
Abstract
Background:
Musculoskeletal (MSK) conditions account for a substantial proportion of general practice consultations, with low back pain (LBP), knee pain and shoulder pain is the most common. High representation rates emphasise the need for efficient management pathways, including the appropriate use of imaging and referral. First contact physiotherapists (FCPs) have improved patient access to self-management strategies; however, GPs continue to generate the majority of imaging requests.
Methods:
MSK imaging guidelines for LBP, as recommended by the National Institute for Health and Care Excellence was reviewed. A retrospective 3-month review of LBP presentations was also undertaken in our GP practice, identifying patients coded with ‘LBP’, ‘backache’, ‘chronic LBP’ or ‘lumbago with sciatica’.
Results:
A total of 299 consultations were recorded (131 male, 168 females; mean age, 63 years). Most patients (66.7%) were initially assessed by a GP, compared with 9% by an FCP, 18% by an advanced nurse practitioner and 6% by an emergency care practitioner. Imaging was requested in 42% of cases: 30% magnetic resonance imaging (MRI) and 12% X-ray. Findings included degenerative disease, suspected discitis, osteoporotic fractures and spondylosis. Referrals to spinal surgery were rare; most patients were managed conservatively with advice, analgesia and physiotherapy. MRI turnaround was 4–5 weeks for routine requests and 8 days for urgent cases.
Conclusion:
Structured pathways and increased FCP involvement improve the appropriateness of imaging requests and support patient self-management. MRI should be reserved for patients with neurological deficits or suspected serious pathology. Expanding direct physiotherapy access can optimise care and reduce GP workload.
Introduction
Musculoskeletal (MSK) conditions comprise a significant proportion of general practitioner (GP) consultations. The article ‘The prevalence of MSK presentations in general practice: An epidemiological study’ recorded a 21.1% prevalence in the average GP practice.[1] The most common presentations were low back pain (LBP) (18.3%), knee pain (17.4%) and shoulder pain (2.4%). Representations of an existing condition accounted for 73.9% of all MSK consultations. This is an important finding, as ideally GPs would prefer to signpost patients to the most appropriate services at or even before, the first point of contact, avoiding unnecessary delays in accessing the right treatment. Representations also add pressure to the already limited number of GP appointments, meaning that streamlining the process could improve both the patient journey and healthcare efficiency.
The introduction of first contact physiotherapists (FCPs) in most GP practices has reduced the number of first presentations to GPs for MSK conditions by providing direct access to physiotherapy. A 2021 study evaluating the FCP model in primary care concluded that GPs expressed confidence in both the service and the competence of FCPs.[2] Patients reported increased self-efficacy, confidence in self-management techniques and generally described the FCP service as a positive experience. Importantly, the study noted that ‘most patients were managed using a tailored self-management strategy within two appointments’.[2]
Imaging requests, however, are more likely to come from GPs than from trained FCPs. This suggests that additional training in MSK conditions may help reduce unnecessary requests for investigation. Most GPs do not undergo specific orthopaedic training during their 3-year GP training course; instead, their knowledge is typically derived from medical school, Accident & Emergency (A&E) placements, experience in practice and training sessions. Some GPs develop joint injection skills, which represent a valuable treatment modality in primary care and help reduce referrals to hospital specialists.
Several articles have reviewed variations in the management of MSK conditions in primary care and explored opportunities for improvement. For example, a 2018 British Medical Journal (BMJ) mixed-methods study described the development of clinical pathways for MSK conditions, which were disseminated to practices and made available online.[3]
MSK Imaging Protocol
In my local area of practice, the Dudley Group National Health Service (NHS) Foundation Trust has implemented a new primary care MSK imaging protocol to streamline imaging pathways and align services with the British Orthopaedic Association guidance. The aim was to improve patient outcomes by ensuring the appropriate assessment and management of clinical problems, rather than relying too heavily on MSK imaging.
