
Abstract
Background:
Accurate pain evaluation in critically ill patients poses significant challenges, particularly when these patients are unable to communicate their experiences. The objective of the study was to evaluate the accuracy and interrater reliability of the Behavioural Pain Scale (BPS) and Critical Care Pain Observation Tool (CPOT) in pain assessment among patients on mechanical ventilator support.
Methods and Materials:
Twenty-six patients on mechanical ventilation in a tertiary care intensive care unit (ICU) were included in this cross-sectional study, and the level of pain was assessed at different states, such as during rest, positioning and suctioning, using both tools. The data was analysed using SPSS 20→ software.
Results:
Receiver Operating Characteristic (ROC) curve analysis showed that BPS and CPOT are equally sensitive during rest (0.488 vs. 0.473) and suctioning (0.581 vs. 0.57), while CPOT is more sensitive during positioning (0.687 vs. 0.575). However, BPS and CPOT are equally sensitive during rest with a high positive correlation and a moderate correlation during active procedures such as positioning and suctioning (P < .001).
Conclusion:
These findings conclude that pain assessment in mechanically ventilated patients is challenging. BPS and CPOT are equally reliable at a moderate level for pain assessment during rest and active interventions like suctioning and positioning. The study emphasises the need for targeted training and standardised criteria to improve interrater reliability, particularly during dynamic procedures, to enhance pain management in critically ill patients.
Keywords
Introduction
Pain is a common and often underappreciated problem in critically ill patients, particularly those who are intubated, sedated, or unable to communicate verbally. Effective pain management in this patient population is crucial, as inadequate analgesia can lead to a range of adverse physiological and psychological outcomes, including prolonged recovery, increased ventilator dependence, and the onset of post-traumatic stress disorder (PTSD).[1] Accurate pain assessment is key to ensuring appropriate interventions, but it remains a challenge in the intensive care unit (ICU) setting due to the inability of patients to self-report their pain.[2]
There are numerous tools for evaluating pain in adult ICU patients. The Critical Care Pain Observation Tool (CPOT) and the Behavioural Pain Scale (BPS) are the most commonly used.[3] CPOT was developed specifically for critically ill patients and includes categories such as facial expression, body movements, muscle tension and ventilator compliance.[4] It is particularly useful during active interventions and procedures that can provoke pain, such as suctioning.[5] In contrast, BPS is a simpler scale that includes facial expressions, verbal responses and guarding behaviours, and it is highly reliable during resting states and non-painful procedures.[6] However, both tools have been criticised for inconsistencies in interrater reliability, particularly in more dynamic situations.[7]
Despite their widespread use, there is limited research comparing the two tools directly, particularly in terms of their accuracy and interrater reliability across different clinical scenarios. This study aims to address this gap by comparing the CPOT and BPS in three clinical conditions: rest, non-painful procedures, such as body repositioning, and painful procedures like secretion suctioning. Understanding the strengths and limitations of each tool in different contexts will help optimise pain assessment and improve pain management practices in critically ill patients.
Methods and Materials
Study Design and Participants
The ethics committee clearance and the setting permission were obtained from the concerned authorities. This cross-sectional observational study was conducted in an ICU with a sample of 26 patients on mechanical ventilation. The sample size was calculated based on the study done by Gomarverdi et al.[8] with correlation ρ = 0.7, power = 90%, and α = 0.05; the calculated sample size was 20. A consecutive sampling technique was used to select the 26 patients in the ICU on a ventilator. The study purpose was briefed and a written consent was obtained for the voluntary participation from the patient, if they were able to communicate through writing or communication board or from the legally authorised relative, if not capacitated all patients aged between 18 and 65 years admitted to our ICU with an expected length of stay of more than 12 hours were included if they could not report their pain on their Individuals with progressive neuromuscular disorders, patients in need of paralysis, and those who were conscious were excluded from the study.
Data Collection Tools
The data regarding demographic and clinical variables of the patients were collected using the predetermined and pretested tools. Patients were assessed for pain using both CPOT and BPS during three distinct clinical scenarios: resting state (without any therapeutic procedures), positioning (non-painful procedure) and suctioning (painful procedure).
BPS is a more recently developed behavioural pain assessment tool used for critically ill patients[9] which includes three behavioural categories: facial expressions, (grimace, wince, neutral expression, closed eyes), verbal responses (moaning, verbal complaints) and muscle responses (rigidity, clenched fists), the score ranges from 0 to 3, with a total possible score between 0 and 9. Based on this scale, the patient’s status is classified as painless (0), mild (1–3), moderate (4–6), or severe (7–9) pain. CPOT includes four behavioural categories[10]: facial expressions, body movements, muscle tension and compliance with a ventilator (for intubated patients). Each category is scored from 0 to 2, with a total possible score ranging from 0 to 8. Based on this scale, the patient’s pain status is classified as painless (0), mild (1–3), moderate (4–6), or severe (7–8).
