
Abstract
Background:
Paraesthesia, characterised by tingling or prickling sensations, typically results from nerve compression or injury. With smartphones becoming integral to daily life, young adults often maintain prolonged static postures that may compress peripheral nerves, particularly in the upper extremities. This study aimed to assess the prevalence of upper extremity paraesthesia among long-term smartphone users aged 15–35 years.
Aim of the Study:
To describe the prevalence and pattern of self-reported tingling or numbness in young adults and to explore associations with smartphone usage habits.
Methodology:
A cross-sectional online survey was conducted among 253 smartphone users aged 15–35 years in Ahmedabad, India. A self-designed questionnaire was pilot-tested for clarity and face validity. Data on demographics, device use (years, hours/day), posture, and paraesthesia (location, timing, severity) were collected. Descriptive statistics summarised symptom prevalence; associations were explored with chi-square tests.
Results:
Overall, 55.7% of respondents reported tingling or numbness in one or more upper extremity regions. The hand was most affected (26.1%), followed by little finger (22.2%), thumb (20.6%), ring finger (19.8%), middle finger (15.0%), and index finger (13.0%). Symptoms occurred primarily during (29.2%) or immediately after (10.7%) device use. Most described mild (24.5%) or moderate (17.0%) symptoms; severe and very severe reports were 2.4% and 2.8%, respectively. Associations reached statistical significance for daily usage duration and symptom presence (P < .05).
Conclusion:
More than half of long-term smartphone users in this sample experienced self-reported paraesthesia. Given the survey-based design and absence of clinical or electrophysiological confirmation, findings should be interpreted as preliminary. Future studies must incorporate objective diagnostic measures, validated symptom instruments, control groups, and control for occupational and activity-related confounders.
Introduction
Technology has become integral to modern life, reshaping how people communicate, work, and access entertainment. By 2020, an estimated 2.87 billion individuals owned smartphones, making them among the most ubiquitous electronic devices worldwide.[1,2] Beyond basic calling and messaging functions, smartphones now serve as multifunctional platforms for gaming, music, video streaming, and education.
Extensive research among adolescents and young adults has linked excessive smartphone use to poor postural habits, forward head tilt and chronic stooping that predispose users to musculoskeletal disorders.[3–6] Common complaints include neck and shoulder pain (‘text neck’) and De Quervain tenosynovitis, colloquially known as ‘smartphone thumb’.[7,8] Surveys suggest teenagers spend nearly 10 hours per day on social media via smartphones, with up to 8.4% of users meeting criteria for smartphone addiction.[3,5]
Physiological sequelae extend to cervical disc injuries, upper limb tingling, and carpal tunnel syndrome arising from sustained and improper hand postures.[7,8] While the musculoskeletal consequences of smartphone overuse are well documented, the neurological dimension, specifically upper extremity paraesthesia from potential median, ulnar, or radial nerve compression, remains underexplored.[6] It is unclear whether the tingling and numbness reported by users stem solely from repetitive strain and poor ergonomics or reflect an underlying predisposition to entrapment syndromes.
Emerging concerns about early-onset paraesthesia in young adults underscore the need for preventive strategies and early screening protocols. Significant research gaps persist: the specific mechanisms by which smartphone habits contribute to nerve compression; objective quantification of nerve dysfunction via conduction studies or imaging; and the development of evidence-based ergonomic guidelines. Future studies employing validated symptom scales, clinical diagnostics, and longitudinal designs are essential to establish causal links, define safe usage thresholds, and inform interventions aimed at preserving upper extremity health.
