005, creating a model that would spread globally.[2,3]
Within colorectal surgery, ERAS has matured into standard practice. Large systematic reviews and meta-analyses consistently show reduced postoperative complications, earlier return of bowel function and shorter hospital stays, often by 2–3 days, when protocols are implemented comprehensively rather than piecemeal.[4] This success naturally provoked the question: Can ERAS be transitioned seamlessly into hepatopancreatobiliary (HPB) oncology?
HPB resections pose a different order of magnitude in surgical stress. Pancreaticoduodenectomy (PD) is associated with delayed gastric emptying (DGE), pancreatic fistula and profound catabolic stress, while major hepatectomy can involve substantial blood loss, coagulopathy and postoperative liver dysfunction. In oncologic contexts, these challenges are compounded by malnutrition, cholestasis or immunosuppression from chemotherapy. Applying colorectal-derived ERAS protocols wholesale risks oversimplifying these complexities.
Recognising this, the ERAS Society released speciality-specific guidelines for liver resection (2016) and pancreatic surgery (2019).[5,6] Early evidence is encouraging. A 2019 meta-analysis of randomised controlled trials in PD reported reduced overall complications and length of stay without increasing readmission rates under ERAS protocols.[7] Similarly, systematic reviews of ERAS in hepatectomy show reductions in pulmonary complications, enhanced mobilisation and decreased hospital stay by nearly 3 days.[8] Yet heterogeneity remains: Compliance with ERAS pathways across centres is variable and not all components translate with equal benefit in HPB contexts.
This narrative review, therefore, addresses a critical question: Does ERAS truly translate seamlessly from colorectal to HPB oncology or do these protocols demand adaptation? By synthesising evidence, including randomised trials, meta-analyses and systematic reviews, we aim to provide a one-stop reference for ERAS in pancreatic, hepatic and biliary oncologic surgery. In doing so, we will explore where principles converge, where divergences demand caution and how future refinements may shape enhanced recovery in this uniquely demanding surgical domain.
Core Principles of Eras and Biological Rationale
ERAS hinges on taming the surgical stress response, a whirlwind of hormonal shifts, catabolism, insulin resistance, fluid imbalance and immunosuppression, that slows recovery. Multimodal strategies such as early feeding, minimised fasting, goal-directed fluid therapy (GDFT) and early ambulation have been shown to accelerate return to baseline physiology.[9,10]
