
Abstract
Background:
Due to an outbreak of conjunctivitis in Uttarakhand, a large number of cases are being reported to hospitals for management. It was important to document it to learn about its characteristics. Through this study, we put forth the distribution and clinical features of the cases managed at a tertiary care hospital in Dehradun, contributing to the widespread event beyond the state of Uttarakhand.
Material and Method:
All cases were isolated from other patients and studied. Proper history, clinical features were recorded, managed with the optimum treatment and monitored for the requisite duration to learn the course and resolution. Data was analysed using the Statistical Package for Social Sciences, Chi-square and Fisher test. A P value less than .05 was considered significant.
Results:
The total number of new patients attending the eye out patient department (OPD) from 1st July to 31st October was 3,381. Out of these 172 patients (5.08%), some presented in one or both eyes. A 5.13% increase was observed in July and August, compared to 0.80% cases and the difference in decline was found to be statistically significant (P value = .0001). The most significant age group affected was between 20 and 30 years of age. Most common clinical features of presentation were attributed to swelling of the eyes, redness and mucopurulent discharge, found to be statistically significant (P < .0001).
Conclusion:
In our study, clinical features are considered to be non-specific for diagnosis, rapid onset and remission with antibiotic therapy could be suggestive of bacterial or even a mixed event of both viral and bacterial aetiology.
Introduction
Conjunctivitis, also known as ‘eye flue’ in layman’s language, is a contagious entity. It is a common cause of ‘red eye’, due to which patients seek consultation, yet outbreaks of conjunctivitis are not typically reported.[1,2] Conjunctivitis could be broadly attributed to allergic or infectious causes. Among infectious aetiologies, viral and bacterial forms are the most common presentations. Studies have reported that adenoviral conjunctivitis contributes to 80% of all acute conjunctivitis cases, while bacterial aetiology accounts for around 50%-75% of cases of infectious conjunctivitis, especially in children.[3] Bacterial conjunctivitis usually presents with redness, mucopurulent/purulent discharge, swelling of the lids and foreign-body sensation. The typical feature is that the onset, involvement of the other eye and resolution are faster in bacterial than in viral conjunctivitis. Matting and adherence of the sticky eyelids on waking up from sleep, lack of itching and absence of a history of conjunctivitis are the strongest factors associated with bacterial conjunctivitis. Viral conjunctivitis is known to present with lid oedema, follicles, subconjunctival haemorrhages, petechial haemorrhages, preauricular lymphadenopathy, lacrimal gland enlargement, nasolacrimal duct inflammation, multifocal punctate keratitis and subepithelial infiltrates.[4-6] Involvement of the cornea causes diminution of vision, which could be a presenting feature of viral keratoconjunctivitis. Cultures for routine conjunctivitis are rarely helpful in deciding on the treatment course or cost-effective. They may be helpful for recurrent, severe or chronic purulent conjunctivitis in any age group and in cases where the conjunctivitis has not responded to medication.[5,7,8] The bacterial conjunctivitis, although self-limiting in benign conditions, relies more on topical antibacterial for faster recovery.[9] Clinical management of adenoviral conjunctivitis is considered to be symptomatic and palliative. Steroids relieve symptoms, but they also contribute to recurrence. Povidone-iodine has broad-spectrum antimicrobial properties to inhibit various bacteria, viruses, fungi and other organisms.[10–12] Through this study, we look into the clinical features of conjunctivitis that presented as an outbreak in Uttarakhand and try to throw some light on its magnitude in a tertiary care centre of Dehradun.
Material and Method
This is a cross-sectional, observational hospital-based study, conducted from July to September in a tertiary care hospital of Dehradun. A sudden increase in the number of cases of conjunctivitis daily, both from within and outside the hospital premises, emphasised the need for a discrete documentation. All patients with red eye or symptomatically suggestive of conjunctivitis were assessed in a separate, isolated room. A thorough history was taken regarding any viral systemic illness, redness, discharge, swelling of lids, itching and diminution of vision. General examination was done to especially look for any preauricular lymphadenopathy and vision of both eyes was documented on Snellen’s Chart.
A torch light and slit lamp examination was performed to assess the anterior segment, particularly the cornea and the pupil. Fluorescein staining was used to detect viral infection of the cornea, where needed. Empirical treatment in the form of an antibiotic drop (frequency depending on the severity) and ointment at night was prescribed and the patient was asked to review either after three days or if symptoms worsened patient was counselled regarding hygienic practices and distancing. Other aetiological factors for a ‘red eye’, including allergic conjunctivitis, were excluded from the study.