Aims and Objectives of the Study
Aim
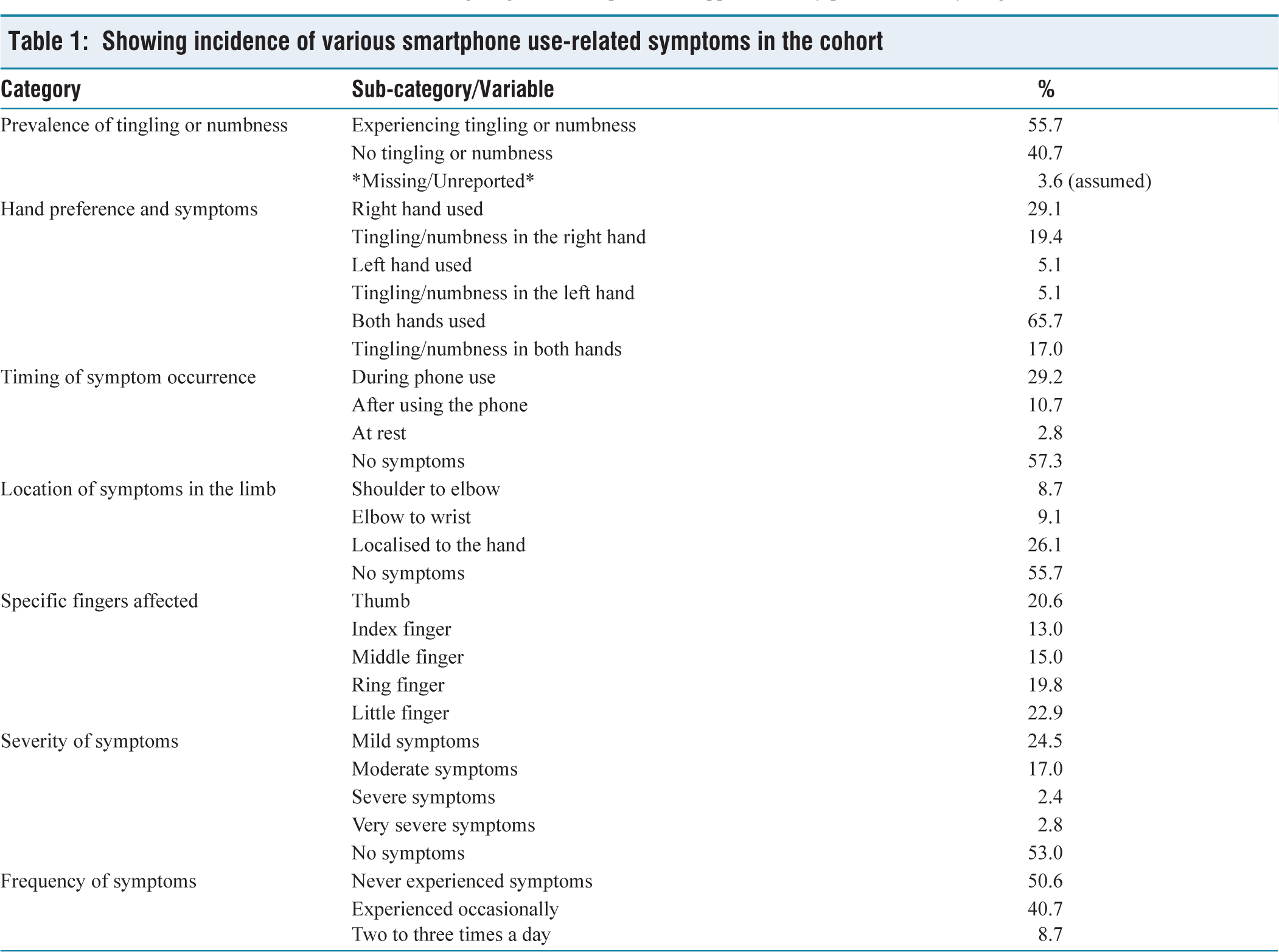
To evaluate the prevalence and pattern of upper extremity on self-reported tingling and numbness (paraesthesia) in young adults in relation to their smartphone usage habits, and to explore the possible involvement of peripheral nerve compression syndromes (refer to Table 1).
Showing incidence of various smartphone use-related symptoms in the cohort
Objectives:
To assess the frequency and intensity of upper limb paraesthesia in smartphone users aged 18-30. To examine the relationship between smartphone usage duration, posture habits, and neurological symptoms. To evaluate awareness and ergonomic practices among users regarding smartphone use.
This study seeks to highlight possible emerging health concerns smartphone-induced peripheral nerve irritation or compression, in young adults. By bridging the current knowledge gap, it aims to contribute evidence toward better understanding the early neurological impacts of smartphone use and to suggest practical approaches for prevention and management.
Materials and Methods
Study Design and Participants
Cross-sectional survey conducted over 3 months in Ahmedabad District, Gujarat, India.
Inclusion: 15-35 years old, smartphone use ≥6 hours/day, consented.
Exclusion: Known cervical radiculopathy, upper extremity surgery history, and neurological disorders.