Translating ERAS to HPB oncology requires nuance. Major liver resections involve significant blood loss, thermal dysregulation and risk of postoperative liver insufficiency. GDFT, balancing fluids with hemodynamic guidance, is crucial to avoid venous congestion while preserving tissue perfusion.[11] A randomised trial comparing GDFT with low central venous pressure (CVP) fluid restriction strategies found no significant differences in blood loss or morbidity, suggesting that HPB surgery resists ‘one-size-fits-all’ approaches.[12]
Pancreatic surgery brings its own complications, particularly DGE and pancreatic fistula. ERAS interventions such as early oral intake, selective drainage and avoidance of routine nasogastric decompression specifically address these problems.[13]
Effective analgesia is another cornerstone. Multimodal, opioid-sparing regimens, utilising thoracic epidurals, transversus abdominis plane (TAP) blocks and non-opioid adjuncts, reduce ileus, enhance mobilisation and blunt opioid-induced immunosuppression.[14] However, compliance with these strategies in real-world HPB settings remains variable, influenced by institutional anaesthetic practices.
Nutrition is equally critical. HPB oncology patients are often malnourished due to cachexia, biliary obstruction or chemotherapy. Prehabilitation and preoperative carbohydrate loading help counteract catabolic stress and immunonutrition has shown benefit in high-risk surgical cohorts.[15]
A consolidated mapping of ERAS domains to biological targets with HPB-specific adaptations is summarised in Table 1.
Core ERAS elements → biological target → HPB-specific adaptation
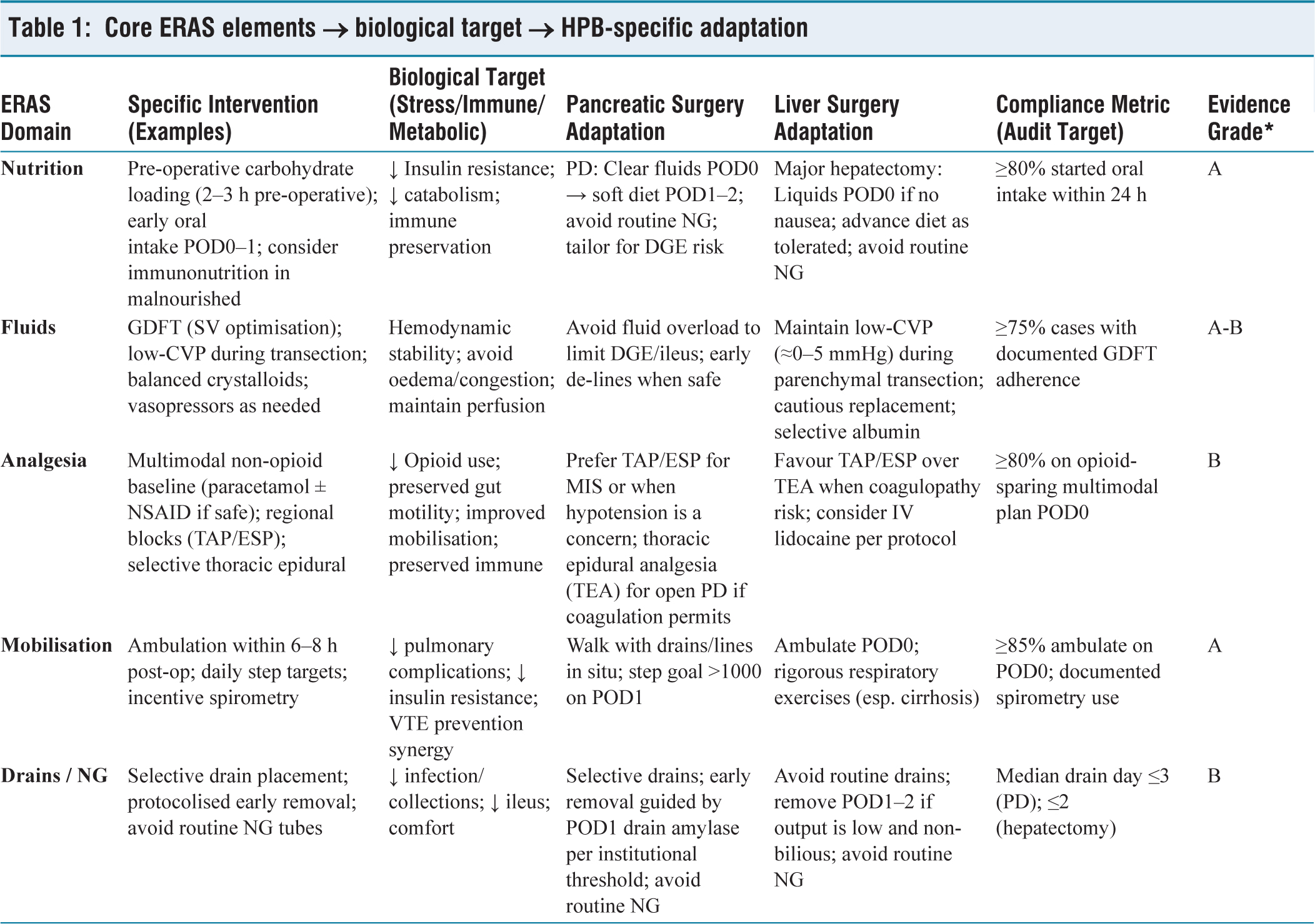
Final, enhanced recovery may influence oncologic outcomes. By reducing postoperative complications and accelerating recovery, ERAS can facilitate the timely initiation of adjuvant therapy and potentially improve long-term survival, reframing ERAS as not merely perioperative optimisation but also an oncologic strategy.[16]
Risk-stratified prehabilitation and nutrition bundles tailored to HPB oncology are outlined in Table 2.
Prehabilitation and nutrition bundles by risk stratum (HPB ERAS)
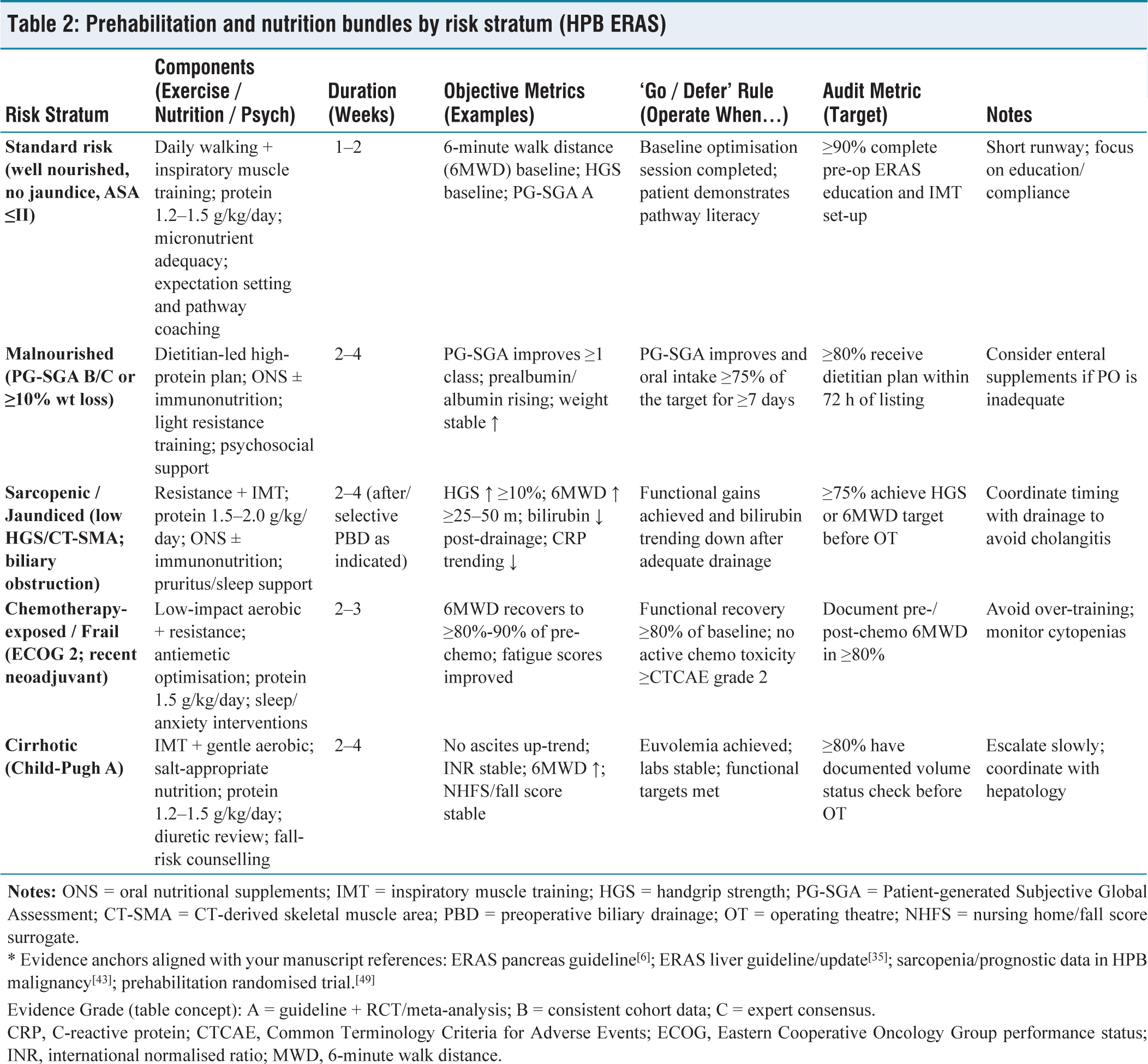
* Evidence anchors aligned with your manuscript references: ERAS pancreas guideline[6]; ERAS liver guideline/update[35]; sarcopenia/prognostic data in HPB malignancy[43]; prehabilitation randomised trial.[49]
Evidence Grade (table concept): A = guideline + RCT/meta-analysis; B = consistent cohort data; C = expert consensus.