Outbreak Investigation
The clinical features suggestive of bacterial infection were a red eye with severe congestion, lid oedema and mucopurulent or purulent thick discharge. Bacterial conjunctivitis was diagnosed with a sudden onset, rapid involvement of the other eye and a faster resolution with a prompt response to medications. The diagnosis of adenoviral conjunctivitis was made when patients presented with excessive watering, chemosis, petechial or subconjunctival haemorrhages, involvement of the cornea and lymphadenopathy. The involvement of the other eye took more than 48 hours and a longer duration of resolution.[4–6] A questionnaire was prepared to collect the findings and events of the patient and was analysed.
Outbreak Management
Besides the adequate methods for the management of patients with conjunctivitis, which included isolation of the patient, provision of a protective kit for hospital personnel and guarding the safety of other patients, thorough awareness was created in the hospital and community. Healthy and hygienic practices were emphasised through digital media and print. All patients were counselled and the cooperation of staff was sought to prevent nosocomial infection.
Statistical Analysis
The presentation of the categorical variables was done in the form of numbers and percentages (%). On the other hand, the quantitative data with normal distribution were presented as the means ± SD. The data normality was checked by using the Shapiro-Wilk test. The comparison of the variables, which were quantitative and normally distributed in nature, was analysed using an independent t-test. The comparison of the variables, which were qualitative in nature, was analysed using the Chi-square test. If any cell had an expected value of less than five, then Fisher’s exact test was used. The data entry was done in the Microsoft Excel spreadsheet and the final analysis was done with the use of Statistical Package for Social Sciences software, IBM manufacturer, Chicago, USA, version 25.0.
Results
The total number of new patients attending the eye out patient department (OPD) from 1 July to 31 October was 3,381. Out of these 172 (5.08%) patients presented with conjunctivitis in one or both eyes. Maximum patients presented with conjunctivitis in July and August, where the new patients seen in OPD were 1,833, out of which 150 (5.13%), in comparison to 20 (0.80%) cases of conjunctivitis in September and October, when 1,548 new patients presented to the eye OPD. The difference in the % of cases of conjunctivitis was found to be statistically significant (P value = .0001).
Out of 172 cases of conjunctivitis, 150 were patients from outside the Department of Ophthalmology, hence were named as the ‘external’ candidates, while 22 patients were serving the department, hence were termed as the ‘internal’ candidates. The most common age group affected among both the internal and external groups was between 20 and 30 years of age (P value < .0001).
Most common clinical features of presentation were attributed to swelling of eyes, redness and mucopurulent discharge and swelling of eyes as 100% external cases presented with these symptoms and this was found to be statistically significant when compared to other clinical features (P value < .0001). No patient had diminished vision at presentation.
In the present study, although 47.60% health personnel in the eye department were not affected, bilateral involvement of eyes at presentation was seen in 100% (n = 22) was noted in all internal cases. Out of 150 external cases, 80.67% (121) showed bilateral involvement at presentation. Thus, bilaterality was significantly common with a P value less than .0001.