One example was the British Elbow and Shoulder Society pathway for the diagnosis, treatment and referral of shoulder pain.[4] Its introduction reduced unnecessary imaging for shoulder presentations. Initially, several GP imaging requests were rejected, compelling GPs to review and follow the guidelines. According to this pathway, in the absence of red flags, initial treatment for shoulder pain typically involves physiotherapy or injection therapy, with imaging considered only if symptoms persist for more than 4 months.[4]
Notably, GPs observed that once the imaging threshold was reached, magnetic resonance imaging (MRI) was considered the gold standard compared to ultrasound for shoulder conditions. Interestingly, the primary imaging modality differs internationally depending on resources, economics and healthcare systems. For example, the United States often favours MRI, while Canada typically advocates ultrasound as the first-line choice.[5]
MRI Referrals from Primary Care
Several NHS guidelines outline the criteria for MRI referrals for back pain.[6] Lumbar spine radiographs have limited diagnostic value when requested for back or radicular pain. X-rays should only be considered in cases of focal, refractory back pain and concern about an osteoporotic vertebral fracture.[6]
Patients with acute back pain (≤6 weeks) should undergo urgent MRI if any of the following are present[6,7]:
Focal neurological deficit localised to a spinal nerve root or cord level. Focal, refractory pain with concern for osteoporotic fracture Previous, current or suspected malignancy Immunosuppression Long-term steroid use Clinical suspicion of discitis