CRP, C-reactive protein; CTCAE, Common Terminology Criteria for Adverse Events; ECOG, Eastern Cooperative Oncology Group performance status; INR, international normalised ratio; MWD, 6-minute walk distance.
Eras in Pancreatic Surgery
Pancreatic surgery, particularly PD, remains one of the most complex abdominal operations, with morbidity rates exceeding 40% despite advances in surgical technique and perioperative care. DGE, postoperative pancreatic fistula (POPF) and infectious complications remain major concerns.[17] The central question is whether ERAS pathways, so successful in colorectal surgery, can mitigate this burden in pancreatic oncology.
Evidence Base and Evolution
The ERAS Society issued its first speciality-specific guidelines for pancreatic surgery in 2019, providing structured recommendations for PD and distal pancreatectomy.[18] These emphasised preoperative counselling, minimisation of fasting, carbohydrate loading, opioid-sparing analgesia, early mobilisation and selective drain use. Unlike colorectal protocols, these guidelines accounted for complications unique to pancreatic surgery.
Multiple meta-analyses confirm that ERAS is safe and beneficial. A systematic review pooling randomised controlled trial (RCT)s and cohort studies found ERAS reduced overall morbidity by nearly 20%, pulmonary complications by 30% and shortened hospital stay by 2–4 days compared with conventional care.[19] Subsequent multicentre studies corroborated these results, reporting a faster return of bowel function, reduced infection rates and improved patient-reported outcomes under ERAS protocols.[20,21]
Pancreaticoduodenectomy
Specific ERAS measures directly target PD-associated complications. Early removal of nasogastric tubes reduces DGE and pulmonary morbidity.[22] Randomised evidence supports early oral intake as safe and effective, with no increase in POPF, while enhancing nutritional status and satisfaction.[23]
Drain management has shifted from routine use to selective, early removal. RCTs show that timely removal, guided by drain fluid amylase, reduces intra-abdominal collections and shortens stay.[24]