Data Collection Procedure
A trained expert nurse conducted the pain assessments using a checklist based on the CPOT and BPS during the three clinical scenarios. Pain scores were recorded, and the assessments were made simultaneously, starting with the BPS, followed immediately by the CPOT. To reduce interobserver variation, only one trained nurse performed all pain evaluations. The pain score was assessed for the selected patients during their ventilator days. A total of 100 observations were made.
Statistical Analysis
The collected data were analysed using SPSS version 20. Receiver Operating Characteristic (ROC) curve analysis was used to compare the accuracy of both tools in different clinical scenarios. Interrater reliability was assessed using Cohen’s kappa, which measures the level of agreement between raters. A kappa value of 0.0 indicates no agreement, while higher values indicate better agreement.
Results
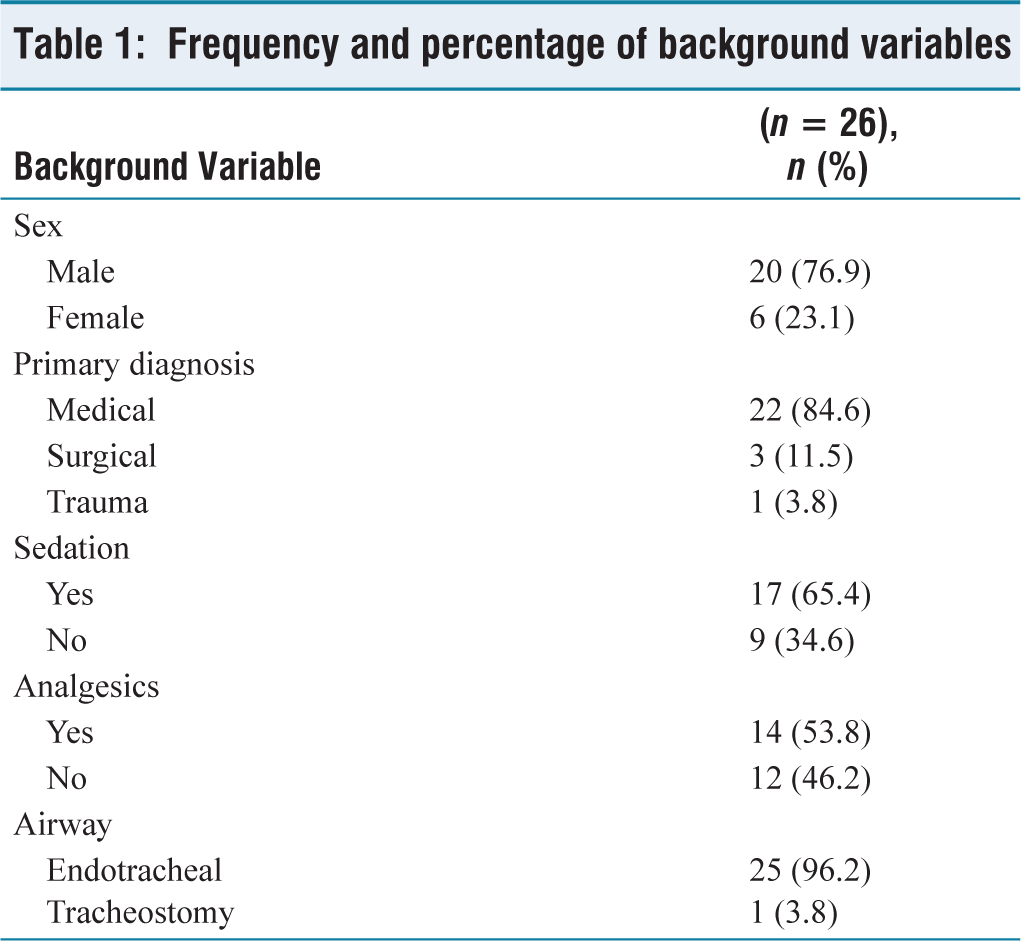
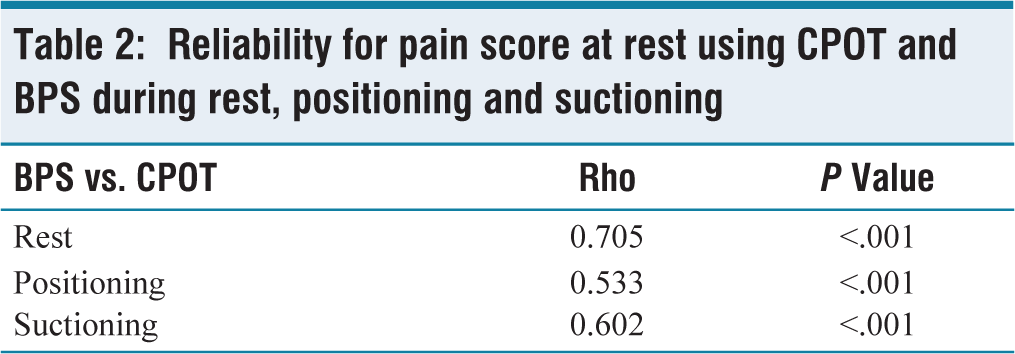
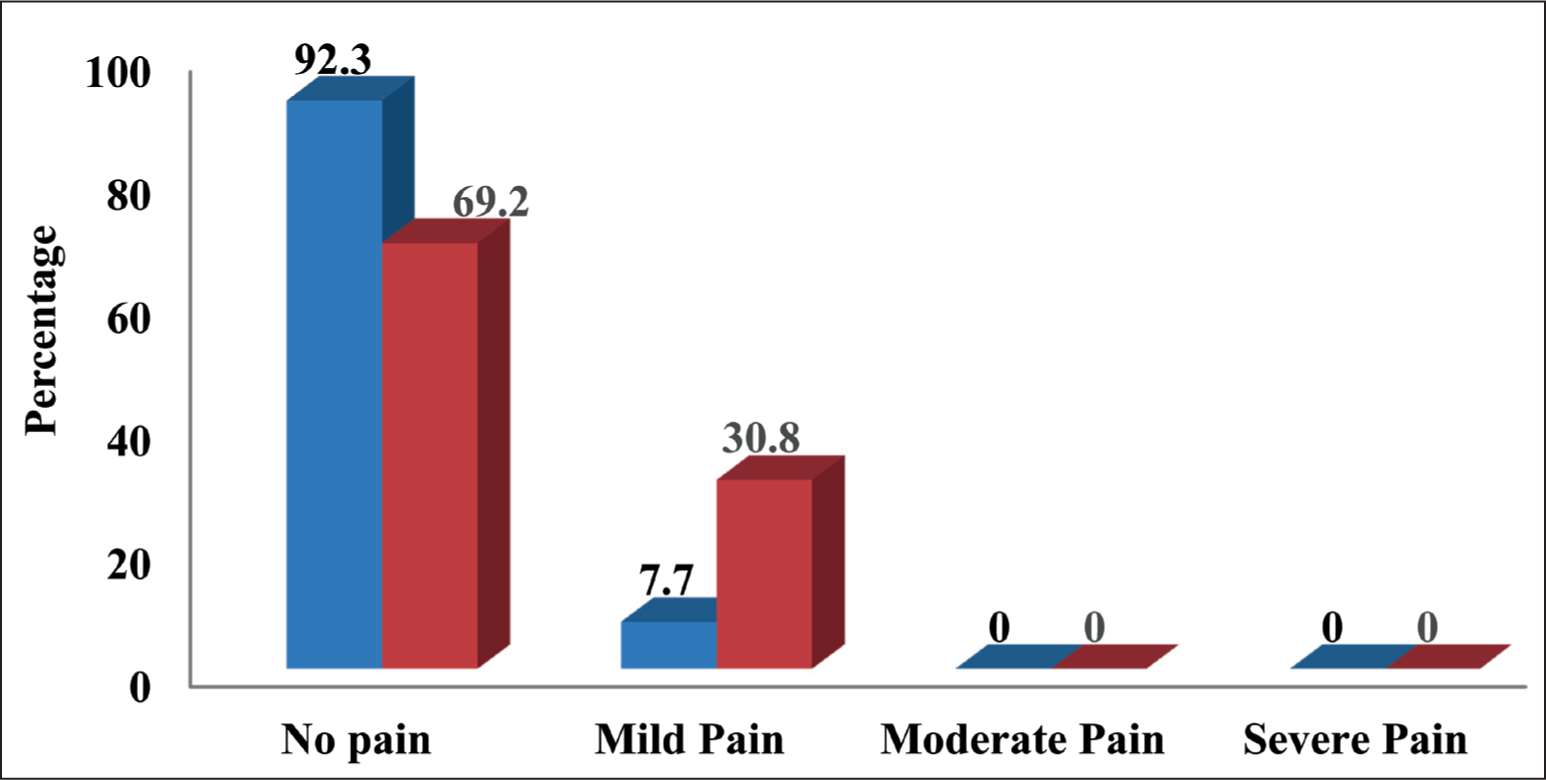
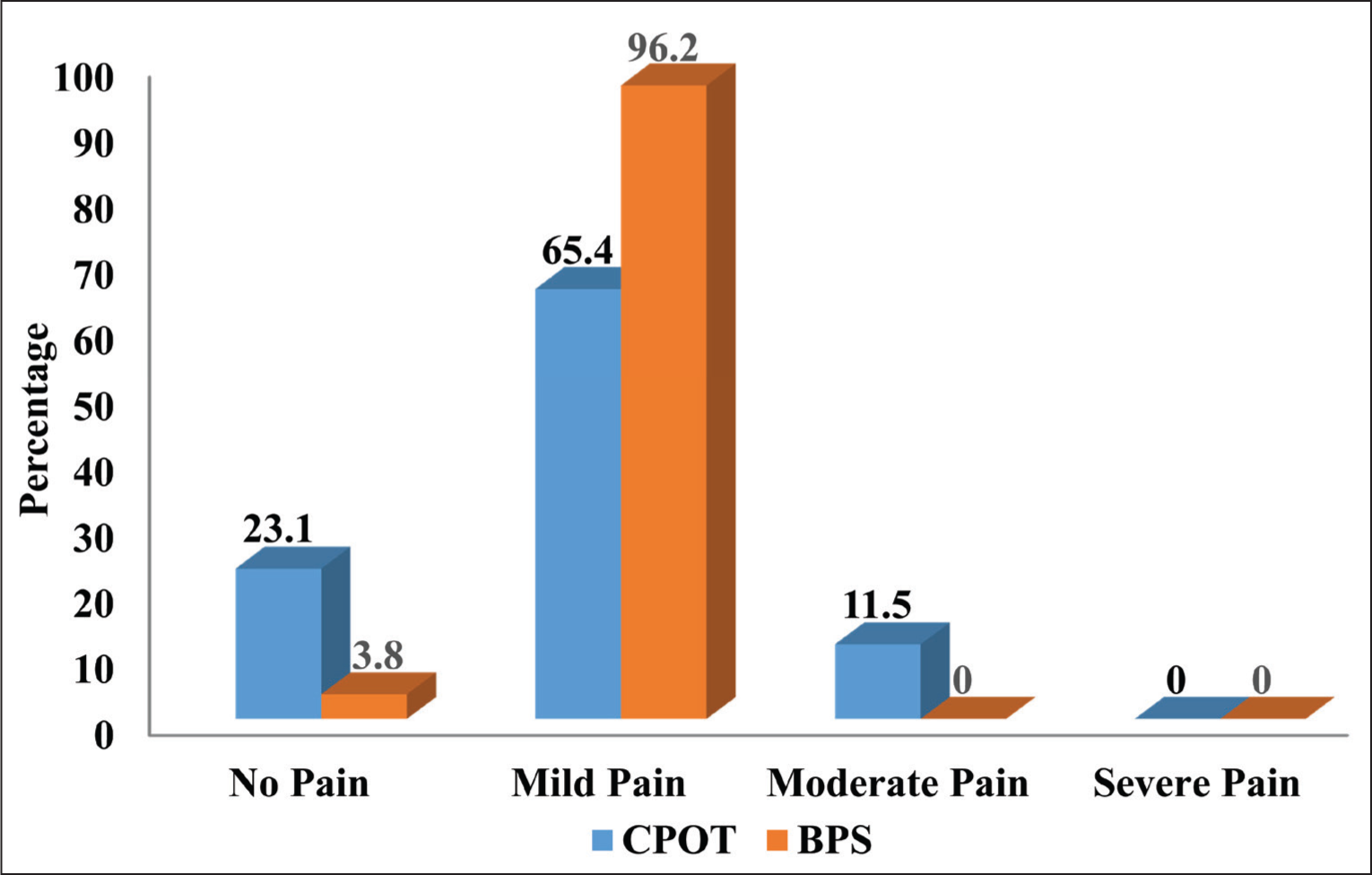