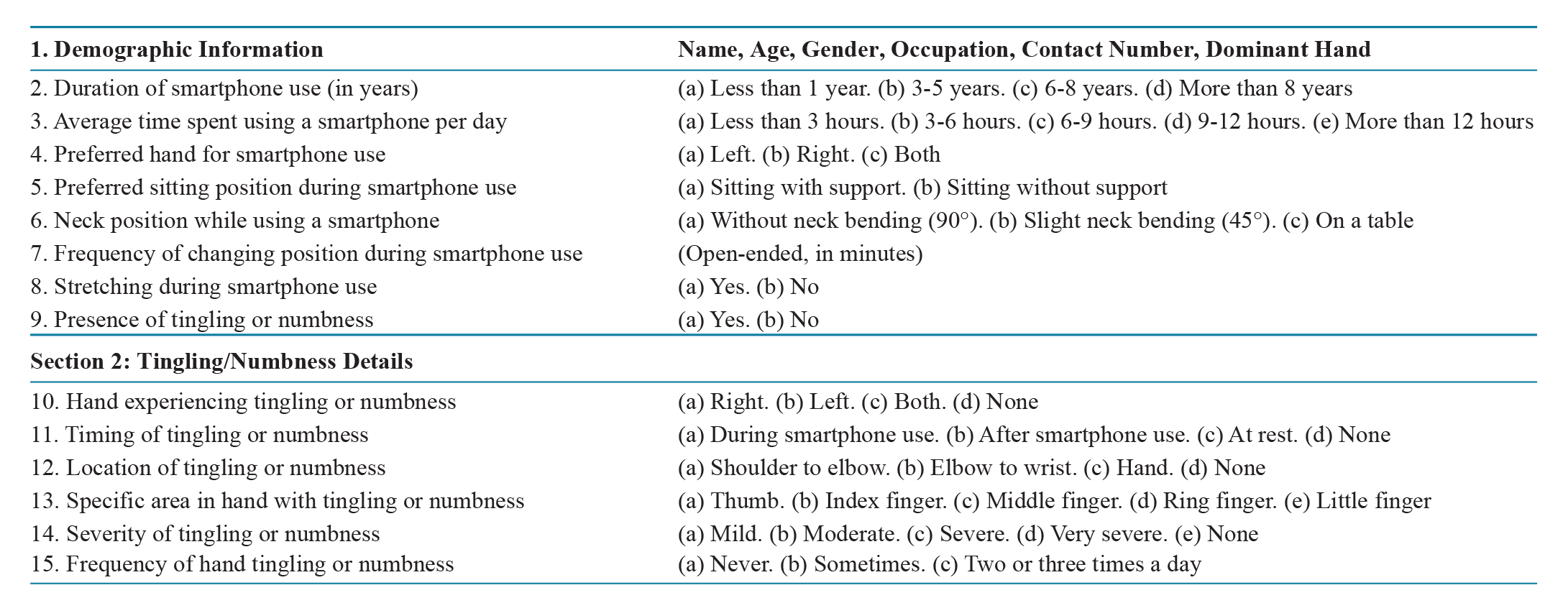
Survey Instrument
Developed by investigators; pilot-tested with 20 volunteers for clarity and face validity.
Sections:
Demographics (age, gender, hand dominance) Smartphone use (years, daily hours, posture, position changes) Self-reported paraesthesia (presence, timing, location, severity, frequency)
No clinical examinations, nerve conduction studies, or imaging were conducted.
Data Collection
Distributed via Google Forms link; 253 complete responses analysed.
Questionnaire
Statistical Analysis
Descriptive statistics for prevalence and patterns.
Chi-square tests examined associations between usage categories and symptom presence.
Significance set at P < .05.
Results
Participant Profile
Age: 71.5% (20–25 years), 15.0% (15–20 years), 9.1% (25-30 years), 4.3% (30–35 years).
Gender: 59.3% female, 40.7% male.
Dominance: 87% right-handed, 13% left-handed.
Smartphone Use Patterns
Years of use: 60.1% (3–5 years), 21.7% (6–8 years), 13.4% (>8 years), 4.3% (<1 year).
Daily hours: 49.4% (3–6 h), 22.1% (6–9 h), 6.7% (9–12 h), 3.6% (>12 h).