Analgesia is a critical component. Epidural analgesia, long considered standard, can delay mobilisation due to hypotension. Alternatives such as TAP blocks, erector spinae blocks or multimodal regimens maintain effective analgesia while facilitating earlier mobilisation.[25,26]
Technique selection within ERAS should prioritise opioid-sparing and hemodynamic stability; a practical comparison of options is shown in Table 3.
Analgesia strategies in HPB ERAS: Pros, risks and mobilisation impact
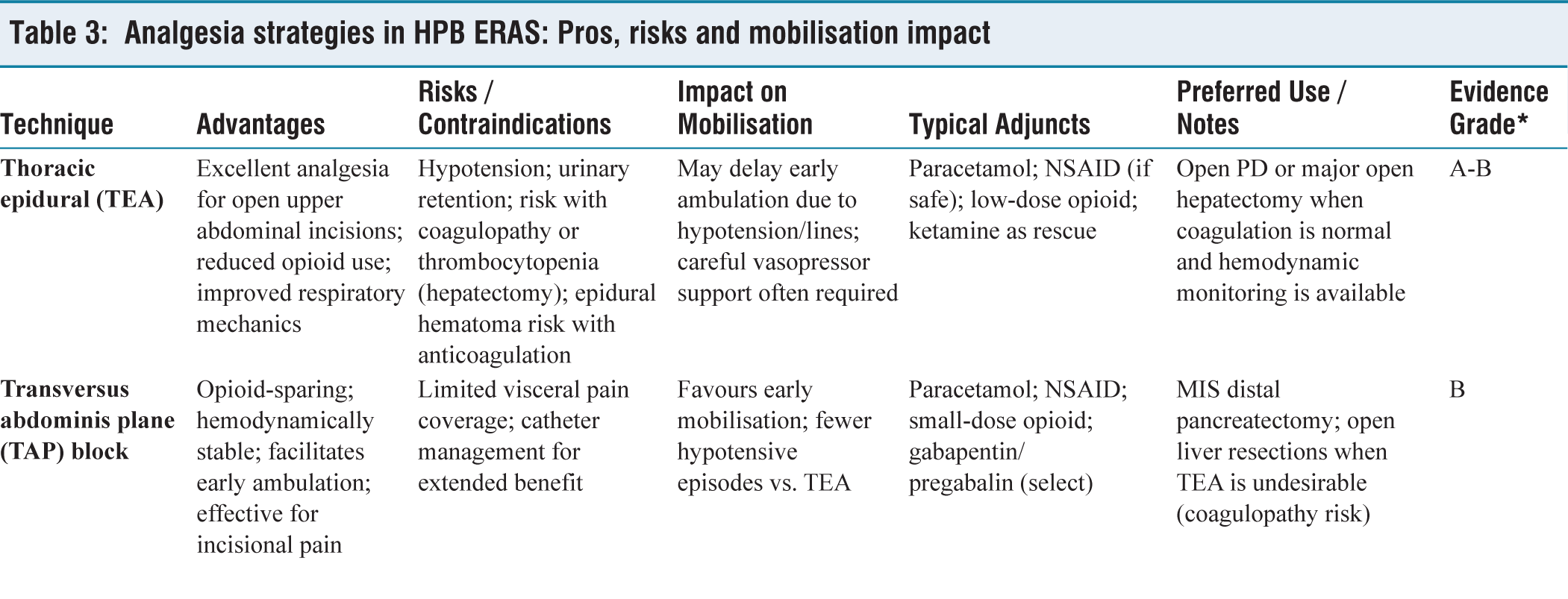
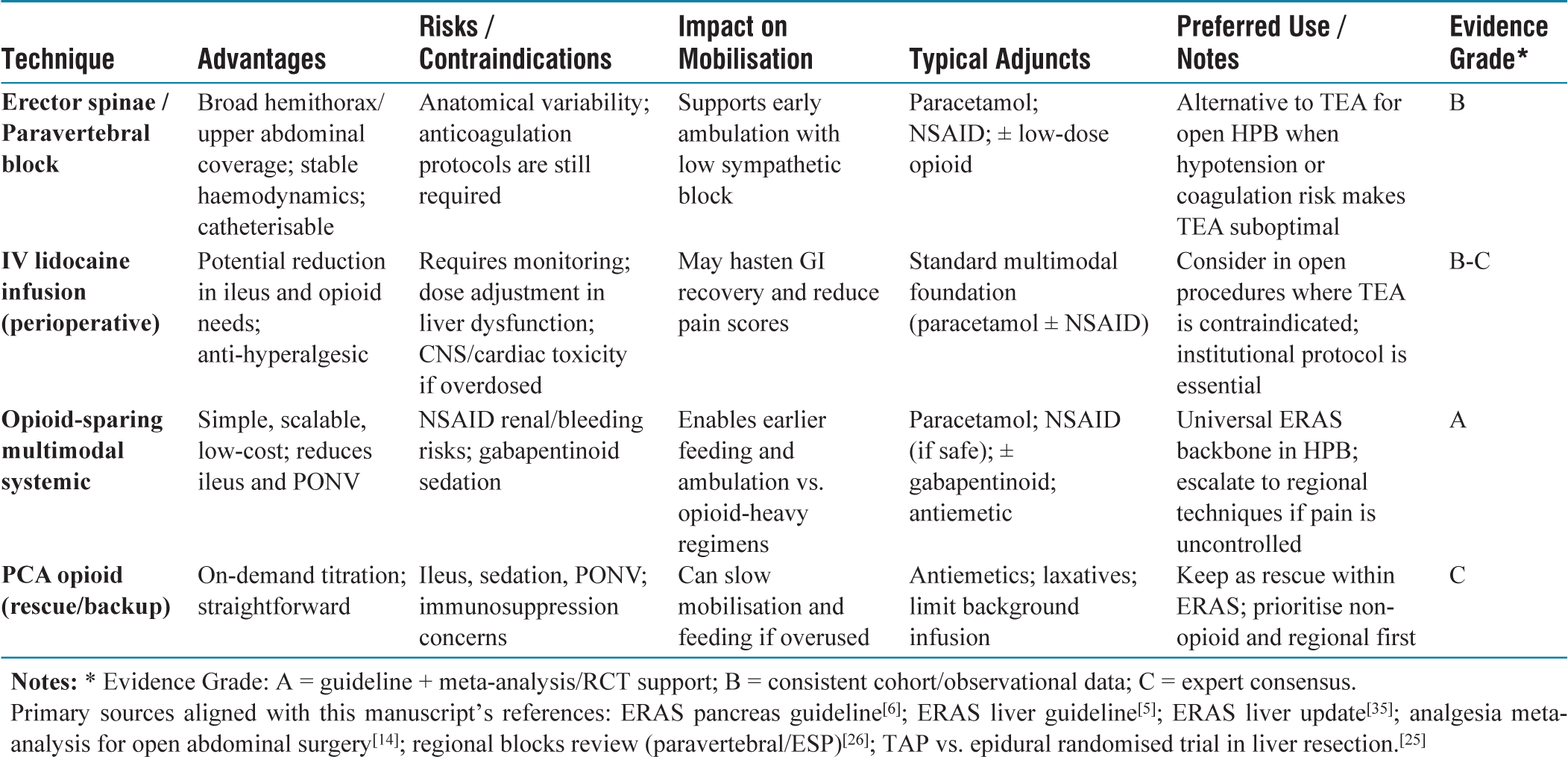
Primary sources aligned with this manuscript’s references: ERAS pancreas guideline[6]; ERAS liver guideline[5]; ERAS liver update[35]; analgesia meta-analysis for open abdominal surgery[14]; regional blocks review (paravertebral/ESP)[26]; TAP vs. epidural randomised trial in liver resection.[25]
Distal Pancreatectomy
Distal pancreatectomy benefits from minimally invasive approaches. Randomised evidence (Laparoscopic vs Open Distal Pancreatectomy trial (LEOPARD) trial) demonstrated that laparoscopic and robotic distal pancreatectomy, combined with ERAS, reduces blood loss, shortens stay by 2–3 days and expedites functional recovery compared with open procedures.[27] Enhanced recovery also minimises opioid use and promotes earlier return to independence.[28]
Compliance and Real-world Implementation
Despite encouraging results, ERAS implementation in pancreatic surgery faces real-world challenges. Compliance rates range from 55% to 75%, with frequent lapses in early feeding, mobilisation and drain removal.[29] Barriers include institutional inertia, entrenched surgical dogma (particularly regarding drains and NG tubes) and anaesthetic preferences for epidural use. Importantly, high compliance correlates directly with improved outcomes, underscoring the need for multidisciplinary teamwork and cultural change.[30]
Criteria-based policies for drains and nasogastric tubes, with audit targets, are summarised in Tables 4 and 5.