Patients with back pain lasting more than 6 weeks and associated neurological findings may also be considered for an MRI.[7,8] In contrast, MRI is not indicated for acute or chronic back pain without radicular symptoms, red flags or adverse features; for sciatica of less than 6 weeks’ duration; or for chronic back pain without progressive features.[9,10]
Results
I conducted a review of LBP presentations in my practice over 3 months (14/05/25–14/08/25). The search included patients coded as ‘LBP’, ‘backache’, ‘chronic LBP’ and ‘lumbago with sciatica’. A total of 299 consultations were recorded [Table 1]: 131 male and 168 female. The mean patient age was 63 years (range, 41–85). Some presentations were initially coded as ‘LBP’ but were later identified as renal in origin (infection or stone). Duplication of care occurred in some cases, for example, when GPs inappropriately referred patients to FCPs instead of community physiotherapy or when patients booked GP appointments while waiting for an FCP consultation.
Patient characteristics and imaging requests (3-month review)
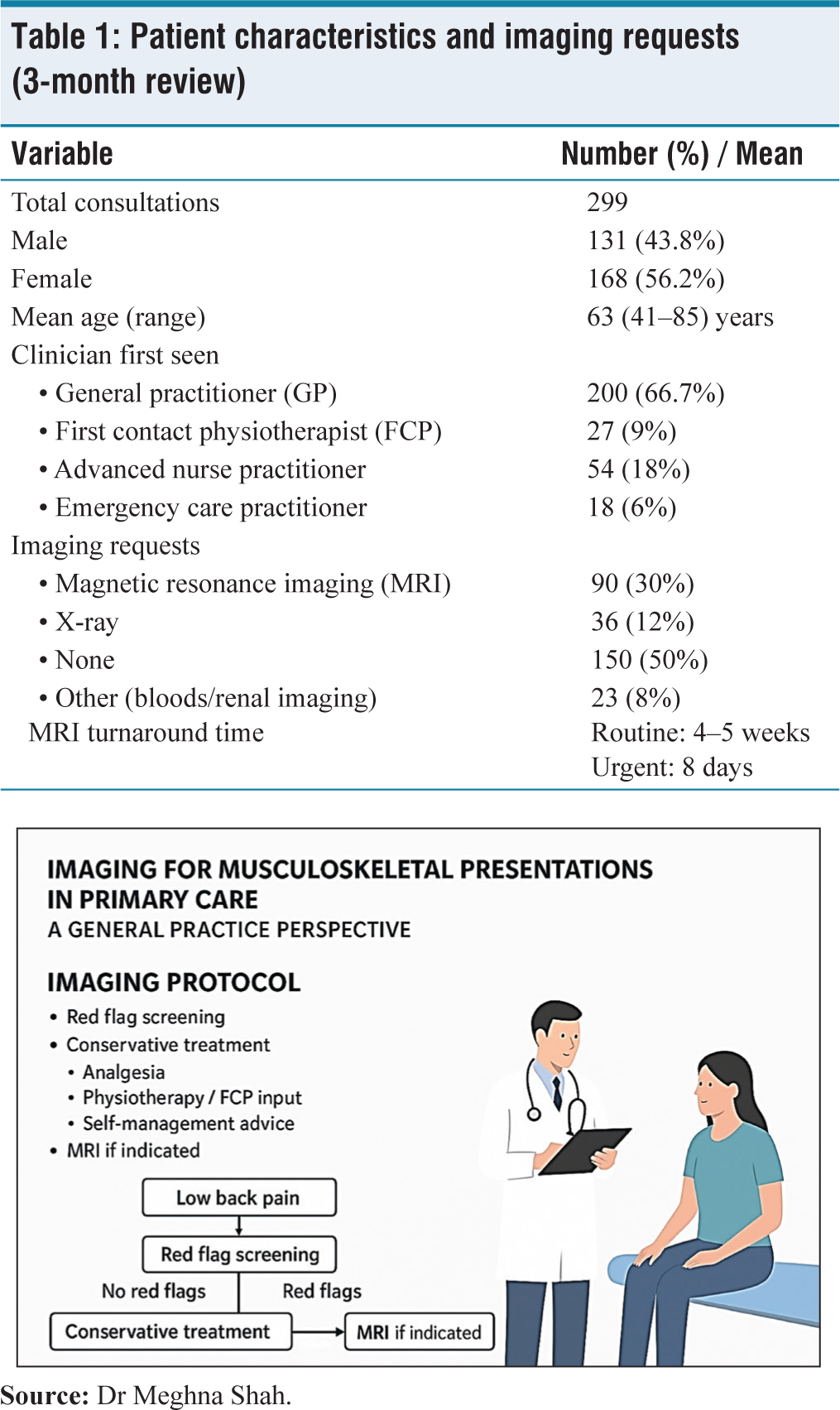
From a sample analysis: 66.7% of patients were initially seen by a GP; 9% by a FCP; 18% by an advanced nurse practitioner; 6% by an emergency care practitioner. Thirty percent of patients had an MRI requested by a GP; 12% had an X-ray, particularly in cases of thoracic pain or suspected osteoporotic fracture; approximately 50% had no imaging requested, as there was no clinical indication. Others underwent blood tests or renal imaging.