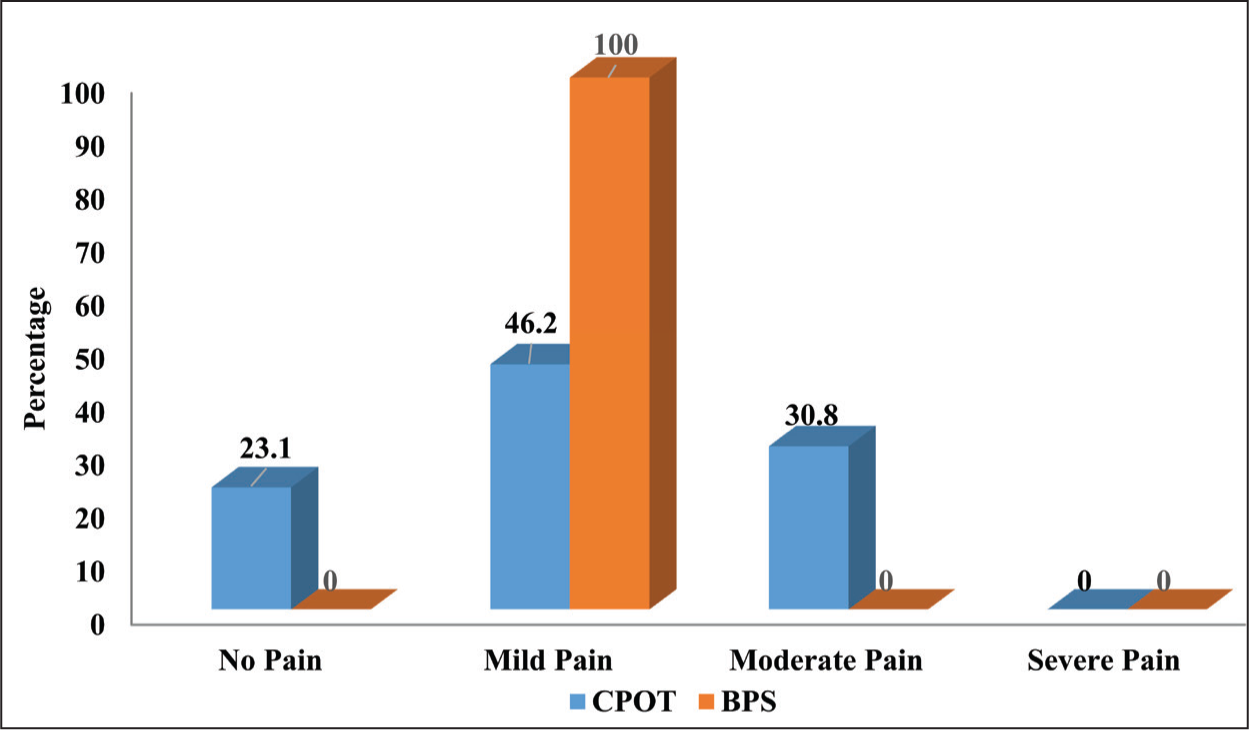
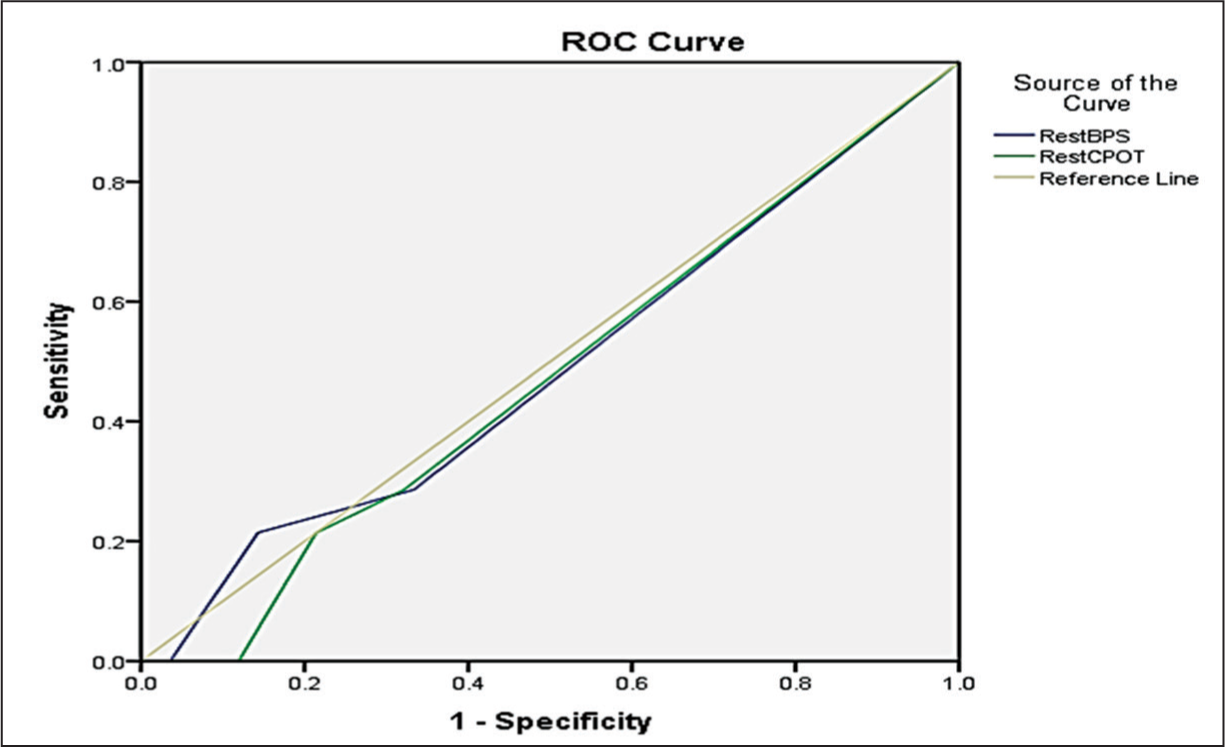
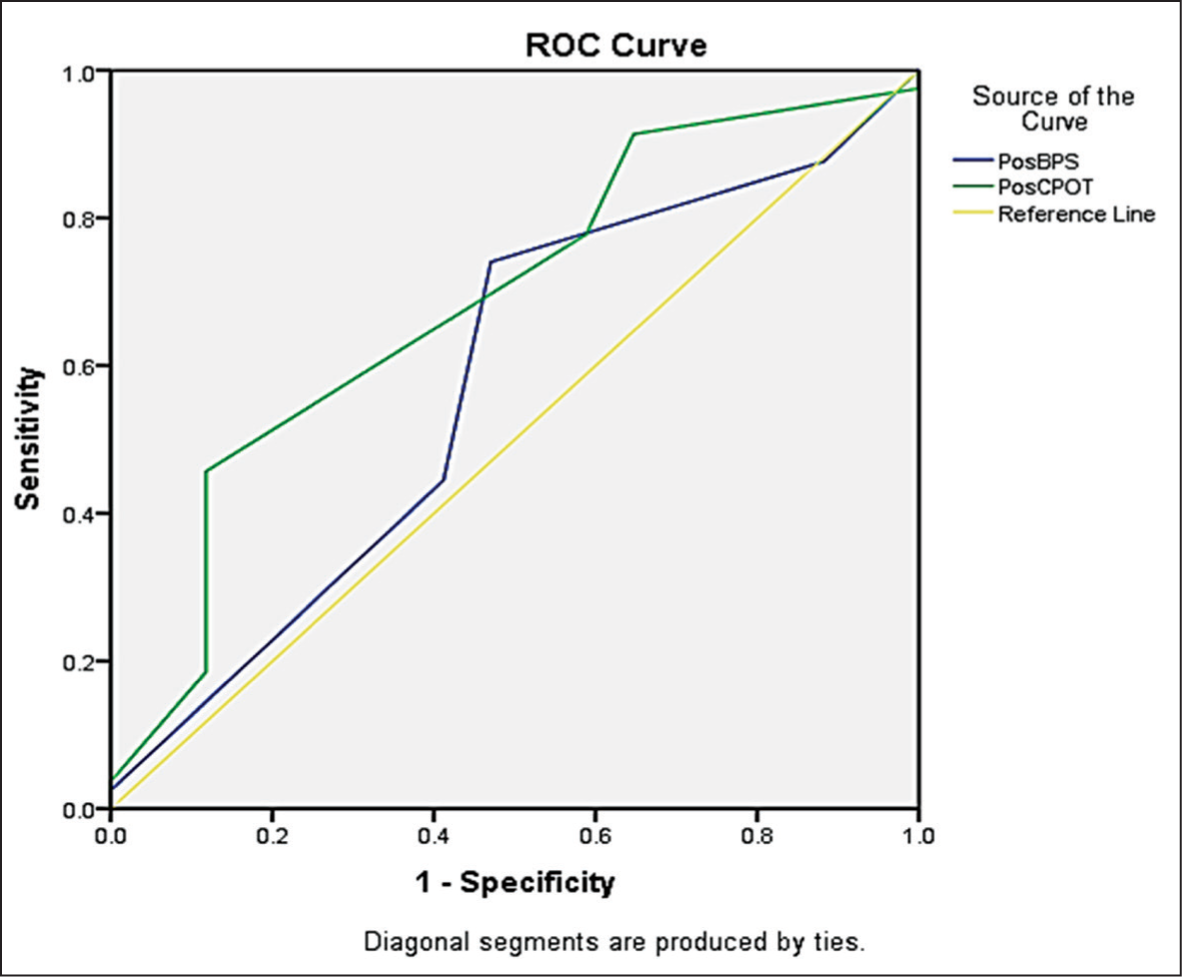
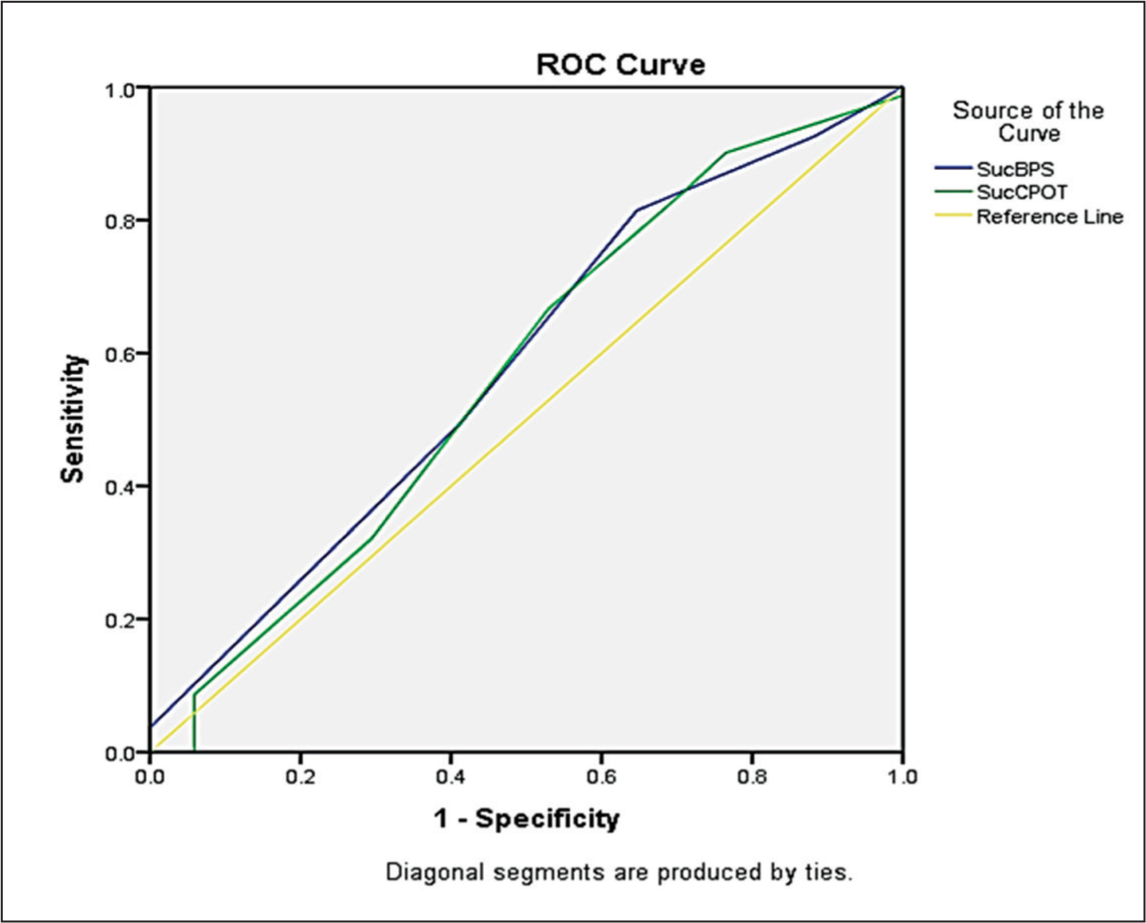
The study included 26 mechanically ventilated patients, predominantly male (76.9%), with most presenting medical diagnoses (84.6%) and receiving sedation (65.4%) and analgesics (53.8%). Nearly all patients (96.2%) were intubated with an endotracheal airway [Table 1]. A strong positive correlation was observed between the BPS and the CPOT at rest (ρ = 