Drains and nasogastric (NG) management in HPB ERAS: Indications, removal criteria and outcomes
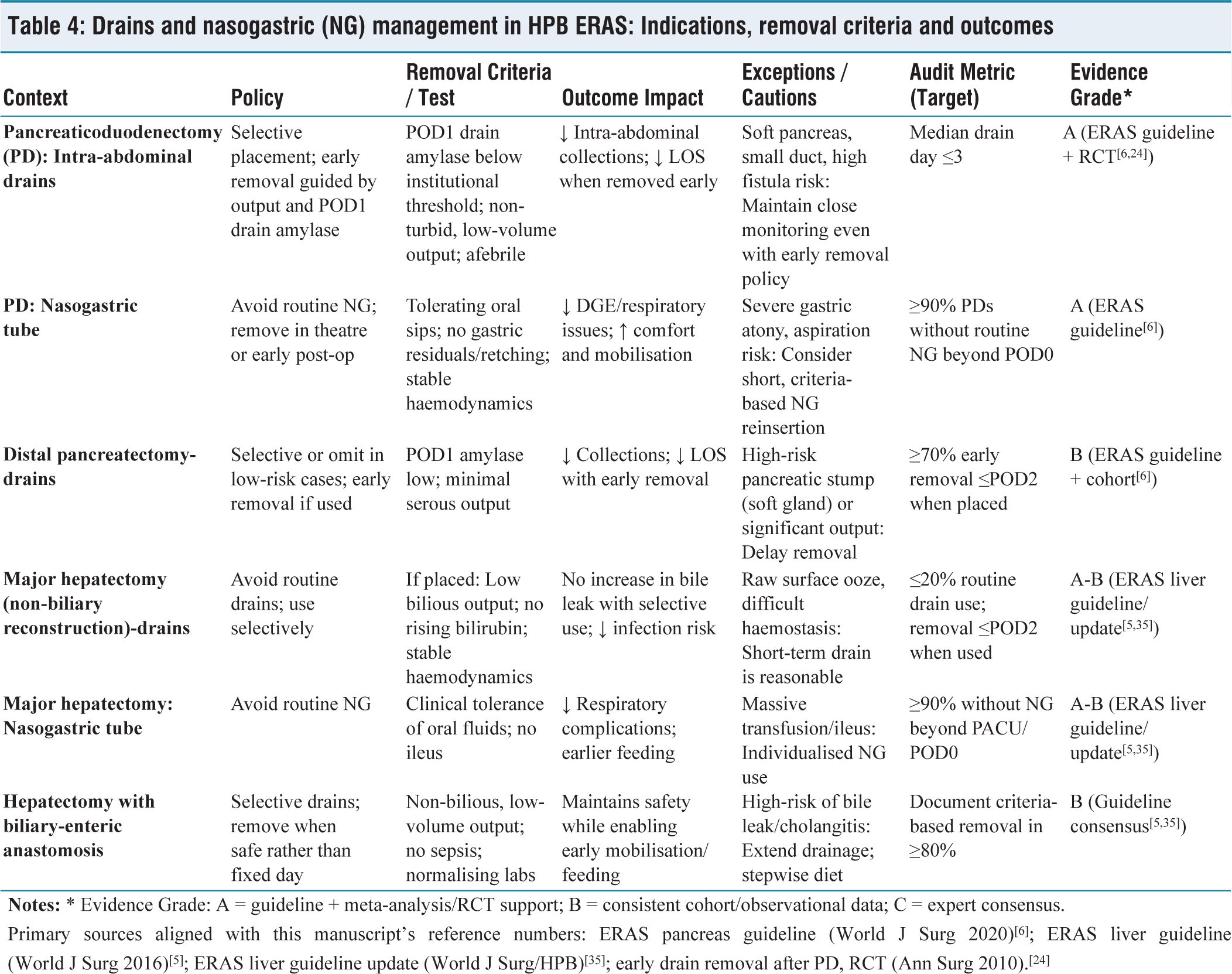
Primary sources aligned with this manuscript’s reference numbers: ERAS pancreas guideline (World J Surg 2020)[6]; ERAS liver guideline (World J Surg 2016)[5]; ERAS liver guideline update (World J Surg/HPB)[35]; early drain removal after PD, RCT (Ann Surg 2010).[24]
Intraoperative fluid strategies in HPB ERAS: GDFT vs. low-CVP, targets and trade-offs
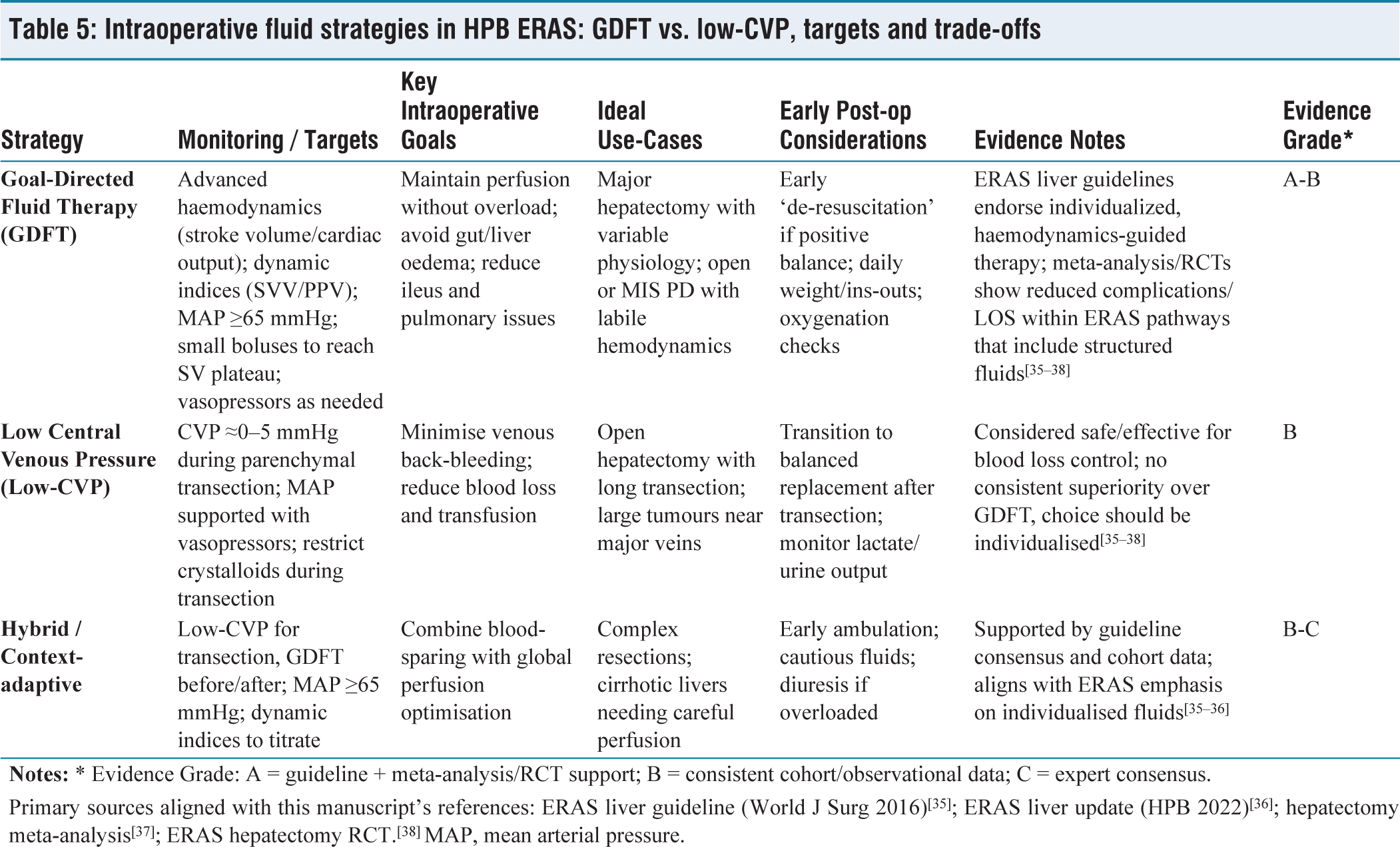
Primary sources aligned with this manuscript’s references: ERAS liver guideline (World J Surg 2016)[35]; ERAS liver update (HPB 2022)[36]; hepatectomy meta-analysis[37]; ERAS hepatectomy RCT.[38] MAP, mean arterial pressure.