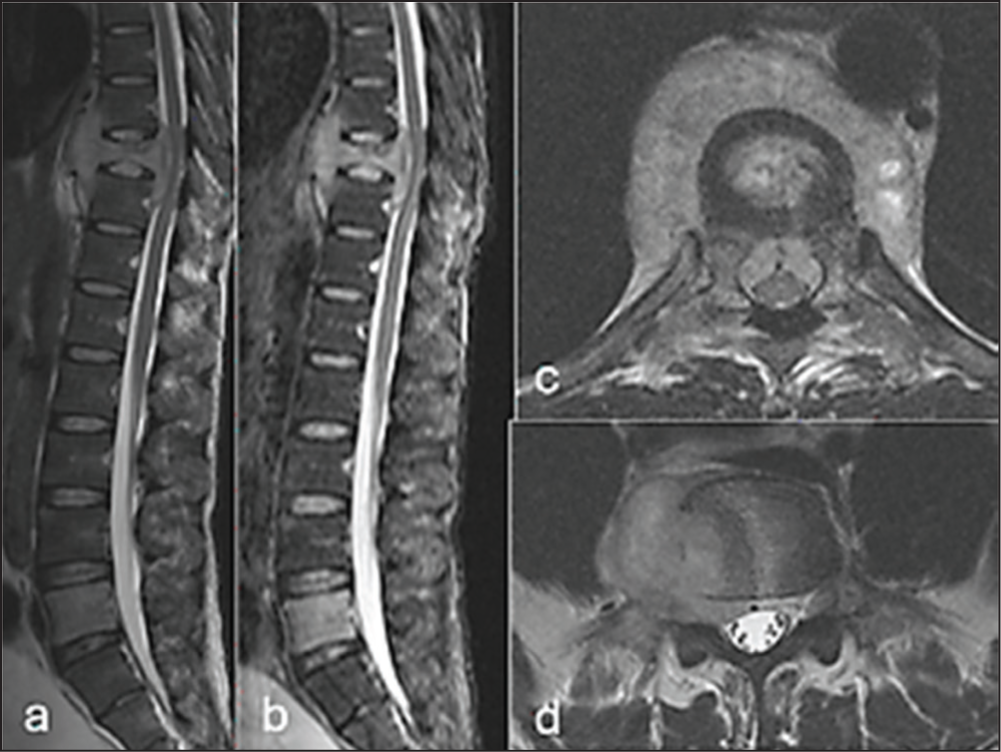
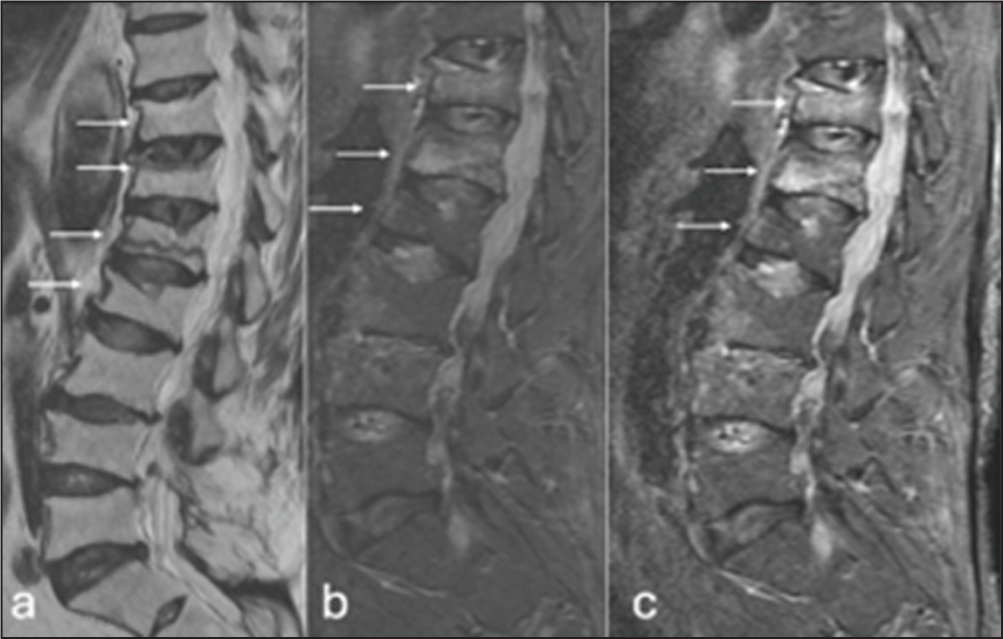
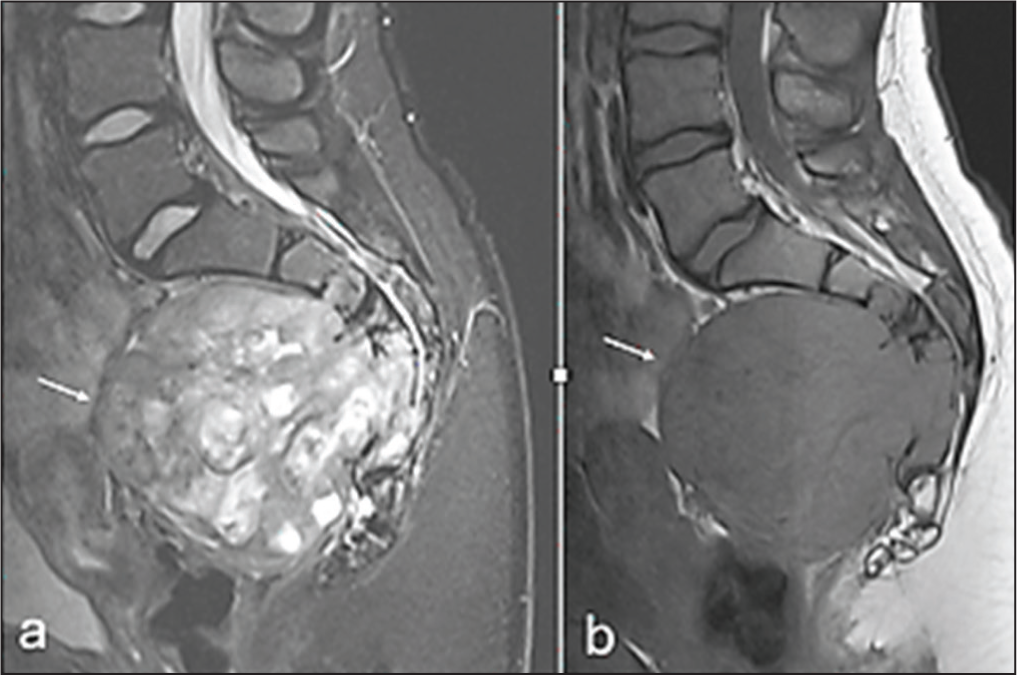
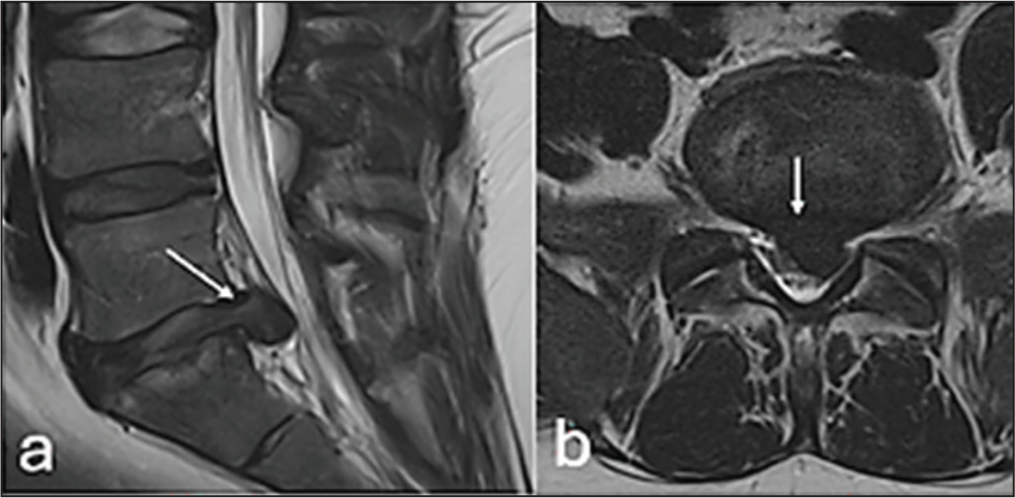
MRI turnaround times were approximately 4–5 weeks for routine requests and 8 days for urgent requests. Reported findings included degenerative disease, suspected discitis [Figure 1], osteoporotic fractures [Figure 2] and spondylosis.[7,8] Referrals to spinal surgeons were rare, with most patients managed using advice, analgesia and physiotherapy. Occasional referrals were made to pain management clinics.