Posture: 85% slight neck bending; 62.2% elbow supported; 37.8% unsupported.
Paraesthesia Prevalence and Pattern
Overall symptom prevalence: 55.7%.
Most affected region: hand (26.1%).
Finger-specific: little (22.2%), thumb (20.6%), ring (19.8%), middle (15.0%), index (13.0%).
Timing: during use (29.2%), after use (10.7%), at rest (2.8%).
Severity: mild (24.5%), moderate (17.0%), severe (2.4%), very severe (2.8%).
Frequency: never (50.6%), sometimes (40.7%), two to three times/day (8.7%).
Association Analysis
Symptom presence increased significantly with daily use >6 hours (χ² = 8.12, P = .017).
Elbow-supported posture showed a non-significant trend toward fewer symptoms (P = .08).
Discussion
Over half of respondents reported tingling or numbness, suggesting a high prevalence of self-perceived paraesthesia in heavy smartphone users. Finger distribution aligns with the median and ulnar nerve territories. However, without clinical or electrophysiological confirmation, we cannot assert true nerve entrapment. Cross-sectional design, convenience sampling, and reliance on a non-validated questionnaire limit causal inferences and generalizability.
Comparable surveys in adolescents and university students have reported musculoskeletal and neurological discomfort, but objective nerve studies remain scarce. Our finding of greater symptom prevalence with higher daily use echoes prior work, yet the lack of a control group and confounder adjustment (occupation, physical exercise, comorbidities) restricts interpretation.
Previous research has shown that prolonged smartphone and handheld device usage is associated with postural, musculoskeletal, and neurological disorders, especially affecting the neck and upper limbs.[9] Studies have linked sustained elbow flexion at approximately 90 degrees—common during smartphone use while seated or lying down—with an increased risk of ulnar nerve neuropathy, characterised by numbness in the ring and little fingers.[9,10]
P. P. Shah conducted a study on physiotherapy students, establishing a link between smartphone addiction and musculoskeletal problems such as text neck syndrome and SMS thumb, resulting in neck and hand discomfort.[11] Similarly, Loveria Sekarrini reported that 31.4% of adolescents aged 15-24 years experienced wrist pain, and 67.8% reported tingling or numbness in the hand due to excessive smartphone usage.[12]
Future research should aim to incorporate objective clinical evaluations in addition to self-reported questionnaires to strengthen the findings. Long-term prospective studies and ergonomic intervention trials may help in further understanding and preventing smartphone-related upper extremity paraesthesia.
Despite its significant findings, this study has some limitations. The cross-sectional design restricts the ability to establish causality between smartphone use and symptoms. Additionally, reliance on self-reported data might introduce recall bias. However, a major strength of this study is its relatively large sample size and its focus on a young adult population, which is highly relevant given the increasing smartphone dependency in this age group.
Limitations of the study:
Survey-only design. No clinical examinations, nerve conduction studies, or imaging to confirm neuropathy. Instrument validity. The questionnaire lacks formal psychometric validation. Sampling bias. Non-probability convenience sample; no control group. Self-report bias. Potential recall and reporting inaccuracies. Confounders. Did not adjust for occupation, physical activity, or preexisting conditions.
Conclusion
This preliminary survey indicates that young adults engaging in prolonged smartphone use frequently report upper extremity paraesthesia. Given methodological constraints, these findings should be viewed as hypothesis-generating rather than confirmatory. Future research must employ validated symptom scales, objective diagnostic criteria (clinical exam, nerve conduction studies), randomised sampling with control groups, and multivariable analyses to delineate true associations and inform ergonomic guidelines.
Footnotes
Acknowledgements
The authors thank Ahmedabad Physiotherapy College, Parul University, for providing the No Objection Certificate to carry out the study outside the college premises.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
This study was approved by the Institutional Ethical Committee of the college.
Informed consent
All participants provided written informed consent prior to their inclusion in the study. The study protocol was reviewed and approved by the Institutional Ethics Committee. Refer annexure in attachment.
Credit author statement
All authors contributed to the conception, design, data acquisition, and drafting of the manuscript. All authors read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Credit information
Name(s) of Department(s) and/or Institution(s) to which the work should be credited: Ahmedabad Physiotherapy College, Parul University.
Data availability
The datasets generated and analysed during the current study are available Refer annexure in attachment.
Use artificial intelligence
No AI tool was used in research.