0.705, P < .001), with moderate correlations during positioning (ρ = 0.533, P < .001) and suctioning (ρ = 0.602, P < .001), indicating statistically significant agreement between the two tools across all conditions [Table 2]. In terms of pain intensity, CPOT recorded 92.3% of patients with no pain at rest, while BPS reported 69.2% as pain-free, and 30.8% with mild pain, suggesting that BPS may slightly overestimate pain in resting states [Figure 1]. During patient positioning, CPOT identified a range of pain intensities, including 11.5% with moderate pain, whereas BPS classified nearly all patients (96.2%) with only mild pain, failing to detect moderate pain levels [Figure 2]. Similarly, during suctioning, CPOT detected 30.8% of patients with moderate pain, while BPS recorded all patients (100%) as having mild pain, indicating a lack of sensitivity to variations in pain intensity [Figure 3]. The ROC curve at rest demonstrated that both tools had poor diagnostic performance, with curves lying close to the diagonal reference line, suggesting low discriminative ability and AUC values likely near 0.5 [Figure 4]. During positioning, CPOT showed superior diagnostic accuracy with an AUC of 0.687, compared to BPS with an AUC of 0.575 [Figure 5]. In contrast, during suctioning, BPS had a slightly higher AUC (0.581) than CPOT (0.570), though both exhibited only moderate accuracy [Figure 6]. These findings suggest that CPOT may be more sensitive and nuanced in detecting varying pain intensities during procedures, while BPS appears limited in differentiating pain levels under clinical stimulation.