Comparison of new cases between July and August and between September and October

Comparison of conjunctivitis between July and August versus September and October
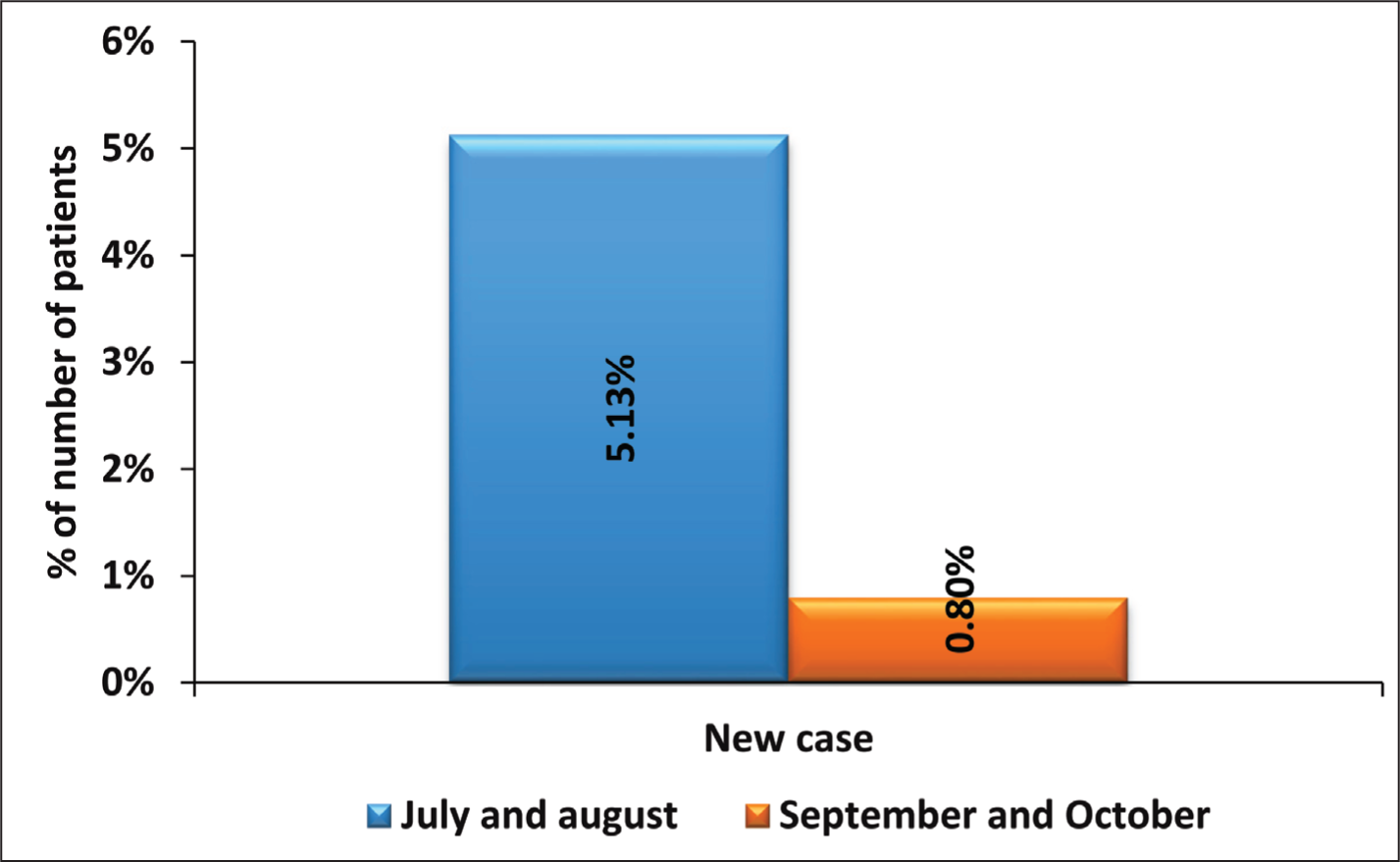
The total number of new patients attending the eye OPD from 1st July to 31st October were 3381. Out of these 172 (5.08%) patients presented with conjunctivitis in one or both eyes. Maximum patients presented with conjunctivitis in the months of July and August, where the new patients seen in opd were 1833 out of which 152 (5.13%), in comparison to 20 (0.80%) cases of conjunctivitis in the months of September and October when 1548 new patients presented to the eye opd. The difference in the percentages of cases of conjunctivitis was found to be statistically significant (P value = 0.0001).