Special Considerations in Pancreatic Oncology
ERAS in pancreatic oncology is complicated by frailty, sarcopenia and obstructive jaundice. These patients may not tolerate early feeding or rapid mobilisation as easily as healthier cohorts. Prehabilitation, tailored nutritional support and staged mobilisation strategies may be required to personalise ERAS pathways.[31] Sarcopenia, in particular, predicts postoperative morbidity and delayed adjuvant therapy; thus, targeted interventions in this subgroup are a future priority.
Oncologic Implications
Beyond perioperative metrics, ERAS may influence oncologic outcomes. Reduced morbidity and faster recovery enable earlier initiation of adjuvant chemotherapy, often within the critical 8-week window post-surgery. A multicentre cohort demonstrated significantly higher rates of timely chemotherapy initiation among ERAS-compliant patients.[32] Furthermore, reduced opioid exposure and attenuated stress responses may preserve perioperative immune function, with potential implications for recurrence risk.[33]
Future Directions
Despite robust evidence, heterogeneity persists. Many studies remain single-centre and compliance varies across institutions. Ongoing RCTs are evaluating ERAS protocols in minimally invasive PD, aiming to standardise best practices and clarify oncologic benefits.[34] Integration of digital health tools for compliance monitoring, biomarkers for risk stratification and multicentric collaborations will shape the next generation of pancreatic ERAS protocols.
Summary
In pancreatic surgery, ERAS is safe, feasible and beneficial. It reduces morbidity by nearly 20%, shortens hospital stay by 2–4 days and accelerates recovery without increasing mortality. However, translation from colorectal protocols is not seamless. Pancreatic-specific complications, patient frailty and compliance barriers necessitate adaptation.
Eras in Liver Surgery
Major liver resection represents a formidable physiologic challenge. Substantial blood loss, intravascular volume shifts, coagulopathy and the risk of post-hepatectomy liver failure (PHLF) have historically contributed to morbidity rates exceeding 30% in complex resections. While perioperative mortality is now under 5% in high-volume centres, the focus has shifted toward functional recovery, quality of life and timely resumption of oncologic treatment. ERAS pathways are increasingly employed to meet these aims.
Guidelines and Evidence
The ERAS→ Society released the first perioperative guidelines for liver surgery in 2016, emphasising multimodal care strategies such as preoperative optimisation, opioid-sparing analgesia, restrictive fluid therapy, early mobilisation and selective use of drains.[35] An international update in 2022 expanded recommendations to include minimally invasive hepatectomy, refined transfusion thresholds and newer regional analgesia techniques.[36]
The benefits are supported by high-quality evidence. A 2017 meta-analysis of more than 2,000 patients showed that ERAS reduced overall morbidity by nearly 30% and shortened median length of stay from approximately 10 to 7 days.[37] A randomised trial confirmed that ERAS reduced pulmonary complications, facilitated earlier mobilisation and did not increase PHLF, even after extended resections.[38] A large multicentre cohort study reinforced these findings, showing that hospitals with high compliance achieved the greatest reductions in complications, length of stay and costs.[39]
Key Elements
Fluid management is central to hepatic ERAS. GDFT, guided by cardiac output monitoring, aims to avoid both hypoperfusion and venous congestion. Randomised comparisons with low-CVP techniques suggest both are safe, highlighting the need for individualised strategies.[38]
Analgesia is another cornerstone. While thoracic epidurals provide strong analgesia, they are associated with hypotension and coagulopathy in liver surgery. Alternatives, such as TAP blocks, erector spinae blocks and multimodal systemic regimens, have gained favour, enabling earlier mobilisation without compromising pain control.[36]
Minimally invasive hepatectomy has synergised with ERAS. An international series of more than 9,000 cases demonstrates reduced blood loss, lower narcotic requirements and hospital stay shortened by 3–4 days compared with open resections.[40] Many of these series include both benign and malignant indications, but accumulating oncologic data suggest that outcomes in hepatocellular carcinoma and colorectal liver metastases are not compromised.