Frequency and percentage of background variables
Reliability for pain score at rest using CPOT and BPS during rest, positioning and suctioning
Percentage distribution of the level of pain based on BPS and CPOT at rest
Percentage distribution of the level of pain based on CPOT and BPS during the position
Percentage distribution of the level of pain based on CPOT and BPS during suctioning
ROC curve to compare CPOT and BPS during rest
ROC curve to compare CPOT and BPS during positioning
ROC curve to compare CPOT and BPS during suctioning
Discussion
This research emphasises the subtle distinctions in the diagnostic efficacy and dependability of the CPOT and BPS pain assessment instruments for critically ill patients on mechanical ventilation. Assessing pain accurately in this demographic is particularly challenging due to many patients’ inability to communicate their pain levels. Consequently, the use of observational tools like CPOT and BPS becomes crucial. Both instruments showed a predictable rise in pain scores from resting states to more active interventions, such as patient repositioning and endotracheal suctioning. However, significant differences were noted in their sensitivity and discriminative abilities across different clinical situations. CPOT was able to discriminate more during positioning and BPS during rest and suctioning. This may be due to its inclusion of categories including physical movements and muscle stiffness, which are more relevant in active interventions. Both BPS and CPOT were found to be more reliable during the resting state and suctioning. The distinction between these two tools lies in their assessment criteria: the CPOT evaluates muscle tone and movements of both the arm and calf (representing the whole body), while the BPS focuses solely on upper limb movements.[11] While BPS and CPOT exhibited a strong correlation at rest (rho = 0.705), this correlation diminished to moderate levels during more dynamic clinical scenarios, such as positioning (rho = 0.533) and suctioning (rho = 0.602). This indicates that the agreement between the tools is more reliable when evaluating pain under low-stimulus or baseline conditions but diverges as the complexity or potential for discomfort increases. Importantly, CPOT consistently detected a broader spectrum of pain intensities across various procedures. For instance, during positioning, CPOT noted that 11.5% of patients experienced moderate pain, whereas BPS categorised 96.2% as having only mild pain. A similar pattern was observed during suctioning, where CPOT recognised moderate pain in 30.8% of patients, while BPS again classified all patients as experiencing only mild pain.
The ROC curve analysis supported these conclusions. At rest, both assessment tools showed inadequate diagnostic performance with AUC values close to 0.5, suggesting that neither tool effectively distinguished between pain and the absence of pain in this condition. This could be attributed to the naturally low variability in patient behaviour while at rest, which restricts observable indicators of pain. However, during positioning, CPOT exhibited enhanced accuracy with an AUC of 0.687—falling within the fair diagnostic utility range—compared to BPS, which had an AUC of 0.575, indicating only poor to moderate accuracy. In suctioning, BPS recorded a slightly higher AUC (0.581) than CPOT (0.570), although both scores remain within the moderate performance spectrum. Since AUC values approaching one signify excellent diagnostic performance and those near 0.5 indicate random chance, these results imply that CPOT is somewhat more effective in identifying subtle changes in pain behaviour, particularly during active clinical interventions.
These results are consistent with earlier studies, including the work of Severgnini et al.,[12] which found that while BPS was more specific (91.7%), CPOT demonstrated greater sensitivity (76.5%)—an essential characteristic in pain detection where underestimation can result in inadequate treatment. Additionally, the combination of both tools in that research increased sensitivity to 80.4%, highlighting the potential advantages of using integrated tools.
The study also noted greater interrater reliability at rest, where pain indicators tend to be more stable and criteria are easier to apply consistently. However, during dynamic procedures like positioning and suctioning, reliability decreased, likely due to heightened variability in patient responses and more subjective interpretation by evaluators. This variability underscores the urgent need for standardised application protocols and focused training for clinical personnel utilising these tools. Variations in tool design may also play a role in performance differences—CPOT includes assessments of muscle tension and body movement in both upper and lower limbs, whereas BPS primarily concentrates on upper limb and facial expressions. It is crucial to recognise that BPS’s potential underestimation of pain during suctioning and positioning could lead to inadequate analgesic interventions if used in isolation. Although the study endorses the use of CPOT for its superior performance in active situations, the consistent correlation between both tools still indicates the benefit of their combined or complementary use, especially when supported by trained personnel. The study is constrained by its relatively small sample size and the reliance on a single evaluator, which may introduce assessment bias and limit the generalizability of the results. Future studies should include a larger cohort with blinded multi-rater assessments to further validate tool performance and minimise observer bias.
Conclusion
Both the CPOT and the BPS serve as valuable instruments for assessing pain in non-communicative ICU patients; however, their diagnostic accuracy can differ based on the context. CPOT demonstrates greater sensitivity in identifying moderate to severe pain during active procedures such as patient positioning and suctioning. Conversely, BPS often underestimates pain intensity in these situations, even though it aligns closely with CPOT when patients are at rest. The assertion that both tools are equally effective for suctioning should be approached with caution, as BPS did not consistently identify moderate pain levels in all patients during this procedure.
To improve the effectiveness of pain assessment, clinical teams should emphasise the use of CPOT during painful interventions and offer specialised training on its implementation. The integration of both tools may enhance sensitivity and overall pain management within the ICU. Future research involving larger sample sizes and blinded, multi-rater evaluations is suggested to confirm these results and mitigate potential assessment bias.
Footnotes
Acknowledgements
To the Research Department, Apollo Main Hospital, Chennai.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Approval was obtained from the Institutional Ethical Committee on 20 August 2022.
Informed consent
Informed consent has been obtained from the patient’s family, who met the eligibility criteria.
Credit author statement
SS participated in conceptualisation, methodology, data collection, data analysis, literature search and manuscript preparation.
SD, RS, JJV and NR were involved in conceptualisation, literature search, validation, supervision and manuscript revision.
All the authors have reviewed and approved the manuscript.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author upon request.
Use of artificial intelligence
No Artificial Intelligence was used.