Distribution of age between internal and external data
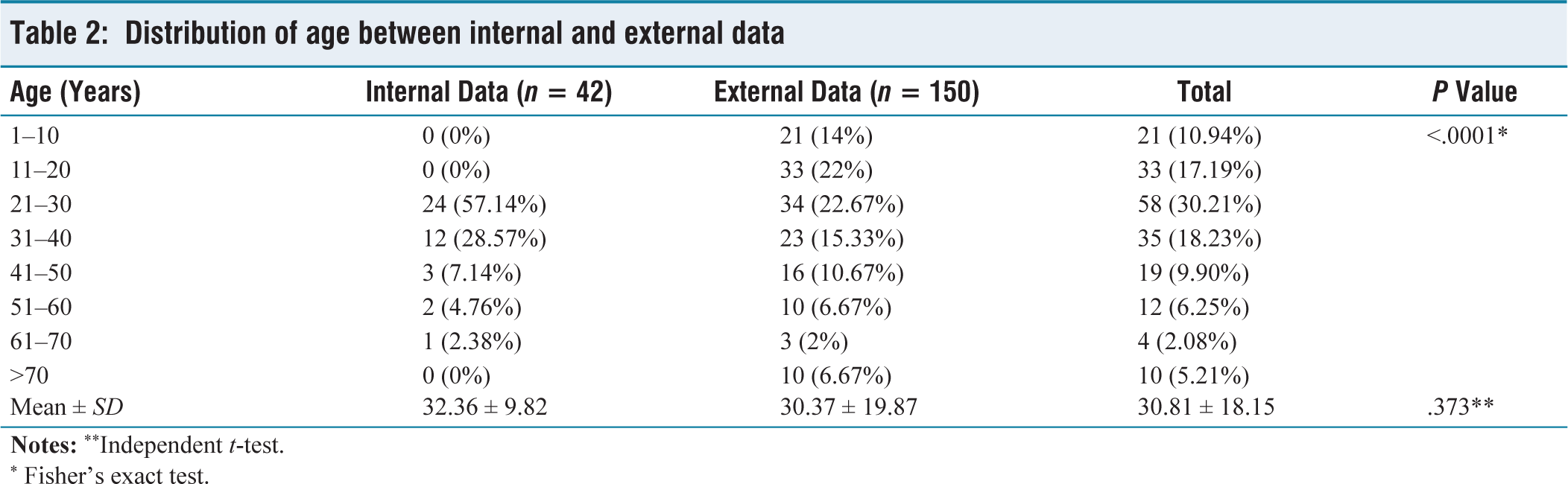
* Fisher’s exact test.
Age distribution in patients with conjunctivitis
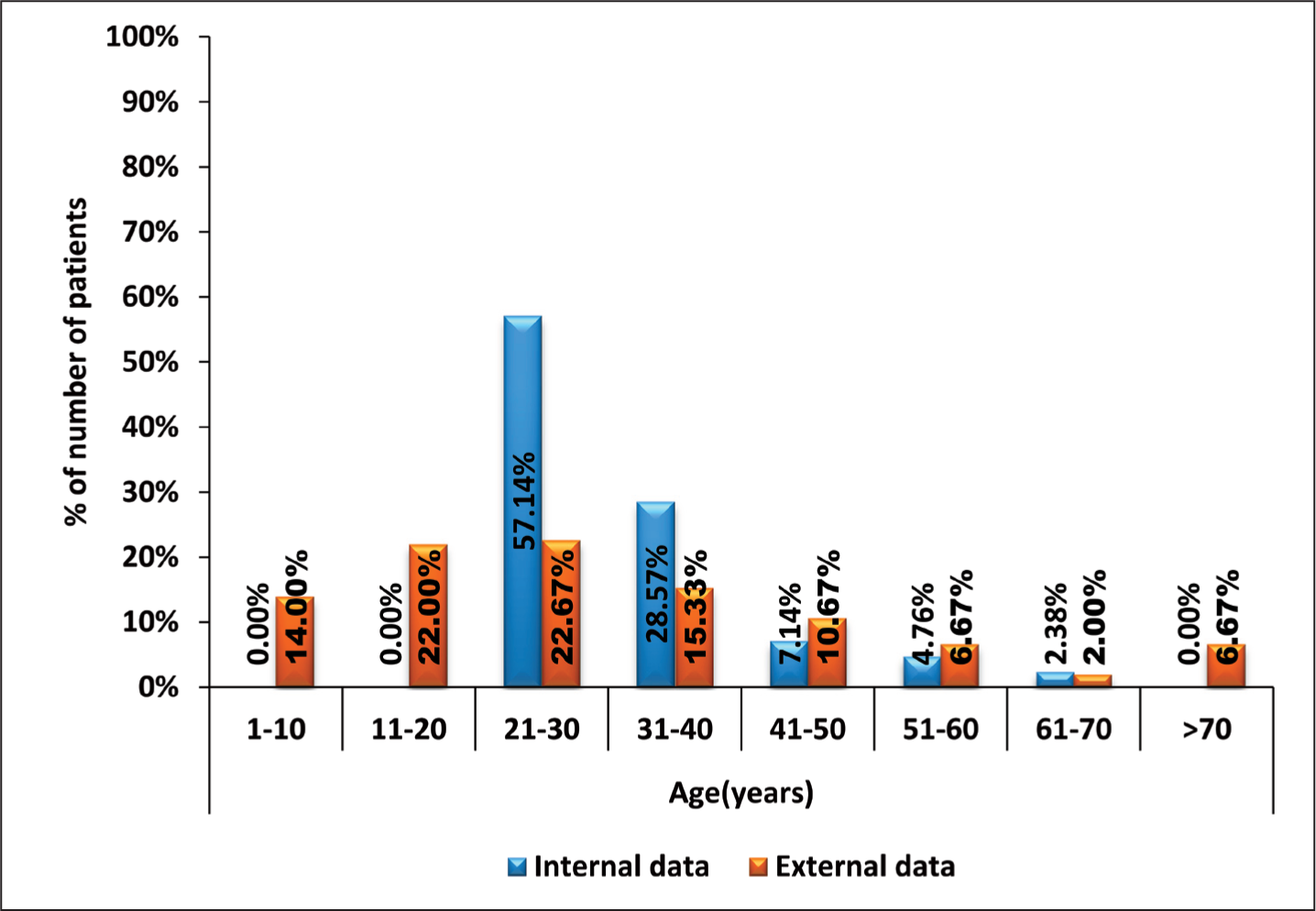
Out of 172 cases of conjunctivitis, 150 were patients from outside the department of Ophthalmology hence were named as the “external” candidates, while 22 patients were serving the department hence were termed as the “internal' candidates. The most common age group of affected among both the internal and external group was between 20 and 30 years of age (P value < .0001).