Cirrhotic Patients and Oncologic Outcomes
Cirrhosis complicates ERAS implementation. Evidence supports safety in Child-Pugh A patients, but caution is warranted in Child-Pugh B or C patients, where fluid balance and mobilisation must be carefully titrated. Regardless of background liver disease, ERAS has not been shown to compromise oncologic adequacy: microscopically margin-negative resection (R0) resection rates, lymph node yield and survival outcomes are equivalent to conventional care.[39] Importantly, accelerated recovery allows earlier initiation of adjuvant therapy in colorectal liver metastases and hepatocellular carcinoma, potentially improving disease control.
Future Directions
Future refinements include multicentre RCTs evaluating ERAS in minimally invasive hepatectomy, digital compliance monitoring tools and tailored prehabilitation for frail or cirrhotic patients. As these data mature, ERAS is poised to become standard practice, aligning surgical precision with perioperative optimisation in hepatic oncology.
Summary
ERAS in liver surgery is safe, feasible and beneficial. It reduces complications by ~30%, shortens hospital stay by 2–3 days and supports faster recovery without compromising oncologic safety. Individualised care, especially for cirrhotic patients, multidisciplinary adherence and integration with minimally invasive approaches will define the next era of enhanced recovery in hepatic oncology.
Eras in Biliary Surgery/Cholangiocarcinoma
Radical surgery for hilar cholangiocarcinoma and complex biliary malignancies is among the most demanding procedures in HPB oncology. These operations often require extended hepatectomy with biliary reconstruction, performed in patients who are jaundiced, malnourished or cholangitic. The physiological stress of such surgery, combined with the risks of bile leak, cholangitis and PHLF, poses challenges for implementing standardised ERAS pathways.
Evidence and Feasibility
Unlike pancreatic and hepatic surgery, there are no dedicated ERAS Society guidelines for biliary malignancies. Instead, practice has been adapted from liver surgery protocols. Early prospective studies suggest feasibility and benefit. In a Chinese cohort, ERAS shortened the median length of stay from 14 to 11 days and reduced infectious morbidity by nearly 20%, without increasing biliary leak after resection for hilar cholangiocarcinoma.[41] Similarly, a French multicentre study of patients undergoing major hepatectomy with biliary reconstruction reported that ERAS reduced pulmonary complications and enabled earlier resumption of oral intake compared with conventional care.[42] More recently, a single-centre analysis confirmed that ERAS for radical resection of hilar cholangiocarcinoma was safe and associated with fewer postoperative complications and faster functional recovery.[43]
Challenges in Implementation
Preoperative biliary drainage represents a particular dilemma. While ERAS generally discourages unnecessary preoperative interventions, selective drainage is essential in jaundiced patients to reduce cholangitis risk and improve hepatic reserve. Surgeons also remain cautious about early drain removal and aggressive feeding after biliary-enteric reconstruction, fearing bile leaks and septic complications. Nutritional optimisation and immunonutrition are crucial, as sarcopenia and protein-calorie malnutrition are strong predictors of adverse outcomes.[44]
Future Directions
The current evidence base is limited, largely derived from Asian and European single-centre series. Broader validation in multicentre and Western cohorts is urgently needed to establish generalisability. Until then, ERAS in cholangiocarcinoma should be viewed as a flexible framework, where core principles, early mobilisation, multimodal analgesia and restrictive fluid therapy are preserved, but elements such as drainage, nutrition and timing of oral intake are carefully individualised.
Comparative Analysis: Does Eras Translate Seamlessly?
The origins of ERAS lie in colorectal surgery, where standardised multimodal protocols consistently demonstrated reductions in morbidity, length of stay and costs.[45] In high-volume colorectal centres, adherence rates frequently exceed 80%–90% and outcomes are now predictable and reproducible worldwide. This maturity naturally prompted attempts to extend ERAS principles to HPB oncology.
Yet translation has proven less straightforward. PD carries risks of DGE, pancreatic fistula and nutritional compromise, while major hepatectomy entails blood loss, coagulopathy and PHLF. Although meta-analyses confirm that ERAS reduces morbidity and shortens hospital stay by 2–4 days in both pancreatic and hepatic resections, the magnitude of benefit is more variable than in colorectal cohorts.[46] Equally important, compliance rates in HPB ERAS are consistently lower, typically around 60%–70% with early feeding, drain management and fluid restriction being the most common areas of hesitation.[47]
Patient profile also differs. Unlike many colorectal patients, those with HPB malignancies often present with obstructive jaundice, cholangitis, sarcopenia or chemotherapy-induced frailty, which complicates the straightforward application of standardised bundles. These comorbidities highlight that while the principles of ERAS, attenuation of surgical stress, early mobilisation, nutritional optimisation and multimodal analgesia are universal, the execution requires thoughtful, speciality-specific adaptation.
Encouragingly, ERAS has not been shown to compromise oncologic outcomes. Studies demonstrate equivalent R0 resection rates, nodal yield and long-term survival compared with conventional care. More importantly, ERAS facilitates earlier initiation of adjuvant chemotherapy, often within the critical 6–8 weeks window after pancreatic or hepatic resections, a factor directly linked to improved survival.[48]
A quantitative summary of effect sizes for pancreatic and liver resections under ERAS versus conventional care is presented in Table 6.