FCPs were more likely than GPs to suggest structured home management programmes.
A limitation of the study is the small sample size that was analysed.
Literature review suggests that early MRI requests in the patient journey can save time, improve care and reduce costs, primarily by lowering secondary care referral rates.[7,8] However, when appropriate, referrals via extended physiotherapy services should be prioritised, as this may increase the diagnostic yield of MRI findings.[8]
MRI Reporting
Studies show that a substantial proportion of people without a history of LBP or sciatica may have abnormal imaging findings.[9–11] Mechanical compression of neural elements by disc herniation, as well as biochemical and inflammatory effects from nucleus pulposus contents, have been proposed as possible sources of LBP.[9,10]
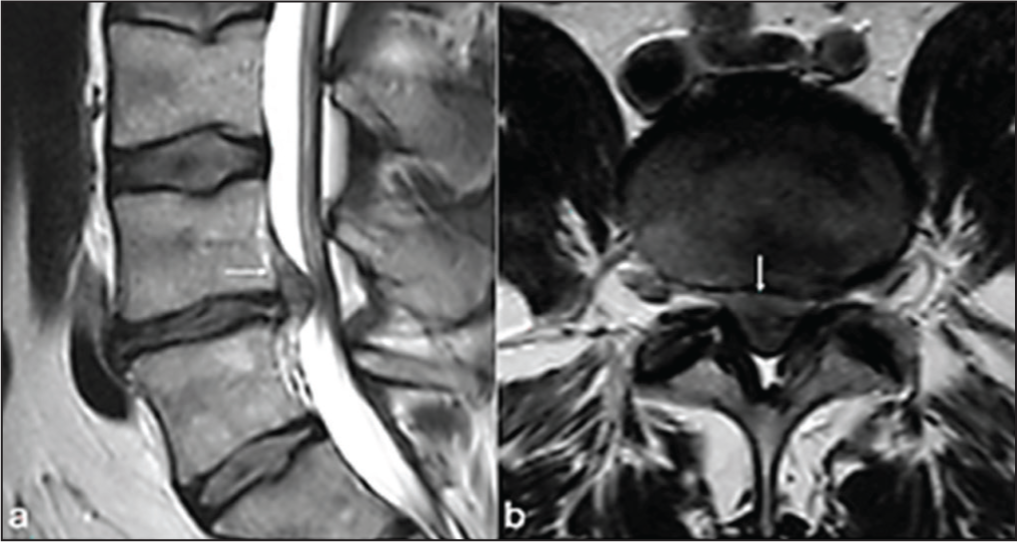
Therefore, caution is advised before attributing any particular anatomical finding as the definitive cause of a patient’s symptoms.[12] Radiologists recommend that potentially relevant MRI findings, such as disc abnormalities [Figure 3], the presence or absence of a high-intensity zone [Figure 4], end plate or marrow signal changes, the degree of nerve root compression [Figure 5] and facet joint degeneration, should always be described comprehensively.[11]
Conclusion
Back pain is often a self-limiting condition. MRI should be reserved for cases with severe or progressive neurological deficits or when serious underlying pathology is suspected. Increasing direct access to physiotherapists improves patient care by enabling early implementation of self-management strategies. It also ensures that subsequent imaging requests are more targeted and clinically appropriate. Access to MRI in primary care enhances patient outcomes through accurate signposting and reduced referrals to secondary care, particularly spinal surgery.
Footnotes
Acknowledgements
Dr Rajesh Botchu, The Royal Orthopaedic Hospital, Birmingham.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable.
Informed consent
Patient consent was waived because no patient-identifiable information was used.
Credit author statement
Meghna Shah: Conceptualisation, formal analysis, writing (original draft).
Anoushka Iyengar: Writing (review and editing).
All authors have read and agreed to the published version of the manuscript.
Data availability
Available on request.
Use of artificial intelligence
None.