Distribution of clinical features between internal and external data
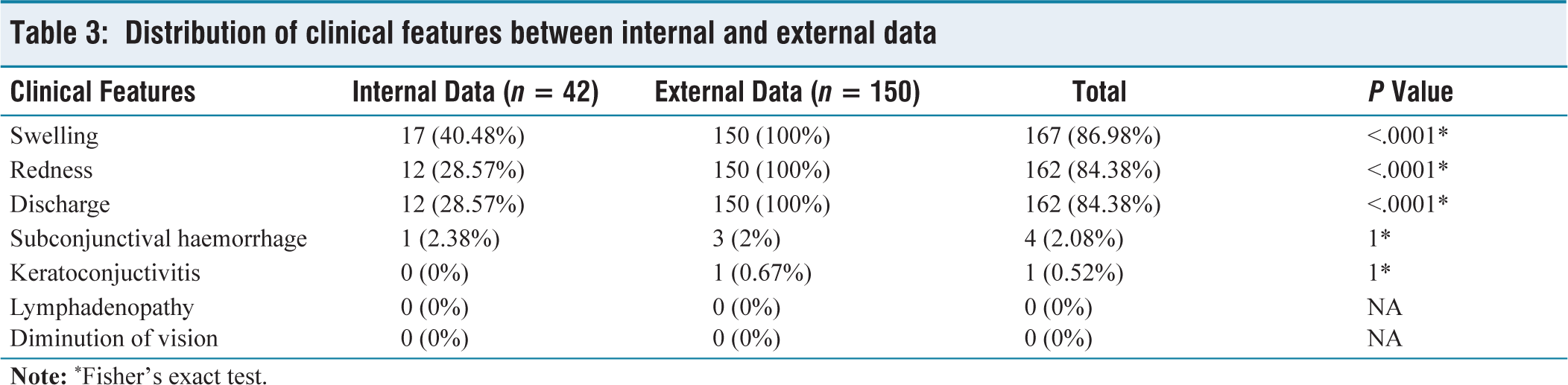
Distribution of clinical features
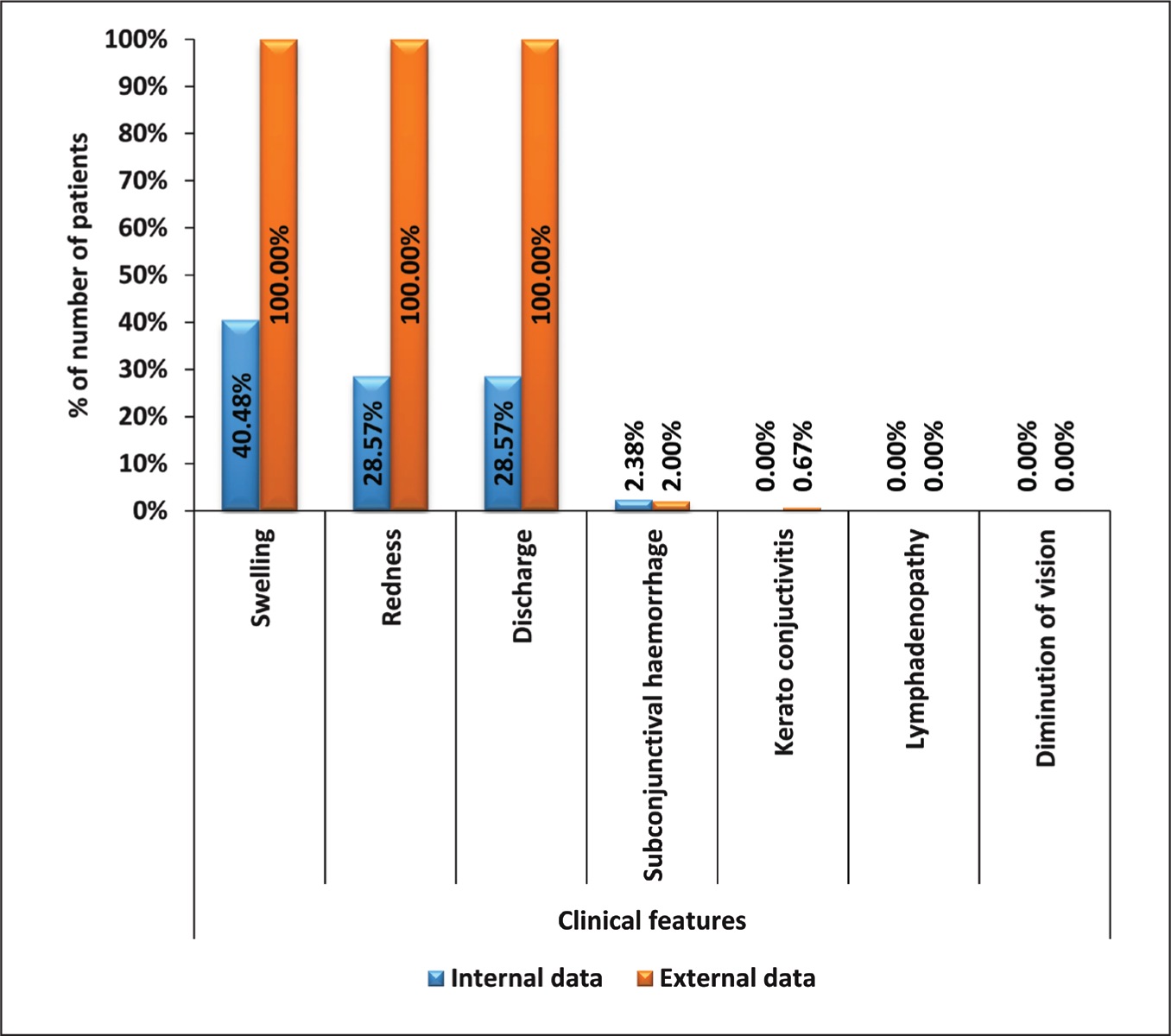
Most common clinical features of presentation were attributed to swelling of eyes, redness, mucopurulent discharge, and swelling of eyes as 100% external cases presented with these