Summary of effect sizes with ERAS vs. conventional care (pancreatic vs. liver resections)
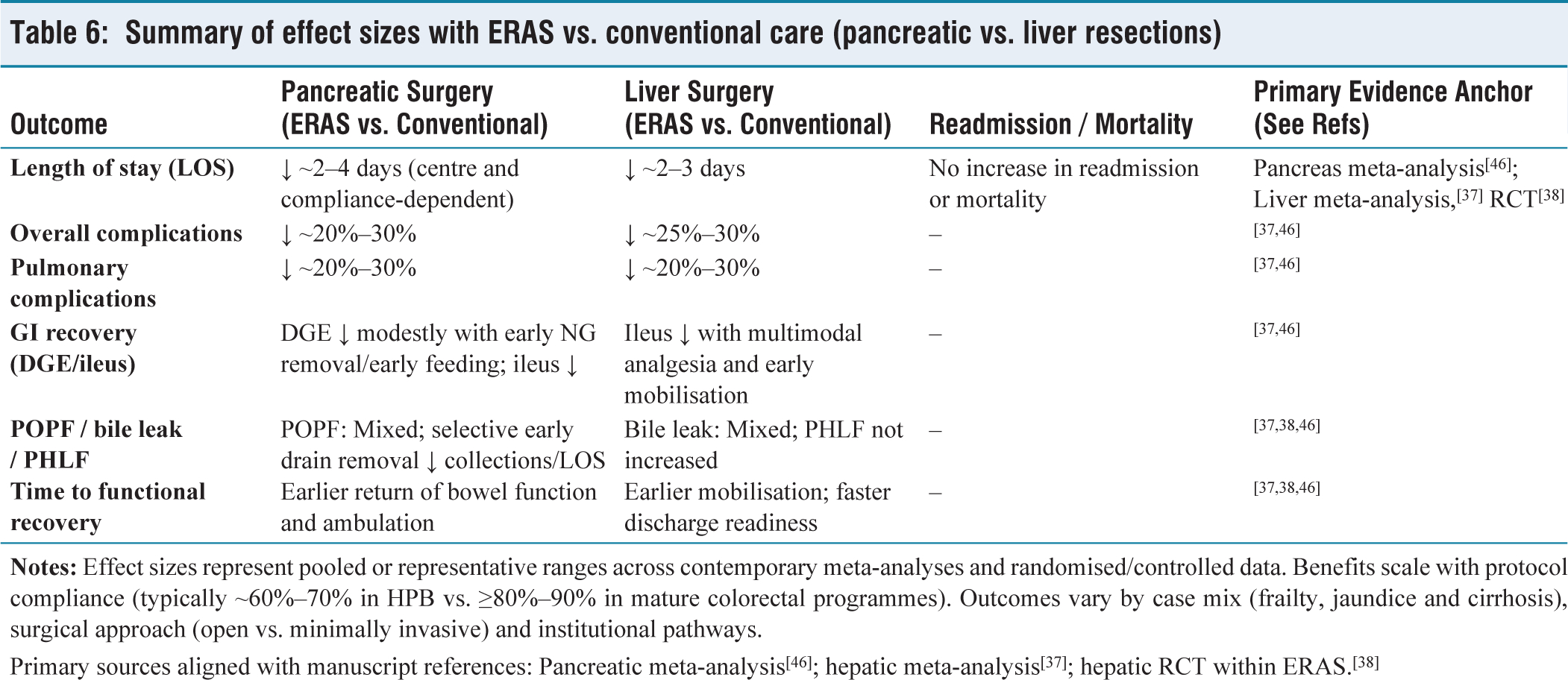
Primary sources aligned with manuscript references: Pancreatic meta-analysis[46]; hepatic meta-analysis[37]; hepatic RCT within ERAS.[38]
Future Directions and Conclusion
Although the evidence base for ERAS in HPB oncology has grown rapidly, its maturity lags behind colorectal surgery. To fully realise its potential, ERAS in HPB surgery must evolve across several key domains.
Future Directions
ERAS should move beyond a uniform pathway toward individualised recovery programmes. Incorporating biomarkers of frailty, sarcopenia and hepatic reserve will allow tailored interventions. Prehabilitation, encompassing exercise, nutrition and psychological support, has shown measurable benefits. In a randomised trial, prehabilitation improved preoperative 6-minute walk distance by 36 m and reduced postoperative complications in high-risk abdominal surgery patients.[49] Such strategies are especially pertinent in frail, jaundiced or chemotherapy-exposed HPB patients.
Compliance remains the strongest predictor of ERAS success, yet real-world adherence averages only 60%–70% in HPB surgery. Mobile health applications and wearable devices are being piloted to track step counts, nutritional intake and analgesic use, providing real-time feedback to patients and clinicians. Early trials suggest these tools improve compliance rates by nearly 15%.[50]
Combining ERAS with laparoscopic or robotic surgery offers synergistic benefits. In the ORANGE II trial, laparoscopic hepatectomy within ERAS shortened hospital stay by 3 days compared with open resection.[51] Ongoing RCTs are evaluating whether minimally invasive PD in an ERAS framework can deliver similar benefits.
Most high-quality ERAS studies come from Asia and Europe. For low- and middle-income countries, simplified, low-cost ERAS bundles, such as reduced preoperative fasting, early mobilisation and multimodal analgesia, can deliver meaningful improvements even in resource-constrained settings.[52] Capacity-building and international collaborations will be critical to ensuring ERAS is accessible globally.
Future trials must extend beyond perioperative outcomes to include recurrence, disease-free survival and chemotherapy delivery. A systematic review suggests that ERAS patients are 20%–30% more likely to initiate adjuvant therapy within the optimal 8-week window, a factor directly linked to survival.[53] Establishing these long-term benefits would position ERAS as an oncologic, not just perioperative, strategy.
Conclusion
ERAS has transformed perioperative care in colorectal surgery and is now steadily reshaping HPB oncology. Evidence supports its ability to reduce morbidity, shorten length of stay by 2–4 days and improve functional recovery without compromising oncologic outcomes. However, translation is not seamless; protocols require tailoring to the unique physiologic challenges of pancreatic and hepatic resections and to the comorbidities of oncology patients. Looking ahead, precision-based ERAS, digital compliance tools, minimally invasive synergy and global equity will define the next era. With these refinements, ERAS is poised to become not just a perioperative adjunct but a new standard of care in HPB oncology, aligning surgical excellence with oncologic integrity.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable (narrative review).
Informed Consent
Not applicable. This manuscript is a narrative review and does not involve human participants or identifiable patient data.
Credit author statement
Data availability
No new data were generated or analysed in this study. Data sharing is not applicable.
Use of artificial intelligence
Artificial intelligence tools (ChatGPT, OpenAI, San Francisco, CA, USA) were used to assist in language refinement and formatting under the direct supervision of the corresponding author. The intellectual content, data interpretation, and final conclusions are entirely those of the authors.
Guarantor
Dr Supreet Kumar accepts full responsibility for the integrity and accuracy of the content.