symptoms and this was found to be statistically significant when compared to other clinical features (P value <.0001). No patient had diminution of vision at presentation.
Distribution of cases according to the laterality of eyes
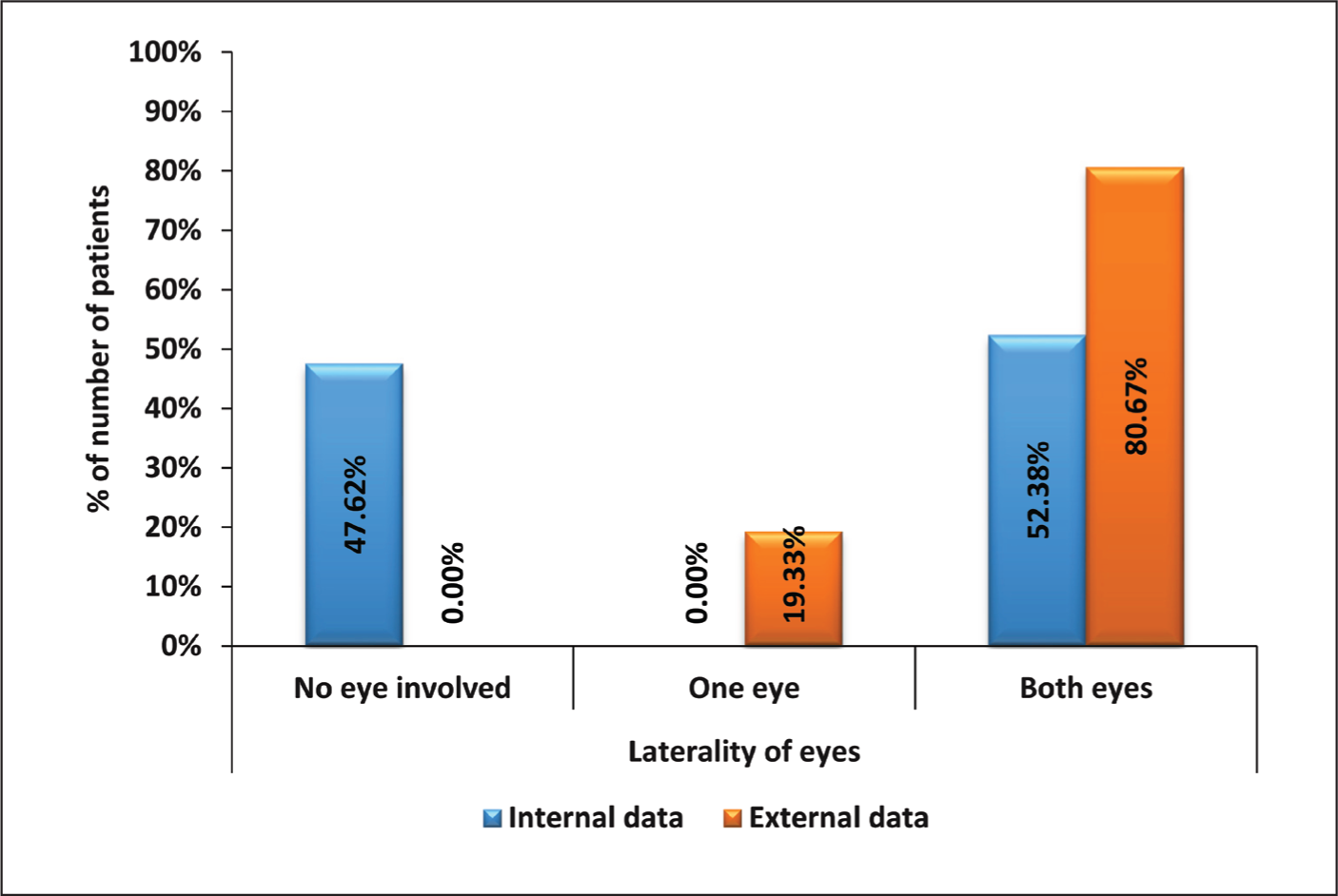
Distribution of cases according to laterality of eyes
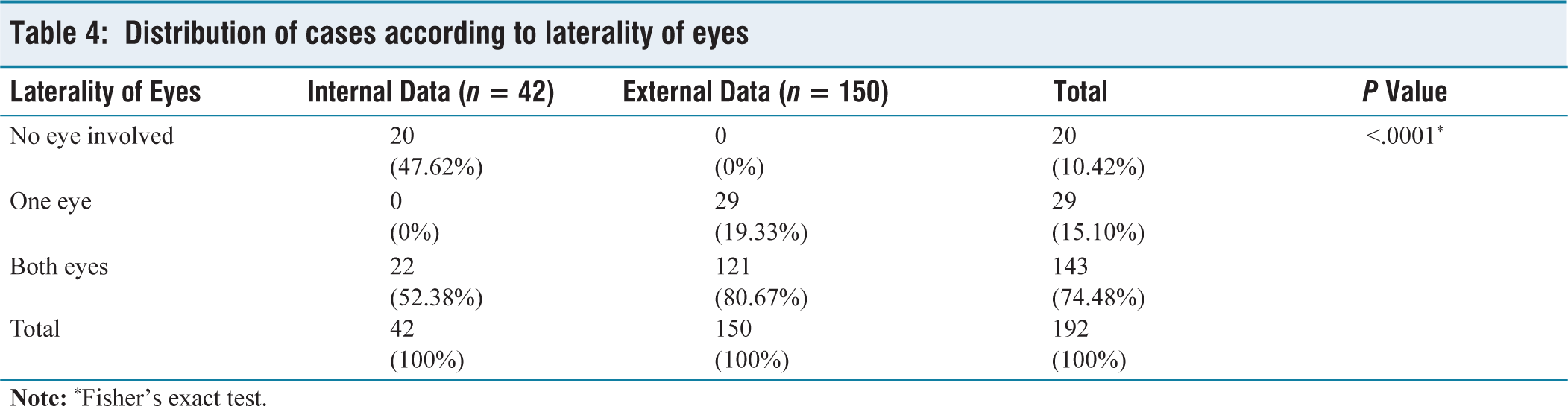
In the present study, although 47.60% health personnels in the eye department did not affected, bilateral involvement of eyes at presentation was seen in 100% (n = 22) was noted in all internal cases. Out of 150 external cases, 80.67% (121) showed bilateral involvement at presentation. Thus bilaterality was significantly common with P value less than 0.0001.
Discussion
Conjunctivitis, as an outbreak affecting a large number of people in a given time period, is a more alarming situation than random and individual cases. The present study reports on an epidemic that was noted in the city of Dehradun, peaking during July and August and declining thereafter, with no cases by the end of October 2023. In our study, out of 3,381 patients diagnosed for various ophthalmological entities, 172 (5.08%) had conjunctivitis. This data also showed a pattern of increase in number during July and August and then a severe fall in September and finishing by the end of October. Reports claim that the pathogen in such outbreaks and epidemics is not typically identified and adenoviral aetiology is commonly assumed.[13] They also found a significant seasonal variation in the northern and southern hemispheres, with countries from the southern hemisphere reporting a greater incidence of outbreaks in late summer to early fall.[13] In our study, the common age group was that of adolescents and young adults, after excluding allergic conjunctivitis right at the outset of the study, as allergic conjunctivitis is chronic, seasonal and needs a long-term follow-up of the cohort.
The significant clinical features in our study were swollen eyes and lids, redness and mucopurulent discharge. Out of 172 cases, 143 (83.13%) showed bilateral involvement of the eyes simultaneously or within 24 hours of infection of one eye. Those 29 (16.87%) patients with unilateral presentation also manifested with the infection of the second eye within 48 hours of conjunctivitis of one eye. Such features of symptoms and signs could suggest a bacterial aetiology. However, due to a lack of uniformity in data for sample collection, a generalised assessment of the pathogen could not be made. In a recent study from Bangladesh, Mokbul et al. diagnosed the viral aetiology based on the images of conjunctivitis and their clinical features and superimposed timing of COVID-19. They also emphasised empirical treatment, proper mass education and awareness.[14]
In our study, the age group most affected was 20 to 40 years. As we have excluded allergic conjunctivitis, infective conjunctivitis reported among children and higher age groups was considerably less. Even among internal candidates, the residents got infected rapidly as compared to senior staff or consultants. Apart from other reasons of hygiene and cleanliness, the higher intermingling and social interaction of people in the above age group might add to the possibility of such an outbreak in a specific age group. However, more data from other health centres is required to draw an inference.
Limitation: Our study shows documented data from one health centre in Dehradun. More information and statistics from other health facilities could add a perspective to the picture of conjunctivitis. Also, being a medical institution, many hospital personnel took empirical treatment themselves and were not available for documentation.
Conclusion
The striking feature of this outbreak of conjunctivitis in our area was a rapid start, speedy resolution, mucopurulent discharge without corneal involvement and diminution of vision. The response to empirical antimicrobial therapy was quick, with full recovery in less than seven days. This is not to affirm a certain bacterial aetiology, but to present statistics documented in our institution for a better outlook. Such studies help to contribute to the global understanding of the epidemic of conjunctivitis and its pattern.
Footnotes
Credit author statement
VV was involved in Concepts, Design, Definition of intellectual content, literature search, conduct of cases, data acquisition, data analyses, manuscript preparation, editing, review and approval.
TS was involved in Concepts, Design, Definition of intellectual content, literature search, conduct of cases, data acquisition, data analyses, manuscript preparation, editing, review and approval.
AK was involved in Concepts, Design, Definition of intellectual content, literature search, conduct of cases, data acquisition, data analyses, manuscript preparation, editing, review and approval.
DR was involved in Concepts, Design, Definition of intellectual content, literature search, conduct of cases, data acquisition, data analyses, manuscript preparation, editing, review and approval.
SM was involved in Concepts, Design, Definition of intellectual content, literature search, conduct of cases, data acquisition, data analyses, manuscript preparation.
Data availability
De-identified data may be requested with reasonable justification from the authors (email to the corresponding author) and shall be shared after approval as per the authors' institution's policy.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
SGRR/IEC/97/23.
Use of artificial intelligence
None.